
Case Report | DOI: https://doi.org/10.31579/2690-1919/530
1Departments of Orthopaedics and Pathology Beijing United Family Hospital, No 2 Jiangtai Road, Chaoyang District, Beijing, 100016, China.
2Pathology Beijing United Family Hospital, No 2 Jiangtai Road, Chaoyang District, Beijing, 100016, China.
*Corresponding Author: Jike Lu, Departments of Orthopaedics and Pathology Beijing United Family Hospital, No 2 Jiangtai Road, Chaoyang District, Beijing, 100016, China.
Citation: Xu B. Qiao, Jing Niu., Jun Jiang, Gao Feng Xu, and Jike Lu, et al, (2025), Brachialis Muscle Ischemia Causing Elbow Flexion Deformity with Myositis Ossificans – A Case Report, J Clinical Research and Reports, 19(5); DOI:10.31579/2690-1919/530
Copyright: © 2025, Jike Lu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 April 2025 | Accepted: 05 May 2025 | Published: 14 May 2025
Keywords: myositis ossificans; calcification; muscles ischemia; outside-in; inside-out; popcorn sign; tumors; FISH test
Myositis ossificans (MO) is a rare entity of extra-skeletal bone formation in various muscles, most commonly in quadriceps, gluteals, small muscles of hand and brachialis, which often triggered by trauma or ischemia. It is first described in medical literature during the 17th–18th centuries, with early cases linked to traumatic injuries. Traumatic MO Formally classified by German pathologist Von Dusch in 1868. Historically, it was termed "rider's bone" due to its association with horseback riding injuries. Repeated trauma to the elbow from sports may be linked to the development of myositis ossificans traumatica (MOT). We report a case of MOT in a 26-year-old male who sustained non-traumatic ischemic compression during sleep and presented with severe pain and a fixed flexion deformity of the elbow. The patient typically presented as a painful, tender, enlarging mass, which was located in anterior distal humerus within brachial muscles of the upper arm, following subtle repetitive local trauma. Although it seems unnoticed, causing ischemia alteration in brachial muscles while he was sleeping on his volar aspect of the elbow for several months. Imaging studies, including ultrasound, X-ray, CT and MRI, revealed a bony mass in the anterior aspect of the right elbow and a history of brachial ischemia caused by sustained pressure. Biopsy histology and molecular biology studies confirmed the diagnosis of MOT. Clinically, MO may present as a painful soft-tissue mass, which could be confused with tumor or inflammatory lesions. MO goes through different phases of evolution, and its appearance on imaging varies depending on the stage of investigation. For differentiation diagnosis from soft-tissue tumors or other malignancies, comprehensive image studies and histology, molecular biology studies are compulsory.
Myositis ossificans (MO) is a benign non-neoplastic disorder characterized by the formation of heterotopic bone in extra-skeletal soft tissues [1]. It predominantly affects adolescents and young adults, with the highest incidence occurring in the second and third decades of life. Males are more commonly affected by MO [1, 2]. MO is classified into three types: fibrodysplasia ossificans progressiva (FOP), MO circumscripta or traumatica (MOT), and MO without a history of trauma (non-traumatic or pseudomalignant MO) [2]. FOP is an ACVR1 mutation and causing constitutive activation of BMP pathway, leading to spontaneous ossification in muscles, tendons, ligaments. MOT is caused by inflammation or hematoma, which induces mesenchymal stem cells to differentiate into osteoblasts via BMP signaling pathway. Ossification in MOT typically occurs in mid-muscle belly. It is primarily an autosomal-dominant condition that usually affects a single muscle or muscle group. The quadriceps, brachialis, and thigh adductor muscles are among the most affected regions [1, 3, and 4]. Patients with MOT are young and with a history of contacting sports. They typically present with pain and restricted range of motion following trauma, ischemia hassling or overuse. The possible causes include repetitive minor mechanical injuries, ischemia, and other noxious stimulation [2]. This study describes the specific image findings, characteristics of the biopsy histology and molecular biology studies, and discussion of differentiation diagnosis of MOT from soft-tissue tumors or other malignancies.
