
Research Article | DOI: https://doi.org/10.31579/2767-7370/065
North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, M8 5RB. United Kingdom
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, M8 5RB. United Kingdom
Citation: Grey Venyo A. K, (2023). Blastomycosis Prostatitis and Blastomycisis Prostate Abscess: A Review and Update. J New Medical Innovations and Research, 4(7); DOI:10.31579/2767-7370/065
Copyright: © 2023, Anthony Kodzo-Grey Venyo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 October 2023 | Accepted: 25 October 2023 | Published: 31 October 2023
Keywords: blastomycoses; blastomycis; prostatitis, prostate abscess; soil; fungus; yeast; asymptomatic; non-specific; smear, biopsy; aspiration; fever; urinary retention; ultrasound scan
Blastomycosis is a globally accepted terminology that is used for a fungal infection which is also referred to as Gilchrist’s disease, which typically afflicts the lungs, but which in addition has the cpability of spreading to the brain, the stomach, the intestine, as well as the skin, where it does manifests as crusting, purple looking warty plaques that are associated with a roundish, bumpy edge as well as central depression. About half of individuals who are afflicted by Blastomycosis, remain asymptomatic and the remaing half do tend to develop symptoms which could include fever, cough, night sweats, muscle pains, loss of weight, chest pain as well as a sensation of feeling tired. The symptoms of Blastomycosis tend to manifest between three weeks and three months ensuing breathing inhalation of Blastomyces spores. It is known that in approximately 25% to 40% of cases of Blastomycosis, the infection could also traverse to other parts of the human body including the skin, bones, central nervous system and on rare occasions. Blastomycosis, could secondarily afflict the urogenital system, or the affliction could be on extremely rare occasions, afflict only the genitourinary tract system only without affecting any other part of the human body. It is known that even though blastomycosis tends to be very dangerous for individuals who have immunosuppression as multiple other co-morbidities. Many individuals who are afflicted by Blastomycosis are ummunocompetent. Bla stomyces dermatidis is encountred within the soil, as well as within decaying organic matter including wood and leaves. It is understood that outdoor activities including: toiletting the soil, hunting and camping within wooden areas do increas the risk for the development of Blastomycosis. Even though up to date there is no well-developed vaccine for the prevention of Blastomycosis, the risk for the development of Blastomycosis could be reduced by individuals not disturbing the soil. Blastomycosis has existed for millions of years; nevertheless, Blastomycosis, was first described by Thomas Caspar Glichrist in 1894. In view of this, Blastomycosis has sometimnes been called Gilchrist’s disease. The manifestations of Blastomycosis, do cover a wide range of symptoms that overlap with the manifestations of more common conditions and for this reason, Blastomycosis has been referred to as the great pretender. Many cases of Blastomycosis have tended to be asymptomatic or sub-clinical. The involvement of the prostate gland in the form of prostatitis or prostate abscess could be non-specific and this does entail symptoms of dysuria, perineal discomfort, supra-pubic discomfort, visible haematuria, retention of urine and other lower urinary tract symptoms. This non-specific manifestation of Blastomycosis of the prostate gland often tends to result in delay in the correct diagnosis due to the fact that clinicians tend to pursue more common diagnosis including benign prostatic hypertrophy, carcinoma of prostate and actute and chronic bacterial prostatitis. Diagnosis of Blastomycosis is best established by visualization of the distinct yeast within smears, cultures or direct tissue/biopsy specimens. Most clinicians had opinioned that even though acute Blastomycosis could be self-limitinmg they had recommended that treatment with antifungal medication for all cases with utilization of at least 6 months of itraconazole for mild to moderate infectionsand amphotericin for life treatening cases or involvemnent of the central nervous system. Fungal abscesses of the prostate gland or prostatitis are rare pathologies that tend to simulate alternative diagnoses and hence a high-index of suspicion is required to establish an accurate diagnosis and to provide correct treatment. Evethough genitourinary tract involvement of Blastomycosis usually ensues haematogeneous spread, pursuant to pulmonary infections, some patients might manifest with isolated urinary tract symptoms. In view of the fact some patients who have Blastomycoses infection of the prostate gland may manifest with isolated lower urinary tract symptoms, it is pertinent for health care professionals to have a high-index of suspicion with regard to individuals who dwell within or have travelled from Blastomycoses endemic areas that are found to have refactory lower urinary tract symptoms who are not responding to treatment with the usual treatments for lower urinary tract symptoms and bacterial prostatitis. When diagnosis of Blastomycosis prostatitis is confirmed, this should generally be treated for at least 6 months of itraconazole and ensued by regular clinical laboratory and radiology-image follow-up assessment. If a patient has Blastomycosis prostate abscess, the infection should be treated generally by radiology-image-guided complete aspiration / drainage of the abscess plus at lest 6 months treatment with itraconazole and regular clinical, radiology image guided, and laboratory test – follow-up assessments in order to confirm absence of recurrence as well to diagnose any future recurrence early. A high index of suspicion is required in order to diagnose Blastomycoses infection of the prostate gland in both the immunocompetent and immunosuppressed individuals globally especially in North and South America, Canada, Africa and India.
