
Research Article | DOI: https://doi.org/10.31579/2690-1919/262
1 Professor and Head, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy
2 Senior Consultant Physician No. (1) Defence Services General Hospital (1000-Bedded)
3 Lecturer, Department of Medicine, Defence Services Medical Academy
4 Consultant Physician, No. (1) Defence Services General Hospital (1000-Bedded)
5 Consultant Endocrinologist, No. (1) Defence Services General Hospital (1000-Bedded)
6 Consultant Haematologist, No. (1) Defence Services General Hospital (1000-Bedded)
7 Consultant Nephrologist, No. (1) Defence Services General Hospital (1000-Bedded)
*Corresponding Author: Khin Phyu Pyar, Professor and Head, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy
Citation: Khin Phyu Pyar, Thurein Win, Aung Phyoe Kyaw, Zar Ni Htet Aung, Nyan Lin Maung,et al. (2022). The EULAR 2022- What Is new? A lesson about Belimumab Therapy and Pregnancy with Autoimmune Rheumatic Diseases, J. Clinical Research and Reports, 11(5) DOI:10.31579/2690-1919 /262
Copyright: © 2022 Khin Phyu Pyar, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 September 2022 | Accepted: 29 September 2022 | Published: 11 October 2022
Keywords: break through infection (BTI); covid-19; breakthrough hospitalization; vaccination; health care workers (HCW); co-morbidity; survivors
Background: Coronavirus disease 2019 (COVID-19) has been threatening the world for more than 2 years. Breakthrough COVID-19 infection has clinical and public health significance. The health care workers have been working in front line; thus, acquiring greatest risks. Their family members are also at high risk being close contact to them. This study aimed to assess the prevalence and the severity of breakthrough COVID-19 infection (BTI) in fourth wave among health care workers (HCW) and their family members, and the protective effect of C OVID-19 vaccine in Myanmar.
Methods: A cross-sectional descriptive study was conducted among health care workers (HCW) and their family members who developed confirmed COVID-19 infection either by rapid test or PCR test at least 14 days after receiving COVID-19 vaccine during the fourth wave from January 2022 to May 2022. Data were collected by using standardized forms and analysis was done.
Results: A total of 1013 participants were included in this study; 227 HCW and 786 family members. Less than half of HCW 44.4% (101/227) and 17.1% (135/786) of family members suffered BTI in fourth wave. Among them, 95% (96/101) of HCW and 57% (76/135) of family members had at least 3 doses of vaccine. The the chances of getting BTI after taking 3 doses, 4 doses and 5 dose were 47.4%, 36.1% and 10% respectively in HCW; and, 32.8%, 22.4% and 1% respectively in the family members. The mean duration of last dose of vaccine to symptom onset was 45.9 ± 40.6 days in HCW and 60.7 ± 66.6 days in the family members. The proportion of different types of vaccine received by HCW were Covaxin 88%, Sinopharm 70%, Covishield 34% and Sputink V 30% whereas the proportion in their family members were Covaxin 27%, Sinopharm 68%, Covishield 56% and Sputink V 13%. Comorbid status was noted in 15% of HCW and 45% of family members. The prevalence of breakthrough hospitalization was 3 (3.1) HCW and 8 (6.4%) family members. The survival rate was 100% in HCW and 97% in family members. Non survivors were over 65 years and they had multiple comorbidities. Half of them received only 2 doses of vaccine; one was unvaccinated.
Conclusions: The majority of cases with BTI in fourth wave was mild. The prevalence of breakthrough hospitalization was 3-6% in HCW and family members; showing the protective effect of vaccine from severe manifestation. Non-survivors were elderly, having multiple comorbidities and incomplete vaccination or unvaccinated. The chance of BTI was decreasing if they obtained 4 doses compared to 3 doses. The possibility of BTI after taking 3 doses of vaccine was 50% in HCW and 33% in family members; it dropped to 36% and 22% respectively after 4 doses of vaccine. Therefore, 3 doses of COVID-19 vaccine could protect 50-67 percent; the protective efficacy increased to 65-87 percent with 4 doses. Therefore, 4 doses of COVID-19 vaccine are recommended for prevention of fifth wave in Myanmar.
