
Review Article | DOI: https://doi.org/10.31579/2690-4861/150
*Corresponding Author: Pooja Pithadia, Medical Biotechnology, Medica Pain Management Clinic, London, UK.
Citation: P Pithadia, S Tulpuele, M Rahman, M Singh. (2021) BMAC and Adipose-Derived MSCs Treatment for Knee Osteoarthritis: A Systematic Review. International Journal of Clinical Case Reports and Reviews. 7(5); DOI: 10.31579/2690-4861/150
Copyright: © 2021 Pooja Pithadia, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 June 2021 | Accepted: 14 July 2021 | Published: 17 July 2021
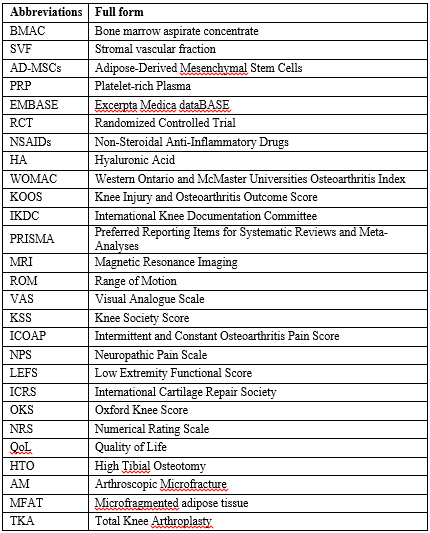
Keywords: bmac; stromal vascular fraction; adipose-derived mesenchymal stem cells; bone marrow aspirate concentrate; svf; knee osteoarthritis
Background: Knee osteoarthritis is the most common musculoskeletal progressive disorder that affects nearly 303 million people worldwide. This condition prevails in 10% males and 13% females among the elders above 60. Although there is conventional nonsurgical and surgical treatment available for knee osteoarthritis, there is a fascinating interest in bone marrow aspirate concentrate (BMAC) as well as adipose-derived mesenchymal stem cells (AD-MSC), including enzymatically treated stromal vascular fraction (SVF) and mechanically treated (microfat/nanofat) injections among physicians. Hence, this systematic review aims to determine the efficacy of BMAC and AD-MSCs (enzyme and mechanically treated) injections for knee osteoarthritis treatment.
Methods: A systematic review was performed on the following data sources (PubMed, Scopus, Google Scholar, EMBASE, and Cochrane Library) published on March 31, 2021. The keywords or MeSH terms include 'Knee Osteoarthritis with 'Bone marrow aspirate concentrate' OR 'BMAC' or with 'Adipose-derived mesenchymal stem cells (AD-MSC)' or with 'Stromal vascular fraction' OR 'SVF' or 'Mechanically treated AD-MSC (mfat/nanofat)'. In addition, the retrieved articles were further reviewed to identify relevant research studies.
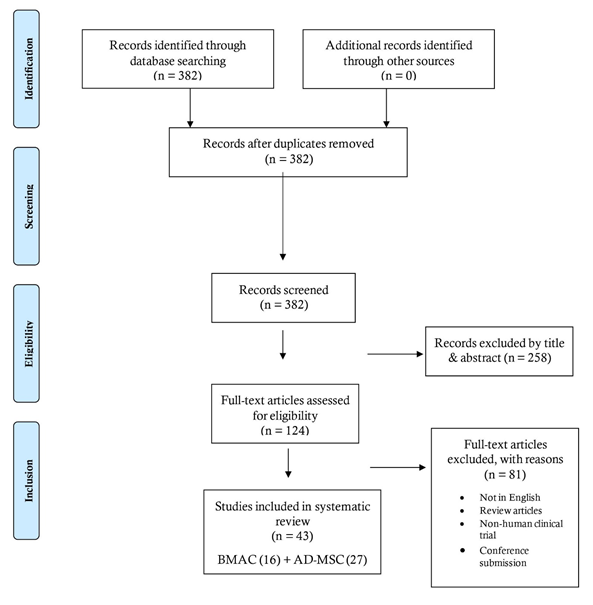
Results: The authors reviewed and tabulated data based on the year of study, study type, therapy protocol, patient population, outcome measures, and interpretation. Among the 382 records screened, 43 studies (16 on BMAC and 27 on AD-MSCs) were included in the systematic review study. Among them, only 5 were randomized controlled trials. These selected studies demonstrated short-term positive outcomes such as improvement in knee pain and function with no adverse side effects. Moreover, researchers reported varied administration methods of BMAC or AD-MSC either as standalone or in combination with other conservative procedures such as PRP (Platelets Rich Plasma), HA (Hyaluronic acid), or surgery.