In this case, a 26-year-old male presented with a complaint of inability to perform motions with his right elbow for the past a month. He was habitually sleeping on his right elbow over his anterior aspect of the distal humerus area for several months and he denied any major injuries. However, due to persistent severe pain, he tried to keep his elbow still and took oral ibuprofen. There was pain during nights and woke him up several times. Any movement of the elbow joint triggered severe pain. Gradually, moving his right elbow was became restricted, with severe flexion deformity. On examination, the right forearm was flexed at 90 degrees with mild swelling noted over the right anterior distal humerus (Fig 1). Upon palpation,tenderness over the anterior distal humerus in brachial musculature and a 5cm soft-tissue mass was palpable. The mass was tender and located in brachial muscles which was moving with elbow flexion and extension. Tinel’s sign was negative. The neurovascular system of the right upper limb appeared intact. Upon investigations, including ultrasonography, anterior-posterior and lateral X-rays, CT, MRI of the right elbow, revealed a bony mass in the anterior distal humerus muscles, as shown in Figures 2-5.
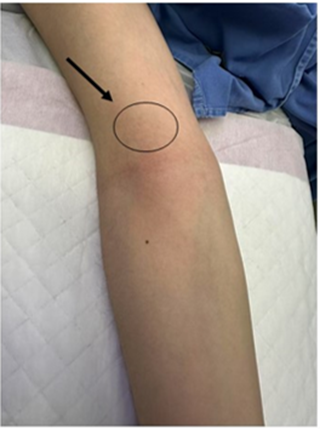
Figure 1: A 5 cm soft-tissue mass was seen and palpable over distal anterior aspect of the humerus that was tenderness and painful while doing any elbow motions (an arrow indicates the mass).
Ultrasonography is the best investigation modality in differentiating between cystic and solid lesions, and for early diagnosis of heterotopic bone formation. Ultrasonography in our case demonstrated a heterogeneous solid mass and some internal blood flow on the Doppler examination. It was noticed the hyperechoic rim surrounded by a hypoechoic rim and the central area that is hypoechoic as well (Figure 2). The calcified lesion was located over distal humerus just above the olecranon fossa on AP radiograph. The calcifications typically become more peripherally oriented and coarse in appearance with a calcified peripheral rim with a lucent center, the calcifications appear as amorphous and flocculent simulating osteoid matrix in brachial muscles (Figure 3).
A low-attenuation soft-tissue mass with associated calcifications, typically the peripheral rim becomes increasingly calcified and the central lucent zone is isodense to adjacent brachial muscles. AP view CT showed “popcorn” calcification in soft tissue with radiolucent center and sagittal plane CT revealed the “popcorn” calcification is not from adjacent bones. The axial view CT demonstrated clearly that the calcification mass anterior to distal humerus in brachial muscles (Figure 4). The MRI appearance follows the isointense to hypointense to skeletal muscle on T1-weighted sequences. T2-weighted sequences will appear hyperintense to surrounding muscles. The peripheral low signal intensity can be seen (Figure 5).
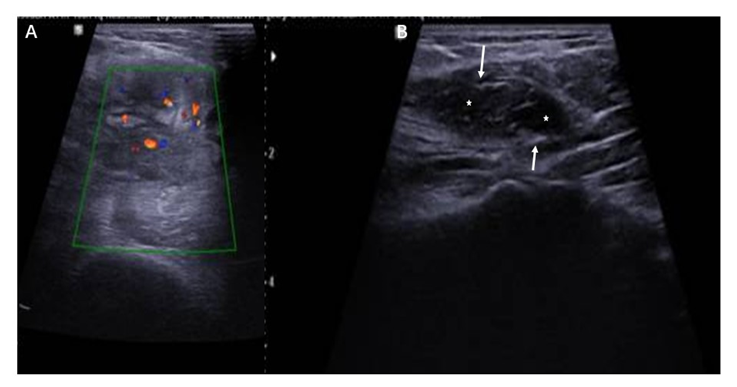
Figure 2: Ultrasonography demonstrates a heterogeneous mass demonstrating some internal blood flow on the Doppler examination (red dots in A). Note the hyperechoic rim (arrows) surrounded by a hypoechoic rim and the central area that is hypoechoic as well (stars).