In Myanmar, the total population was estimated at 54.05 million in 2019, with about 70% of the population resided in rural areas (United Nations Population Division, 2021). Fourth wave began in January 2022 and reached peak in March. As of March, 2022, the total number of daily new confirmed cases was nearly 2,000 (WHO, 2022b).
Vaccine program has been launched in Myanmar since January 2021; Covaxin and Covishield were the two main vaccines available initially. Later, Sinopharm, Sinovax, Sputink and Moderna has been accessible. First, two doses were given with the interval of 4-6 weeks. All the HCW were considered as at risks group and given vaccination in priority group; first dose of vaccine in January/February 2021 and second dose in March/April 2021. Third and fourth doses were given 5-6 months apart depending on availability of vaccine. As of early April 2022, 50% of total population of Myanmar got one dose; and, 40% of total population received 2 doses of vaccine (MOHS, 2021).
Covaxin is whole-virion inactivated SARS-CoV-2 vaccine; it uses a complete infective SARS-CoV-2 viral particle consisting of RNA surrounded by a protein shell, but modified so that it cannot replicate (Robertson S, 2020). Various studies on Covaxin proved safety and immunogenicity (Thiagarajan, 2021) (Ella et al., 2021) (Ella et al., 2020). The clinical efficacy was 81% in Bharat Biotech report (Thiagarajan, 2021). Sinopharm and Sinovax are similar to Covaxin.
Covidshield is structurally similar to AstraZeneca. Efficacy at preventing disease and infection to D614G & B.1.1.7 by AstraZeneca were 85% and 51% respectively; efficacy at preventing disease and infection to B.1.351, P.1, B.1.617.2 by AstraZeneca were 83% and 51% respectively (IHME, 2021). A large-scale study in India armed forces following completed Covishield vaccine revealed nearly 93% reduction in prevalence of Covid infections; and, reduction in COVID-related deaths by 98 % (Ghosh et al., 2021). However, the Omicron strain was refractory to current vaccine. The efficacy of vaccine on Variant of COVID-19: D614G (ancestral type), B.1.1.7 (Alpha), B.1.351 (Beta), P.1 (Gamma) and B.1.617.2 (Delta) should be assessed. Where genomic sequencing of cases did not occur, we use the location of the study as a proxy for the predominant variant type. For example, studies in South Africa were assumed to represent vaccine efficacy against B.1.351. BTI were found to be related with COVID-19 variant of concern (Kustin et al., 2021).
The efficacy varies with type of vaccine; 70% for Covaxin, 90% for Covishield and 94% for Sputnik V. The immunity was said to be lasted for 6 months. With the development of new strain, variant and subtype, the efficacy was found to be lowered. The effect of Covaxin on alpha & delta strain was mentioned in some studies (Lopez Bernal et al., 2021). Regarding Covaxin, efficacy at preventing disease and infection to D614G & B.1.1.7 were 78% and 69% respectively whereas efficacy at preventing disease and infection to B.1.351, P.1, B.1.617.2 were 68% and 60% respectively (IHME, 2021).
SARSCoV2 virus has been mutating; and most of the findings were the same- vaccine effectiveness against severe disease were higher and retained for longer than effectiveness against mild disease (UK Health Security Agency, 2021). Not only the findings from England but also from US confirmed that second booster or fourth dose had high protection rate 80% in first 6 months. Report from England in November 2021 which based on findings from 886,000 cases with the Omicron variant, primary immunization with two doses (ChAdOx1 nCoV-19 or BNT162b2 vaccine) gave limited protection against symptomatic disease caused by the omicron variant. However, a BNT162b2 or mRNA-1273 booster after either the ChAdOx1 nCoV-19 or BNT162b2 primary course substantially increased protection. Nevertheless, the duration of protection waned over time (Andrews et al., 2022). In recent CDC report released in 15 July 2022, after the first booster shot, vaccine effectiveness against severe illness with Omicron variants BA.1 and BA.2/BA.2.12.1 was 68% in the first six months. Then, it declined to 52
Study Design and Population
family members from January 2022 to May 2022. The SARS-CoV-2 infection was confirmed either with RT-PCR testing or rapid diagnostic test from a nasopharyngeal sample. Symptoms were analyzed by their selves and also by the primary investigator; then, they took appropriate treatment by themselves and senior physicians. If required, second opinion was given by senior physician through Viber. Moderate and severe cases were hospitalized and treated according to national and local guideline; they were followed up till day 30 through Viber. Data were collected by using standardized forms and analysis was done.