Conclusions: BMAC and AD-MSC (enzymatically and mechanically treated) injections prove safer and more efficacious in patients with knee osteoarthritis for a shorter duration of 2 years. However, the available literature lacks high-quality studies with no varied clinical settings and long-term follow-up of more than two years.
Osteoarthritis (OA) is the most common type of progressive musculoskeletal arthritic disorder affecting nearly 303 million people worldwide [1]. Compared to all the joint regions, OA commonly affects hip and knee joints [2]. Due to a steady increase in ageing, obesity, and life expectancy, knee OA is prevalent in 10% males and 13
This systematic review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [17,18].
A comprehensive, systematic literature search was performed in April 2021, and an analysis of these articles was conducted by all the authors involved in the study. The databases of PubMed, Scopus, Google Scholar, EMBASE, and Cochrane Library were searched from 2011 to March 31, 2021. The following keywords were used in different combinations: 'Knee Osteoarthritis with 'Bone marrow aspirate concentrate' OR 'BMAC' or 'Adipose-derived mesenchymal stem cells or 'Stromal vascular fraction' OR 'SVF' or 'Mechanically treated AD-MSC (mfat/nanofat)'.
Study selection
All participants in the trials had to have a clinical diagnosis of knee osteoarthritis under either intra-articular BMAC or AD-MSCs treatment.
We limited the search to articles in English, and only human studies were included. After assessing all titles and abstracts, all relevant articles were obtained. Even the bibliographies were also searched to identify further relevant literature that met our inclusion criteria.
All studies were included if their design could be classified into one of the following categories: open-label, randomized controlled trial, prospective, retrospective study, and pilot study.