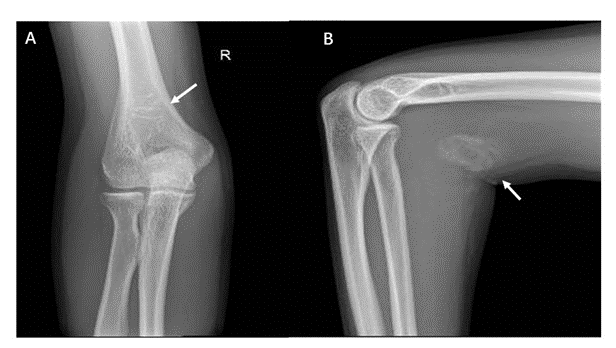
Figure 3: The typical radiographic appearance of MO is circumferential calcification with a lucent center and a radiolucent cleft (“popcorn sign”) that separates the lesion from the cortex of the adjacent bone. This pattern of peripheral predominate calcification is a clinically significant feature which distinguishes this entity from (parosteal osteosarcoma) that tends to contain centrally located calcifications. The calcified lesion is located over distal humerus just above the olecranon fossa on AP radiograph (an arrow in A). The calcifications typically become more peripherally oriented and coarse in appearance with a calcified peripheral rim and a lucent center (A). The calcifications appear as amorphous and flocculent simulating osteoid matrix in brachial muscles (an arrow in B)
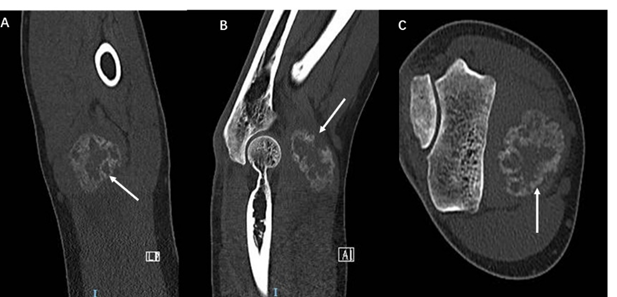
Figure 4: A low-attenuation soft-tissue mass with associated calcifications, typically the peripheral rim becomes increasingly calcified and the central lucent zone is typically isodense to adjacent brachial muscles. AP view CT showed “popcorn” calcification in soft tissue with radiolucent center (an arrow in A) and sagittal plane CT revealed the “popcorn” calcification is not from adjacent bone (arrow in B). The axial view CT demonstrated clearly that the calcification mass anterior to distal humerus in brachial muscle (arrow in C).
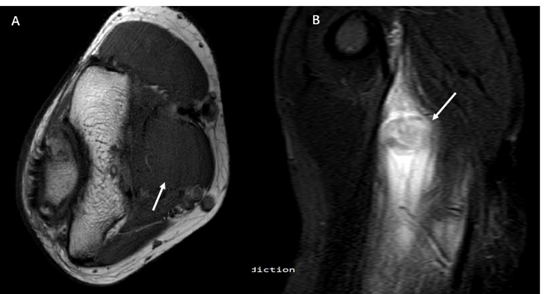
Figure 5: The MRI appearance that follows the isointense to hypo intense to skeletal muscle on T1-weighted sequences (An arrow in A). T2-weighted sequences will appear hyperintense to surrounding muscle. The peripheral low signal intensity can be seen (An arrow in B).
The needle core biopsy was performed under general anesthesia. Five strips of tan soft tissues from one entry point but towards different directions of the mass were taken with the samples in 2mm in diameter and 15-20mm in length respectively. Histological sections reveal that the cytological features of the lesion were similar to those of nodular fasciitis.
The fibroblastic or myofibroblast cells in the lesion are uniform and have bland nuclear features with vascularized stroma with extravagated erythrocytes, fibrin, and lymphocytes. Mitoses are present but are not atypical. A typical histologic finding is woven bone formation with a conspicuous peripheral lining of osteoblasts. The histologic features were consistent with MOT (Figure 6).