It has been iterated that Blastomycosis is an endemic infection which is caused by Blastomyces dermatitidis, and which is found primarily within the South-Eastern, South-Central, and Mid-West United States of America, with prevalence that has ranged from 0.5 to 4 cases per 100,000 per year. [1] [2] [3] It has been pointed out that Blastomycosis infection often initially manifests with non-specific systemic symptoms which include weight loss, fevers, and fatigue. [1] It has also been documented that majority of Blastomycosis infections do manifest with pulmonary presentations, with rare instances of extra-pulmonary involvement including the skin, central nervous system (CNS), bone, and the genitourinary (GU) system. In addition, it has been iterated that very few cases of blastomycosis infection with initial presentation isolated to the prostate had been reported in the global literature. [1] [4] Considering the fact that Blastomycosis has been reported to occur within some parts of United States of America, Canada, Africa and India and because of global travel of individuals for holidays as well as to settle within other areas of the world, it would be envisaged that Blastomycosis can be encountered anywhere in the world. In view of the rarity of Blastomycosis prostatitis and Blastomycosis prostatic abscess, it would be envisaged that both clinicians and patients globally would tend not to be familiar with the manifestations, diagnostic features, treatment, as outcome ensuing treatment of blastomycosis prostatitis and blastomycosis prostate abscess. There is therefore the need to review and summate experiences that had been reported by few clinicians that had reported cases of blastomycosis of the prostate in order to provide a birds eye view on blastomycosis of the prostate gland to enable both clinicians and patients all over the world to be conversant with the diagnostic features of the infection to help all individuals to have a high index of suspicion for the infection which would enable the establishment of a prompt diagnosis of the infection in order to also enable prompt and effective treatment of the infection. The ensuing article contains a review and update of the literature on Blastomyces prostatitis and Blastomyces prostate abscess which has been divided into two parts (A) Overview which contains General Overview of various aspects of Blastomyces and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to Blastomycoses prostatitis and blastomycoses prostatic abscess.
AIMS:
To review and update the literature on Blastomyces and Blastomyces Prostatitis as well as Blastomyces prostate abscess.
Internet Data Bases were searched including: Google; Google Scholar; PUBMED, Yahoo and AOL. The search words that were used included: Blastomyces; Blastomyces of prostate; Blastomyces Prostatic abscess; Blastomycosis prostatitis; Blastomycosis Prostate Abscess; Blastomycosis prostatic abscess; Blastomycosis abscess of prostate gland. Forty-eight (48) references were identified which were used to write the article which has been divided into two parts: The ensuing article contains a review and update of the literature on Blastomyces prostatitis and Blastomyces prostate abscess which has been divided into two parts (A) Overview which contains General Overview of various aspects of Blastomyces and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to Blastomycoses prostatitis and blastomycoses prostatic abscess.
