
Case Report | DOI: https://doi.org/10.31579/2640-1053/142
1 Unidad Medica Onco-hematologica, Puebla, Mexico.
2 Hospital General de Zona No. 01, Instituto Mexicano del Seguro Social, Hidalgo, Mexico.
3 Department of Oncology, Medicine School, Benemerita Universidad Autonoma de Puebla, Puebla, Mexico.
4 Hospital Universitario de Puebla, Benemerita Universidad Autonoma de Puebla, Puebla, Mexico.
5 Hospital Angeles Puebla, Puebla, Mexico.
6 Unidad Medica de Alta Especialidad Manuel Avila Camacho, Instituto Mexicano del Seguro Social, Puebla, Mexico.
7 Hospital Guadalupe, Puebla, Mexico.
*Corresponding Author: Salvador Macias-Diaz, Unidad Medica Onco-hematologica, 7 sur 4515, Puebla, Puebla, Mexico.
Citation: Salvador M. Diaz., Karina C. Guerrero., Eduardo T. Bernal., Andrea C. Sanchez., Ixel E. Lopez., et all (2023), Breast Melanoma, a Disease Unsuspected by the Oncologists: Presentation of a Case Report and Review of the Literature, J. Cancer Research and Cellular Therapeutics. 7(1); DOI:10.31579/2640-1053/142
Copyright: © 2023 Salvador Macias-Diaz. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 April 2023 | Accepted: 05 May 2023 | Published: 12 May 2023
Keywords: breast cancer; melanoma; triple-negative; poorly differentiated tumor; immunohistochemistry
Breast melanoma is a rare disease, with a clinical and histopathological presentation like usual breast carcinoma. We present the case report of a 40-year-old woman with the initial diagnosis of triple-negative breast carcinoma with a poorly differentiated tumor, she received neoadjuvant chemotherapy with anthracyclines and taxanes with no response, subsequently received carboplatin with a slight decrease in tumor size and surgery was possible, the histopathological report of the modified radical mastectomy with more extensive immunohistochemistry concluded melanoma, due to the delay in delivery of the pathology result, she was not a candidate for adjuvant immunotherapy due to extemporaneity. The breast melanoma is an uncommon disease, so it must be suspected in a tumor with a poorly differentiated histological grade and in the absence of response to chemotherapy, therefore, a larger immunohistochemical panel is suggested to have a more specific diagnosis.
Breast melanoma is a rare entity, it can originate in the breast or be a metastasis from another site, representing 0.5 and 2.7% of all malignant breast tumors, respectively. It manifests as a firm and mobile mass [1], may or may not affect skin [2] and it can invade regional lymph nodes, which is why it is often indistinguishable from breast carcinoma [1]. Primary melanoma of the breast without an apparent lesion on the skin is a controversial issue, since its pathogenesis is debated, arguing that it could originate from ectopic melanocytes; however, some authors believe that it is a metastatic disease of an undiscovered primary [3]. Mammography, breast ultrasound, magnetic resonance imaging, computed tomography (CT), and positron emission tomography computed tomography may be useful for its study, however, biopsy with immunohistochemical markers (tyrosinase, Melan-A/Mart-1, MITF, S -100, HMB-45, BRAF-V600E, vimentin) is the ideal method to confirm the diagnosis [1]. Lymph node status is the most important prognostic indicator. Its main treatment is surgical resection, with a combination of radiotherapy and systemic oncological therapy [4]. Staging and surgical treatment follow the guidelines for usual breast carcinoma [1], including the possibility of performing conservative surgery with sentinel node biopsy, but with the recommendation of surgical margins of up to 2 cm [2,4], breast reconstruction surgery being permissible [5], while systemic cancer treatment follows the guidelines recommended for melanoma, with the use of immunotherapy or target therapy against BRAF [1].