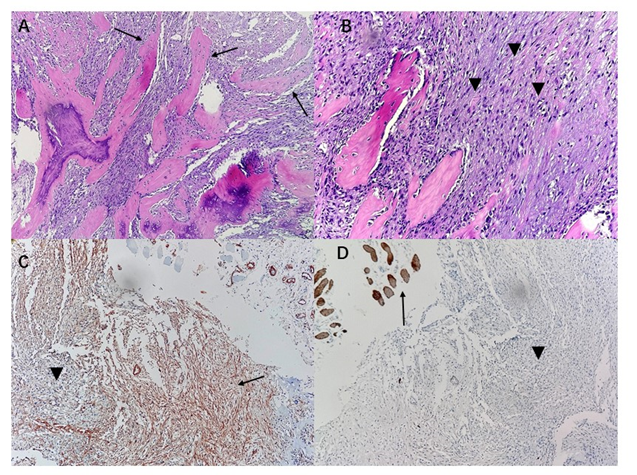
Figure 6: Histology and immunohistology photos: A. 10x20 power view field displayed very typical histologic feature of MO: zonal maturation of bone with osteoblastic rimming (arrows); B. 10x40 power field Some areas reveal that centralized proliferations of spindle fibroblasts and myofibroblasts and mixed with mature bone (arrow heads); C and D. 10x20 power view filed demonstrated spindle fibroblasts (an arrow) and myofibroblasts (an arrow head) with smooth muscle actin (SMA) [removed]C, an arrow), but the myogenic marker Desmin (D) is negative (an arrow head).
The final diagnosis needs USP6 gene (ubiquitin-specific protease 6) rearrangements, which are present in most MOT cases. The FISH test
(fluorescence in situ hybridization) demonstrated the USP6 gene rearrangement in the samples which is consistent with clinical and histological diagnosis of MO (Figure 7 C).
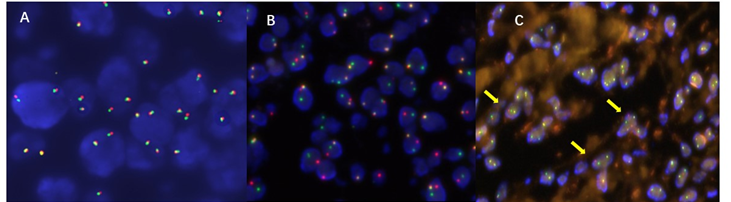
Figure 7: Fluorescence in situ hybridization study: A. Negative control; B. positive control; C. the sample tested revealed positive for USP6 gene breakage. Break-apart fluorescence in situ hybridization FISH reveals rearranged USP6 (arrows).
MO is a lesion characterized by calcification or ossification within muscle or other soft tissues, typically occurring following trauma and hematoma formation in the affected area [3]. Extra-skeletal bone formation was first described by Guy Patin in 1692 and Von Dusche in 1868, and was named MOT [3]. MOT is primarily caused by changes in perimysium connective tissue rather than the myocytes themselves. Inducible osteoprogenitor cells (IOPCs) in this tissue are responsible for the formation of heterotopic bone in MOT. Under the influence of local and systemic factors, IOPCs can differentiate into cartilage and bone cells. These cells are not fixed in one location and can migrate through the bloodstream or lymphatic system and have been observed in various anatomical sites such as lymph nodes, skin, thymus, and spleen. This ability of IOPCs to form bone in different areas beyond the injury site contributes to the development of MOT [5].
MOT usually occurs in response to traumatic injury without a direct genetic cause, whereas FOP is a rare genetic autosomal dominant disorder caused by mutations on chromosome 2 of the ACVR1 gene. The gene
encodes a receptor for a protein called bone morphogenetic protein (BMP), which regulates bone and cartilage formation. This mutation leads to the inappropriate activation of BMP signaling, resulting in abnormal bone formation in soft tissues, often triggered by trauma [6]. However, the brachialis muscle due to ischemia from habitual sleep positioning is unusual in our case study.
In a case series reported by Saad A et al., it was observed that 73% of MOT cases affected the muscles of the lower limbs, with 26
MOT is a real and obviously benign condition that can cause the debilitating complication of muscle ischemia, and often leading to severe limitations in joint function. Patients without a history of injury or with unnoticed subtle compression of the muscles (as in our case) may develop MO. It is essential to differentiate MOT from other conditions with similar features, such as malignant fibrous histiocytoma, soft-tissue sarcomas (e.g., synovial sarcoma), malignant bone tumors, especially parosteal sarcoma, calcific tendinitis, infectious osteomyelitis, extra-skeletal osteosarcoma, and other types of MO. Diagnosing MOT requires careful consideration of the clinical history, imaging studies (ultrasound, X-ray, CT scan, and MRI), and biopsy for histopathological and molecular confirmation. Early and accurate diagnosis is crucial to reducing pain symptoms, preserving joint function, and optimize outcomes for individuals with MOT. However, the mechanism of the muscles ischemia causing MOT needs further study in the future.
Dr. Jike Lu, Department of Orthopedic Surgery, Beijing United Family Hospital, Beijing, China,
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