Operational Definitions
Unvaccinated means the subject did not receive COVID-19 vaccine dose at the time of study. In complete vaccinated means the subject did receive either one or two dose of COVID-19 vaccine. Complete vaccinated means the subject received third dose of COVID-19 vaccine. Complete vaccinated but not immune means the subject received third dose but < 14>
Body mass index (BMI) was a person’s weight in kilo-grams divided by the square of height in meters and it an indicator of body fatness. BMI was categorized as under- weight (< 18>
The severity of COVID-19 was classified as mild, moderate and severe disease. Mild disease was symptomatic patients without evidence of viral pneumonia or hypoxia. Moderate disease was confirmed patients with clinical signs of pneumonia (fever, cough, dyspnea, and fast breathing). Severe disease was confirmed patient with clinical signs of pneumonia (fever, cough, dyspnea, and fast breathing) adding one of the following: respiratory rate > 30 breaths per min, severe respiratory distress and SpO2 < 93>
Data Collection and Procedure
Demographic characteristics (sex, age, height, weight, blood group), comorbidity (hypertension, diabetes mellitus) and severity of disease (mild, moderate, and severe) were collected using a standardized case report form. The name of the vaccine and date of each dose were recorded. The data were checked by two medical officers and then, supervision, completeness, and consistency of collected data were performed by the principle investigator.
Statistical Analysis
The collected data were entered into Microsoft Excel 2016 and exported to IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY: IBM Corp) for analysis. Descriptive statistics were presented as frequency and percentages for categorical variables and mean (standard deviation, SD) for continuous variables.
Flow chart
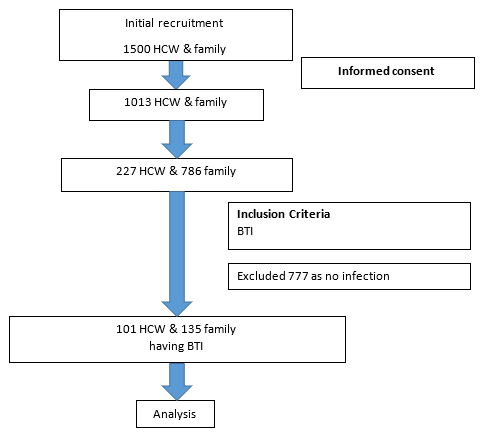
A total of 1013 subjects were recruited initially; 227 HCW and 786 family members. Less than half of HCW 44.4% (101/227) and 17.1% (135/786) of family members suffered BTI in fourth wave. Among them, 95% (96/101) of HCW and 57% (76/135) of family members had at least 3 doses of vaccine.
Table (1) shows the clinical characteristics and outcomes of HCW and family members infected in 4th wave of COVID-19 Pandemic. Mean age was 35.3 ± 7.0 years in HCW and 47.4 ± 22.6 years in family members. The age range in family members was 18 years to 96 years whereas that of HCW was 25 years to 59 years.
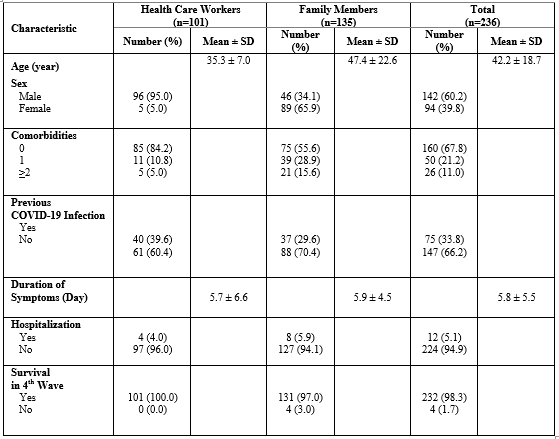
Table (1) : Clinical characteristics and outcomes of physicians and family members infected in 4th wave of COVID-19 Pandemic (N=236)
Comorbid status was noted in 15.8% of HCW and 44.4% of family members. The prevalence of breakthrough hospitalization was 4 (4.0%) HCW and 8 (5.9%) family members. The survival rate was 100% in HCW and 97% in family members.