We present a 40-year-old woman treated at a public hospital in Mexico, with a family history of cancer, mother with colon cancer, brother with neck cancer, paternal uncle with lung cancer, paternal cousin with head cancer, cousin with cancer in the lumbar region, cousin with bladder cancer. The patient arrived at the Oncology clinic in January 2022 with a diagnosis of clinical stage IIIB left breast cancer with a 5.5 cm fungoid tumor and a 6 cm fixed left axillary conglomerate. The initial biopsy reported poorly differentiated infiltrating canalicular carcinoma, immunohistochemistry was performed for breast cancer with estrogen receptors, progesterone receptors and HER2 negative. She started treatment with neoadjuvant chemotherapy with epirubicin and cyclophosphamide every 21 days for 4 cycles, continued with docetaxel every 21 days for 4 cycles [6,7], with no response, however, due to the lack of surgical time in the hospital, another 4 cycles of docetaxel were continued presenting loco-regional progression, for which treatment was modified to 1 cycle of gemcitabine and carboplatin [8], presenting a slight decrease in tumor size and being able to perform a modified radical mastectomy on October 28, 2022 (Figure 1).

Figure 1: Left modified radical mastectomy.
In January 2023, still without having the mastectomy pathology report, we decided to start with adjuvant capecitabine [9], and she was referred to Radio-oncology to evaluate treatment. In April 2023, the histopathological report with complete immunohistochemistry was
finally collected which reported invasive, nodular, ulcerated melanoma, measuring 7 cm, Breslow 40 mm, 4 mitosis / mm2, with lymphovascular invasion, with 3 of 18 nodes removed with metastases and with tumor 1.5 cm from the nearest surgical margin (Figure 2).
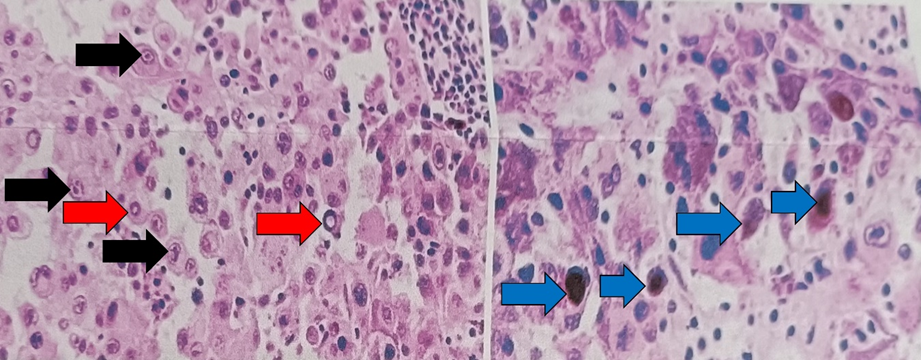
Figure 2: Neoplasm with epithelioid cells with marked atypia, pseudoinclusions (red arrow), intracytoplasmic melanin (blue arrow) and prominent nucleolus (black arrow).
CT scan from April 2023 without data on tumor activity. Based on these results, we decided to discontinue capecitabine and continue monitoring, we did not consider adjuvant immunotherapy because more than 22 weeks had passed since surgery [10], we are still awaiting evaluation by Radio-oncology.