We included studies in which adult participants were diagnosed with knee osteoarthritis by clinical or image evaluation. We excluded articles lacking access to the full text, conference presentations, narrative reviews, editorials, and expert opinions.
The articles found were pooled and subjected to inclusion and exclusion criteria established before the commencement of this systematic review. A PRISMA flowchart of this systematic review is provided in Figure I.
Data extraction
The researchers independently recorded the study design, therapy protocol, patient population, outcome measures, and interpretations.
Literature search
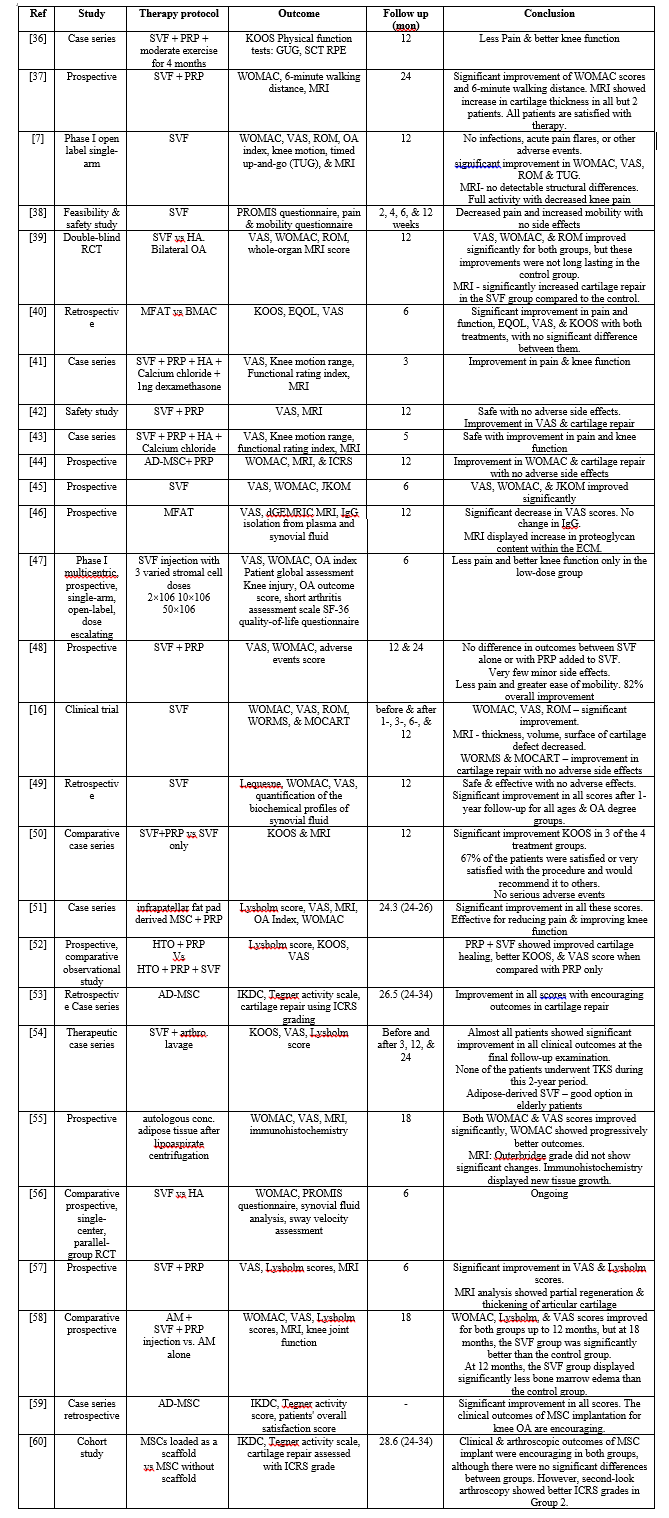
Of the 382 articles initially identified by the search, 16 [19,30,32,35] on BMAC and 27 [36,62,16]. on AD-MSCs, including SVF, met the inclusion criteria. Therefore, the relevant data is given in Tables III and IV.
Participants
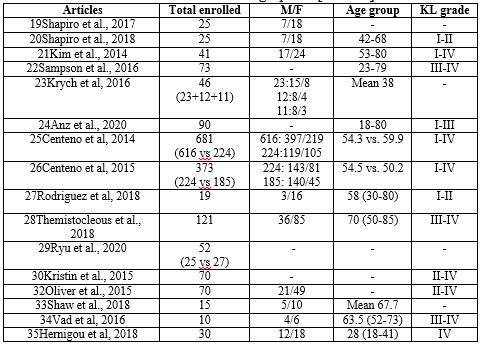
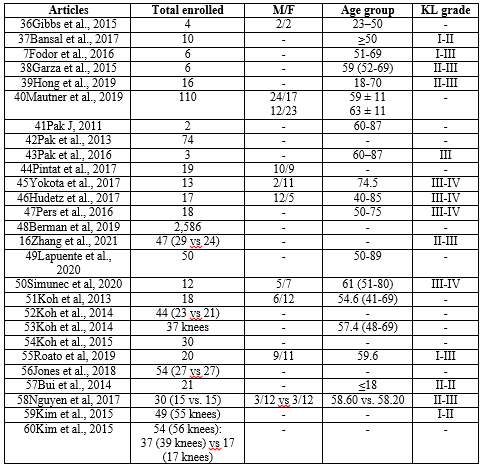
The 16 studies under BMAC involved 10 to 681 patients with the age group of between 18-85 affected by knee OA [Table I), while 27 studies under AD-MSCs, including SVF, involved 2 to 2586 knee OA patients between 18-89 age group [Table II]. Among these 44 studies, only 5 were randomized controlled trials. Fourteen papers were prospective studies, with three of them being comparative, two being open-label, one being a pilot study. The rest were retrospective studies, with two of them being comparative.
Therapeutic approaches
Regarding the therapeutic protocol, BMAC was either injected alone or combined with PRP in the same session, alternatively as a booster dose after a certain period. Very few authors injected BMAC in association with adipose tissue or scaffold. Under AD-MSCs, it was either injected alone or combined with PRP, adipose tissue, HA, or scaffold.