Non survivors in family members were elderly; their age were 67 years, 70 years, 90 years and 96 years. Sixty-seven years old lady was late stage of carcinoma of breast though she had 4 doses of vaccine. Two non-survivors were unvaccinated; 96 years and 70 years. Both had comorbidities; diabetes mellitus, hypertension, chronic obstructive airway disease and obesity in 70 years old male; and diabetes mellitus in 96 years old man. over 65 years and they had multiple comorbidities. The remaining was 90 years old woman; she had only one dose of vaccine.
in 4th wave of COVID-19 Pandemic. Generally, 95% (96/101) of HCW and 56.3% (76/135) of family members who had COVID-19 infection received complete vaccination, 3 doses and more. In HCW, the chances of getting BTI was 47.5% after taking 3 doses; and, it dropped to 35.6
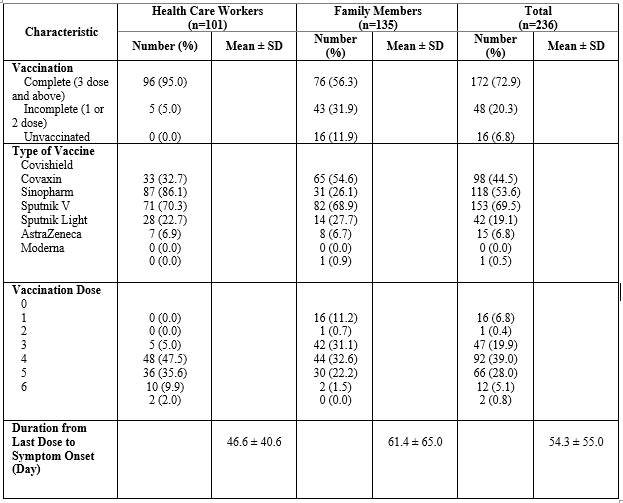
Table (2): Vaccination status of HCW and family members infected in 4th wave of COVID-19 Pandemic (N=236)
Table (3) demonstrates the vaccination status and previous infection in physicians and family members infected during 4th wave of COVID-19 Pandemic. One third of HCW and 15.8% of family members had COVID-19 infection either in the second wave and third wave; and, they received 3 doses of vaccine (complete vaccination) at the time of study. Fifty five percent of HCW and 41% of family members had 3 doses of vaccine (complete vaccination); and, they were not infected with SARS Co2 virus in the second wave and third wave
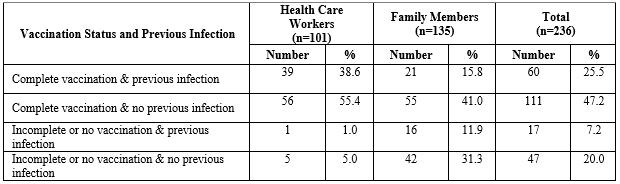
Table (3): Vaccination status and previous infection in physicians and family members infected during 4th wave of COVID-19 Pandemic (N=236)
Fourth wave of COVID-19 infection began in Myanmar in January 2022; the Omicron variant was imported from neighboring countries (Pyar, 2022). Fourth wave was mainly due to the Omicron variant as surveillance of nasopharyngeal swab PCR revealed the Omicron variant (Pyar, 2022). COVID-19 vaccine Programme has been launching since 2021; and, fifty percent of total population received two doses of vaccine. Health care workers have the opportunity to booster vaccine as they are front line workers; and, their family members have the access to National Vaccination Programme. In addition, the COVID-19 vaccine is available in private hospital and they can do vaccination there. In this study, the proportion of unvaccinated (subject did not receive COVID-19 vaccine dose at the time of study) was 11.2% in family members. Nearly 50% of population received at least one dose of vaccination at the time of study according to MOHS report; therefore, increasing vaccine coverage would reduce COVID-19 infection. The proportion of incomplete vaccinated person having BTI (subject did receive either one or two dose of COVID-19 vaccine) was 5% (5/97) in HCW and 32% (40/125) in family members; thus, incomplete vaccinated person could not prevent BTI.
Ninety five percent of HCW and 57% of family members had at least 3 doses of vaccine in this study. It was comparable with previous study on BTI among physicians in Myanmar done last year by K P Pyar et al where over 98% of physicians were fully vaccinated, two doses at their study period. Regarding type of vaccine, majority of physicians and HCW received was Covaxin in both studies done in 2021 and 2022 (Pyar et al., 2021). On the other hand, nearly 70% of family members were vaccinated with Sinopharm; they were non-government service persons.