Breast melanoma is a rare disease, there is a record published since 1959 by Stephenson et al., with a patient with metastatic breast melanoma only receiving palliative surgical treatment due to the lack of effective systemic therapy in those years [11]. In the hospital where the case report patient was treated, immunotherapy is available, nivolumab for example. Unfortunately, there is no immunohistochemistry panel for melanoma, so the tissue is sent to other reference medical units to complement the histopathological reports, however, the delivery time is delayed, this prevented indicating adjuvant immunotherapy because it was considered extemporaneous. Primary and metastatic breast melanoma may resemble poorly differentiated triple-negative breast cancer on initial biopsy because additional immunostains are not usually performed to differentiate between triple-negative breast carcinoma from melanoma or metaplastic carcinoma, therefore, the differential diagnosis of breast melanoma should always be considered in the presence of a poorly differentiated tumor [12]. In the case report, we considered that it was sufficient to be able to start neoadjuvant chemotherapy treatment, having a histopathological report of carcinoma with triple negative immunohistochemistry. Cases have been reported in which the first biopsy of the breast tumor refers to invasive ductal carcinoma, but when performing a second biopsy of an adjacent tumor, melanoma is reported, so performing immunohistochemistry is very useful for the definitive diagnosis [13]. Unfortunately, on some occasions, a metastatic melanoma can lose immunohistochemical melanocytic markers and can express GATA3 and cytokeratin, further confusing the diagnosis [14]. Tumors with a mixed component (carcinoma and melanoma) or "collision tumor" have also been described in the primary breast tumor and in its metastases [15, 16]. This could be due to the bidirectional genetic association between breast cancer and melanoma, since patients with a predisposing mutation for breast cancer, such as BRCA2, also have a higher risk of melanoma, while those with mutations of susceptibility to melanoma, such as the CDKN2A gene, present an increased risk of breast cancer [17, 18]. Another theory is that both neoplasms share a divergent monoclonal origin [4, 19]. In the patient, we considered that her tumor was not a "collision tumor" nor of a shared monoclonal origin and that the difference between the initial biopsy report and the mastectomy report was due to a more extensive immunohistochemical panel. There is a case report of a patient with metastatic triple-negative breast carcinoma who, after receiving chemotherapy and target therapy including bevacizumab and lapatinib, presented a new metastasis with histopathological characteristics of melanoma with expression of S-100, HMB-45 and Melan-A in immunohistochemistry, which raises the possibility of neoplastic transformation [20], we also do not consider that this has happened with the patient, since she only received treatment with chemotherapy, without developing metastases. The etiology of breast melanoma is not completely known, associations with exposure to ultraviolet solar radiation, skin pigmentation, sun sensitivity, and many nevi have been reported (21), or it may originate from a burn scar [22] or tattoos [23]. In the case of the patient, these risk factors were not investigated, because we did not initially suspect breast melanoma, although she did not have burn scars or tattoos in the breast region. Multiple case reports indicate the left breast as the most frequent location [15, 24], predominantly in upper quadrants, probably due to sun exposure [12, 21]. The patient's tumor is consistent with laterality, but the tumor was in the lower outer quadrant. Breast melanoma is a disease that must be evaluated by a multidisciplinary team. Due to the few published cases, we consider that the treatment should combine the recommendations of the international guidelines for breast cancer and melanoma, in non-metastatic stages consider initial surgery and later evaluate adjuvant radiotherapy and systemic treatment with immunotherapy or anti-BRAF. In patients with a large-volume tumor and/or significant regional involvement with little probability of complete removal of the tumor, without reaching the required surgical margins, we suggest systemic neoadjuvant treatment.
The breast melanoma is a disease unsuspected by the Oncologist, which assimilates to a triple negative breast carcinoma in its clinical and histopathological presentation, so it must be suspected in a tumor with a poorly differentiated histological grade and in the absence of response to chemotherapy. Therefore, a larger immunohistochemical panel is suggested to have a more specific diagnosis, for which clinicopathological correlation is the most crucial step towards to the correct interpretation and adequate clinical management.
Consent for publication
Informed consent was obtained from the patient.
Availability of data and materials
The datasets used and/or analyzed are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
There was no funding for this study.
Authors' contributions
Salvador Macias-Diaz is the Clinical Oncologist who indicated the chemotherapy treatments to the patient and collected all the patient's clinical history, he also participated in the design, writing, editing and review of the final manuscript. Karina Cruz-Guerrero participated in the data collection and analysis, she also participated in the design and writing of the final manuscript. Andrea Castro-Sanchez, Ixel Escamilla-Lopez, Eduardo Tellez-Bernal, Maria de Jesus Gonzalez-Blanco, Jose Gustavo Nuñez-Cerrillo, Cynthia Shanat Cruz-Medina and Jose Maria Ortega-Solar analyzed the data and reviewed the literature.
Not applicable.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