Outcome measures
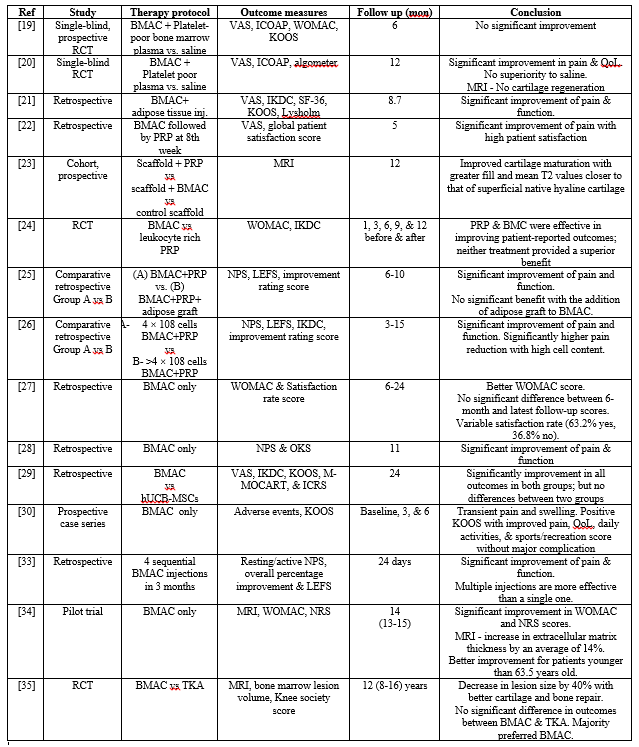
Regarding outcomes, varied clinical scores such as WOMAC, VAS, KOOS, IKDC, KSS, ICOAP, NPS, and LEFS were used to evaluate the outcomes of BMAC injections (Table 1) and AD-MSCs injections (Table 2). Even MRI was performed before and after the procedure to detect positive changes in the resultant images. Very few authors used ICRS, OKS, NRS, ROM, Tegner activity, Lysholm patient satisfaction scores, and PROMIS questionnaires. Immunohistochemical analysis was reported only in Roato et al. 55. 's study involving AD-MSCs injections.
Safety and efficacy of BMAC and AD-MSCs therapy
None of the studies analyzed in this systematic review recorded any complication or adverse effect of BMAC and AD-MSCs administration. Only mild pain and swelling have been observed in very few patients within the initial few days following BMAC/AD-MSCs injection procedure. Furthermore, both BMAC and AD-MSCs showed positive clinical outcomes with significant improvement in pain, articular function, and range of movement.
The results of this systematic review validate that both BMAC and AD-MSCs treatments are safe and effective to treat knee OA. However, the therapeutic use of BMAC and AD-MSCs, especially SVF, is restricted across the United States, Europe, and many other countries based on safety and efficacy concerns.
The significant finding of this systematic review is that most of the studies are of low quality with a lack of well-defined methodologies, with very few RCTs, thus preventing us from providing any substantial conclusions on the therapeutic potential of these AD-MSCs and BMAC injections.
Furthermore, there is an inadequate patient selection process, although these studies reported good reliability. The inclusion and exclusion criteria, recruitment rate, and a well-defined selection process were rarely reported. Hence, further studies including larger patient cohorts should be performed to demonstrate the long-term effect of both BMAC and AD-MSCs injections.
Many patients underwent conservative treatments such as steroid treatment or surgical procedures in most of these studies, such as microfracture, arthroscopic debridement, or high tibial osteotomy. Hence there is no clear understanding of the exclusive clinical potential of these BMAC and AD-MSCs injections.
We can find the release of platelet-rich plasma (PRP) treatment without adequate evidence in the recent past. This treatment has been used clinically due to high media exposure only [61]. There is a possibility to exempt 510(k) regulations [62]. New medical devices "substantially equivalent" to those already prevalent in the market can skip the standard FDA approval process. Hence, there was an increase in the production of PRP kits. However, this market saturated due to overproduction by various preparation systems, thereby preventing a "standardization" of PRP therapy for knee OA treatment.