In this study, nearly half of HCW and 17.1% of family members suffered BTI in fourth wave. Hence, the prevalence of BTI in HCW in this study was 10 times higher than other studies of BTI in HCW done in India, Israeli, Chicago and US (Sharma et al., 2021) (Tyagi et al., 2021) (Bergwerk et al., 2021) (Teran et al., 2020); and, two times higher than Myanmar study on BTI among physicians ( Pyar K P et al ., 2021). As the percentage of having booster dose/ 4 doses of vaccine among HCW was 36%, the reason for increasing prevalence of BTI among HCW may be related with viral factor- changes in genotype and phenotype, leading to reduction in vaccine efficacy to new mutant strain. Therefore, the WHO suggests to monitor genomic surveillance, phenotypic characteristics, and vaccine effectiveness data with respect to variant-updated vaccines (WHO, 2022a).
Ninety five percent of HCW had at least 3 doses of vaccine in this study; therefore, only half of HCW had BTI in fourth wave. The proportion of BTI among family members was higher than HCW (80%) because 57% of family members had at least 3 doses of vaccine. It can be concluded that 3 doses of COVID-19 vaccine had little protection for BTI in fourth wave. Moreover, following 4 doses of vaccine, 36% of HCW and 22% of family members did develop BTI in this study. It again pointed out 2 important facts. It confirmed that 4 doses of vaccine had better efficacy to prevent BTI than 3 doses as there was 50% reduction in number of BTI after 4 doses. Secondly, 4 doses of vaccine did not have 100% protection because 36% of HCW and 22% of family members who had 4 doses suffered BTI in fourth wave.
In addition, the frequency of acquiring BTI after 5 doses dropped dramatically to 10% in HCW and 2% in family members. Therefore, 5 doses seemed to have greater protection against BTI; it also confirmed the report from UK in 2021 and US in July 2022. According to the report from England in November 2021 which based on findings from 886,000 cases with the Omicron variant, primary immunization with two doses (ChAdOx1 nCoV-19 or BNT162b2 vaccine) gave limited protection against symptomatic disease caused by the omicron variant. However, a BNT162b2 or mRNA-1273 booster after either the ChAdOx1 nCoV-19 or BNT162b2 primary course substantially increased protection (UK Health Security Agency). Fourth doses were also associated with a reduction of hospitalization and emergency department visits related to BA.1 and BA.2/BA.2.12.1(CDC, 2022).
Regarding the severity of infection, they did not require oxygen therapy or ventilatory support; thus, they were mild cases. It gave another evidence for previous findings from Myanmar (Pyar et al., 2021) as well as other reports from India (Girish Chandra Dash et al., 2021) (Tyagi et al., 2021). Only 3 cases from HCW and 8 cases from family members required hospital admission in this study were mild; thus, it proved the findings from various countries as well as Myanmar study in 2021. In the study from Israeli breakthrough infection in HCW were mild or asymptomatic (Bergwerk et al., 2021). Furthermore, the study done in Delhi which included 325 HCW, 95% of cases were mild and did not need oxygen therapy (Sharma et al., 2021). Moreover, the study carried out among HCW in chronic care hospital dealing with cases of diabetes mellitus, prevalence of symptomatic BTI was 13.5% (15/113) and only one case (1/15) required treatment in hospital; mortality rate was zero (Tyagi et al., 2021). In addition, in Chicago study, two-third of BTI were asymptomatic and 10% of cases (2/22) were hospitalized; one out of two hospitalized cases died because of co-morbidities and the contributing factor for death was multiple co-morbidities (Teran et al., 2020). Reasons to be hospitalized in BTI were interesting; it may or may not be related with COVID-19. The report on BTI to CDC in 2021 April, based on preliminary data, 2,725 (27%) cases of BTI were asymptomatic, and 995 (10%) patients were known to be hospitalized; and, 160 (2%) patients died. Among the 995 hospitalized patients, 289 (29%) were asymptomatic or hospitalized for a reason unrelated to COVID-19 (CDC COVID-19 Vaccine Breakthrough Case Investigations Team, 2021). In this study, 4 cases from family member were non-survivors; they were elderly people with multiple co-morbidities. The mortality rate was almost zero among HCW. It also gave another supporting evidences that vaccination prevented prevalence of infection, reduced the severity of infection and mortality.