[A] OVERVIEW
Definition / general statements [5]
The ensuing summations had been made related to the definition and general aspects of Blastomyces: [5]
Essential features [5]
Epidemiology
The ensuing summations related to the epidemiology of the infection had also been iterated: [5]
Sites
Summations related to the sites of Blastomyces infection include: [5]
Pathophysiology
The pathophysiology of blastomycosis had been summated as follows: [5]
Clinical features [5]
Laboratory tests
Haematology blood tests
Biochemistry blood tests
Urinalysis, urine microscopy and culture
Microscopy Pathology Examination
Microscopy pathology examination of specimens containing Blastomyces does demonstrate the ensuing: [5]
Antibody detection tests
Blastomyces antibody detecting tests are available in a number of established laboratory centres but these would tend not to be available within small district centre laboratories. Some of the available tests for the identification of Blastomyces include the ensuing: [5]
The ensuing iterations had been made regarding the treatment of blastomycosis: [5]
Microscopy (histology) description
The microscopy histopathology examination features of specimens of containing blastomycosis infecting agent include: [5]
Immunohistochemistry staining studies
Positive stains
It has been pointed out immunohistochemistry staining in cases of blastomycosis tends to demonstrate the ensuing positive staining findings: [5]
Molecular / cytogenetics description [5]
Differential diagnoses
Some of the documented differential diagnoses of blastomycosis had been documented to include the following: [5]
[B] Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, And Some Studies Related to Blastomocosis Prostatitis and Blastomycosis Prostate Abscess.
Sloan et al. [1] reported a 59-year-old man who had recently been diagnosed as having prostatitis and an elevated serum prostate specific antigen level of (PSA of 9.7), but otherwise he did not have any significant past medical history, who had presented to the emergency department (ED) with urinary retention. A Foley urethral catheter was inserted and the results of her urine culture obtained was negative for urinary tract infection. The patient was discharged with instructions to continue taking tamsulosin, a six-week course of sulfamethoxazole-trimethoprim, and to consult with urology. He was seen in the urology clinic the following week, during which time his symptoms had improved. He underwent digital rectal examination which had revealed a slightly firm non-tender prostate gland. He was advised on management options for his enlarged prostate and his Foley urethral catheter was removed. He was able to void with a residual urine volume of 37mL. He was scheduled to have a repeat serum PSA test 3 months later. Many days subsequently, the patient presented to the Emergency Department after he had developed recurrent urinary retention, as well as night sweats and fevers of up to 102.7 °F. During his presentation, the patient had a temperature of 100.2 °F, but he was otherwise hemodynamically stable. He had a leucocytosis up to 15.5 × 109/L and mild anaemia (haemoglobin 12.8 g/dL). His renal function was at baseline (creatinine 1.0. mg/dL). His urinalysis revealed 3+ leukocyte esterase, negative nitrites, >182 WBCs, 1+ bacteria, and 19 RBCs. He had a Chest x-ray which revealed a vague opacity that was reported to be concerning for possible early pneumonia, but was otherwise unremarkable. He denied having any upper respiratory symptoms, including cough or shortness of breath. He had a CT scan of pelvis which demonstrated multiple low-density regions within his prostate gland which was reported to be suggestive of a possible abscess (see figure 1). The Emergency Department staff inserted a Foley urethral catheter, as well as obtained blood and urine cultures, and the patient was commenced on broad-spectrum antibiotics.