This same scenario is now approaching AD-MSCs and BMAC therapies that are not affected by the regulatory burden. Moreover, they can be quickly harvested from the OA patient and administered immediately through an intra-articular injection with PRP or HA (hyaluronic acid). HA provides an environment where MSCs can easily adhere to the target area around the lesion and differentiate into cells to build damaged bone and cartilage. Similarly, PRP consists of highly concentrated platelets and varied growth factors to exacerbate the proliferation of MSCs [68,69]. Hence, this simultaneous use of other biological agents or administering these treatments following the conventional procedures prevent a reasonable comparison of the studies performed so far.
The available RCTs have several biases since most of the patients were treated bilaterally [20,63]. This is not the ideal condition to determine the efficacy of a treatment since the patients cannot evaluate one knee independently from the other. There was no proper clarity on the number of cells administered and the exact number of injections for the best outcome. It was even difficult to interpret which one of the two treatments provide better outcomes. Although their immunophenotypes are more than 90% identical [64,65], they still have many distinct characteristics, especially in their cell surface markers, differentiation potentials, and distribution within the body. An in vitro analysis revealed that almost 300-fold more SVF can be derived from 100 g of adipose tissue when compared to 100 ml of bone marrow aspirate [66,67]. However, there is no apparent connection between the quantity and the dose-effect. Furthermore, there is no substantial evidence to define the patient's profile that could respond better to a specific treatment compared to others. Hence, this topic demands more research to understand the effect of both BMAC and AD-MSCs therapies.
Both bone marrow harvesting and lipoaspiration are minimally invasive procedures with minimal side effects. However, lipoaspiration was more severe due to the associated risks of pain and hematoma. Anyway, the surgeon who opts for these treatments depends on the availability of preparation kits in different countries. Moreover, industries have been releasing their proprietary kits for BMAC and AD-MSCs preparation, with new methods still being developed. However, there is no adequate research evidence to support the ability of MSCs.
At present, stem cell treatment is expensive and cannot be considered a "routine" treatment for knee cartilage degeneration. From a clinical viewpoint, the use of BMAC and AD-MSCs for knee OA treatment seems to be safe and deliver positive clinical outcomes. Moreover, this treatment can be a minimally invasive therapeutic option for patients who are ineligible for surgery. However, their promising outcomes for a shorter duration (3 months–24 months) must sustain for the long term of more than two years compared to the available conventional treatments. Hence, the use of BMAC or AD-MSCs therapies must be thoroughly discussed between the physician and the patient before proposing them as a first-line therapeutic approach to avoid surgery.
However, increasing the number of treatment options for knee OA does not always intend to improve the standard of care, especially when there is a lack of enough comparative trials that determine the effectiveness of a novel treatment compared to established ones.
Limitations
It is possible that BMAC and AD-MSCs injections could deliver positive outcomes in treating knee osteoarthritis, according to the results from our study. Nonetheless, the factors affecting the outcomes are but not limited to the lack of control group, a small number of studies and co-interventions, a small sample size, lack of long-term follow-up of not more than two years, the possibility of bias, and lack of objective assessment on the interventions
Although these above findings provide encouraging results, the lack of comparative study with corticosteroids and hyaluronic acid limits definitive conclusions, furthermore, the relationship of sex, age, and the severity of knee osteoarthritis could not be figured out clearly.
Additionally, MRI evaluation was not performed in all the studies to complement the clinical parameters, including the quantification of knee cartilage regeneration following the treatment. Moreover, there is a lack of comparison among the outcomes for different KL grades. Hence, more studies are required to confirm the positive long-term effects of AD-MSCs and BMAC therapies for knee osteoarthritis.
Despite having all these limitations, the treatment of knee osteoarthritis with BMAC and AD-MSCs seems to be safe by delivering positive clinical outcomes. This treatment can be a potential minimally invasive option for those who are ineligible for invasive approaches.
BMAC and AD-MSCs injections prove safer and more efficacious in treating knee osteoarthritis on a short-term duration (3 months-24 months) without any adverse side effects. However, only very few randomized control studies are published to support this result. Additionally, there is a lack of high-quality research studies for more than 2 years with varied trial settings.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