The fact that natural immunity from previous COVID-19 infection should have protection to same variant was not true in the Omicron variant infection; there were several reports on reinfection in the Omicron variant infection, (Steel & Fordham, 2022). Therefore, the analysis was done among cases of BTI with completed vaccination. One third of HCW and 15.8% of family members had COVID-19 infection either in the second wave and third wave and they received 3 doses of vaccine (complete vaccination); it showed that the immunity acquired from previous COVID-19 infection (possibly the Delta wave infection) did not prevent the new infection, the Omicron variant. Fifty five percent of HCW and 41% of family members had 3 doses of vaccine (complete vaccination) and they were not infected with SARS Co2 virus in the second wave and third wave; it confirmed that the infectivity rate of the Omicron variant was higher than the previous wave- the Delta variant.
The proportion of complete vaccinated persons having BTI (subject received third dose of COVID-19 vaccine) was 94.8% in HCW and 56.8% in family members; therefore, third dose of COVID-19 had minimal protection against COVID-19 infection possibly the Omicron variant. However, it prevented severe form of disease; oxygen requirement and ventilatory support. Furthermore, it reduced breakthrough hospitalization; 3% in HCW and 6% in family members. It also cut the mortality; zero in HCW and 3% in family members. It confirmed the previous reports.
Comorbid status was low in (15.8%) in HCW; and, three times higher (44.4%) in family members.The mean age was higher in family members. As BTI may be causally related to the host determinants (age, comorbidities, immune status, immunosuppressive drugs), the prevalence of breakthrough hospitalization was 4 (4.0%) in HCW and 8 (5.9%) in family members. The survival rate was 100% in HCW and 97% in family members.
Non survivors in family members were elderly; their age were 67 years, 70 years, 90 years and 96 years. Sixty-seven years old lady was late stage of carcinoma of breast though she had 4 doses of vaccine. Two non-survivors were unvaccinated; 96 years and 70 years. Both had comorbidities; diabetes mellitus, hypertension, chronic obstructive airway disease and obesity in 70 years old male; and diabetes mellitus in 96 years old man. over 65 years and they had multiple comorbidities. The remaining was 90 years old woman; she had only one dose of vaccine.
Serial measurement of protective antibody level to SARS CoV2 virus following vaccination should be done in this study as immunity characteristics like mucosal versus systemic immunity, duration of immunity determines vaccine efficacy and BTI. Moreover, BTI may be causally related to the viral profile such as viral variant and load, incubation period, transmissibility, pathogenicity, immune evasion; viral load and sub-variant type were not done in this study. Being resource limited setting, the study could not confine to one particular type of vaccine.
The majority of BTI in fourth wave was mild and the prevalence of breakthrough hospitalization was 3-6% in HCW and family members; showing the protective effect of vaccine from severe manifestation. Non-survivors had multiple comorbidities. The chance of BTI was decreasing if they obtained 3 doses and 4 doses compared to 2 doses. The possibility of BTI after taking 3 doses of vaccine was 50% in HCW and 33% in family members; it dropped to 36% and 22% respectively after 4 doses of vaccine. Thus, 3 doses of COVID-19 vaccine could protect 50-67 percent; the protective efficacy increased to 65-87 percent with 4 doses. Therefore, 4 doses of COVID-19 vaccine are recommended for prevention of fifth wave in Myanmar.
Therefore, expansion of COVID vaccination program is required to reduce morbidity and mortality of future COVID-19 infection in Myanmar. Cost-effectiveness of vaccine should be logistically important too particularly in low resource setting. Research on BTI in relation to changing variant should be considered.. Serial measurement of protective antibody level should be done for recommendation of exact timing for booster dose.
The authors would like to thank all the candidates for giving informed consent to this study. The authors also acknowledged Prof Ko Ko Lwin, Prof Kyaw Zay Ya, Prof Myint Zaw for administrative support, and Professor Khine Khine Su and Dr Kyaw Wunna for laboratory support.
The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
This study was approved by Hospital Research and Ethic Committee from Defence Services General Hospital (1,000-Bedded) Mingaladon, Myanmar. Informed consent was also taken from each physician.
The authors received no financial support for publication of this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