Figure 1: Enlarged and heterogeneous prostate with low-density regions concerning for prostatic abscesses. Reproduced from: [1]
During his admission to hospital, the infectious disease team was consulted, at which time it had been revealed that the patient had participated in gardening, outdoor work, and he had recently returned from a trip to the Nevada desert. He was continued on ceftriaxone while fungal cultures and antigens to Coccidioides and Blastomyces had been collected. The patient continued to develop intermittent fevers and he had developed occasional nausea and vomiting. He was scheduled to undergo cystoscopy and transurethral resection of the prostate and prostate abscess (TURP). Nevertheless, on the day of his surgery, his fungal urine cultures returned positive for Blastomyces dermatitidis. His surgery was accordingly rescheduled and his antibiotics were discontinued with commencement of oral itraconazole. He had CT scan of his thorax which revealed many pulmonary nodules bilaterally. Forty-eight hours pursuant to commencement of his antifungal treatment, the patient continued to develop intermittent fevers and he had a persistent leucocytosis to 12.1 × 109/L. The decision was made to proceed with the undertaking of cystoscopy and TURP. His intra-operative assessment had demonstrated a normal-appearing urinary bladder and bi-lobar hyperplasia of his prostate gland. Resection of his prostate gland demonstrated friable prostatic tissue with multiple cavities that contained purulent fluid which were sent for pathology examination. The patient remained afebrile post-operatively and his leucocytosis had settled. His urethral catheter was removed and he voided without any problem. He was discharged home the next day with a 12-month course of itraconazole. Pathology examination of his resected prostate and prostatic purulent fluid showed that the final specimen was 6.7grams in weight with pathology demonstrating granulomatous prostatitis with many yeast forms that had features compatible with Blastomyces (see figure 2 and figure 3).

Figure 2: Prostatic tissue demonstrating necrotizing granulomatous prostatitis with numerous yeast forms compatible with Blastomyces species (H&E, 40X magnification). Reproduced from: [1]

Figure 3: Prostatic tissue demonstrating necrotizing granulomatous prostatitis with numerous yeast forms compatible with Blastomyces species (PAS-D Stain, 40X magnification). Reproduced from [1].
It was also reported that the patient was reviewed during his follow-up assessment 1 month pursuant to his surgical operation and it was noted that he was doing well and his post-void residual urine volume was 2mL that had indicated complete emptying of the urinary bladder. He also had follow-up computed tomography (CT) scan of thorax, 3 months pursuant to his surgery which had shown significant improvement with illustration of decreasing size of his remaining pulmonary nodules. He was maintained on itraconazole for 12 months, and at the time of publication of the article, the patient had ceased taking his medications and upon his assessment it was confirmed that the patient was doing well and he was asymptomatic. The authors made the ensuing detailed educative summation: [1]
Wittman et al. [14] reported an otherwise healthy 25-year-old man who had manifested to the emergency department with fevers and left sided testis pain. He had urinalysis which was suspicious for infection and ultrasound scan of his scrotum and scrotal contents was undertaken, which demonstrated hyperaemia of his left testis, and left epididymis which was indicative of left epididymoorchitis. He was also found to have several nodular lesions of his skin upon his back, extremities, as well as scalp. One of these lesions was incised and sent for culture and syphilis RPR, which were negative. His sexually transmitted infection testing was also negative, including HIV. He was treated by means of intramuscular gentamicin and a ten-day course of doxycycline. He reattended the emergency department two weeks later with worsening scrotal pain and he had reported a 20-pound weight loss over the preceding month. His assessment workup revealed a leucocytosis of up to 14 × 109/L and a scrotal ultrasound scan which demonstrated progression of his epididymoorchitis with development of a 1.5 cm scrotal abscess. He had Computed tomography (CT) scan of his pelvis which showed a 6 cm prostate abscess as well as infection within his left sacro-iliacc joint. (see figure 4). He was admitted to the hospital and commenced upon broad-spectrum antibiotics. Concern was high for blastomycosis based upon the appearance of his cutaneous lesions, so a urine Blastomyces antigen test was obtained, which was positive. He was transitioned to intravenous fluconazole treatment. He had computed tomography (CT) scan of thorax and abdomen which showed innumerable pulmonary nodules in a miliary pattern that was adjudged to be consistent with the diagnosis of blastomycosis. He was taken to the operating theatre for scrotal exploration and drainage of the scrotal abscess. Culture of the abscess fluid grew out Blastomyces dermatitidis. The next day he was taken for insertion of a trans-gluteal drain by the Interventional Radiology team into his prostate with drainage of 65 mL of green purulent fluid. Culture of this also grew out Blastomyces dermatitidis. His trans-gluteal drain was removed 3 days subsequently following the recording of minimal drainage output. He was transitioned to oral itraconazole for a total of 12 months of treatment. He had a repeat urine Blastomyces antigen test which was negative 9 months after commencement of his treatment.

Figure 4: Complex low-density fluid collection with rim enhancement within the prostate concerning for abscess. Reproduced from: [14].
Wittman et al. [14] made the ensuing educative iterations:
Wittman et al. [14] made the ensuing conclusions:
[17] Neal and Nikolai [17] reported a healthy 51-year-old man who had manifested with a 1-month history of lower urinary tract irritative symptoms. He had urinalysis which was suggestive of infection, and the patient was treated with multiple antibiotics without relief of symptoms. A urology examination demonstrated abnormal induration of his prostate gland. He had biopsy of the prostate gland which upon pathology examination demonstrated features indicative of Blastomyces dermatitidis. He was treated with itraconazole for 6 months. He reported symptom improvement within 2 weeks of beginning treatment. Neal and Nikolai [17] concluded by providing an advice that within areas where Blastomyces dermatitidis is endemic, clinicians should be aware of the presence of this fungus and possible sites of infection.
Busato et al. [18] reported the case of blastomycosis manifesting as epididymitis and prostatitis. The diagnosis was suggested based upon pathology examination of a prostate biopsy specimen of a man who had manifested with lower urinary tract symptoms (LUTS) and that was confirmed by culture. Special staining was utilized to identify Paracoccidioides brasiliensis in the prostate tissue. Despite the treatment the patient died. Busato et al. [18] made the ensuing iterations:
Inoshita et al. [19] reported upon 2 patients who had manifested with prostatic involvement as the first prominent clinical manifestation of systemic blastomycosis. The clinical symptoms of both patients had commenced with dysuria and urinary retention. In 1 patient skin his lesions had developed 4 weeks later and his initial chest x-ray findings were positive. The other patient became aware of skin lesions concurrently with his urinary tract symptoms and he had negative chest x-ray findings. Successful treatment of the patients consisted of amphotericin B in 1 case and ketoconazole in the other case. A review of the literature had revealed 8 well documented cases of blastomycosis with the initial manifesting symptom of prostatic involvement. A summary of the previously reported cases was presented and the importance of recognition of skin lesions in such patients was stressed by the authors.
Labastida et al. [4] reported A 70-year-old man, who was born and raised within a rural community (Cerralvo) in the north-eastern Mexican state of Nuevo León, who had stated in his medical interview that he had not had any pathology history of diabetes mellitus, high blood pressure, or any immunodeficiency. he stated that he was a farmer and he had denied having travelled to other regions of North America over the preceding recent years. His deficient hygiene habits were apparent, but his nutritional status was adequate. He attended the emergency room due to him having acute urinary retention and urinary bladder distention. and he had presented with having irritative and obstructive urinary symptoms over the preceding 6 months. During his clinical examination a Grade II-III prostate gland was found. A Foley urethral catheter was inserted and 1500cc of urine was drained. He was discharged with an appointment at the urology outpatient clinic. Ten days subsequently the patient was re-admitted to the emergency room manifesting with fever, pallor, and visible haematuria. His laboratory tests abnormal findings included neutrophilia upon complete blood count and a serum PSA of 8.3 ng. He underwent trans-rectal ultrasound scan which had shown a marked distention of his urinary bladder and a urinary bladder calculus. his prostate gland had shown a moderate increase in size measuring 4.76 cm x 5.3 cm x 4.4 cm and a volume of 59.4 cc, with heterogeneous echogenicity and borders with a lobular appearance. The initial clinical diagnosis was benign prostatic hypertrophy which was complicated by acute prostatitis; nevertheless, in view of the increase in his serum PSA level and the ultrasound characteristics, a trans-rectal biopsy (TRB) of his prostate gland was decided upon to exclude other prostate pathologies, mainly carcinoma. Utilizing the traditional haematoxylin and eosin technique, the histopathology TRB sections had demonstrated a predominantly lymphocytic inflammatory process, with scarce epithelioid histiocytes which had clumped together and which had formed granulomas; giant cells were also found. (see Figure 5 and figure 6).
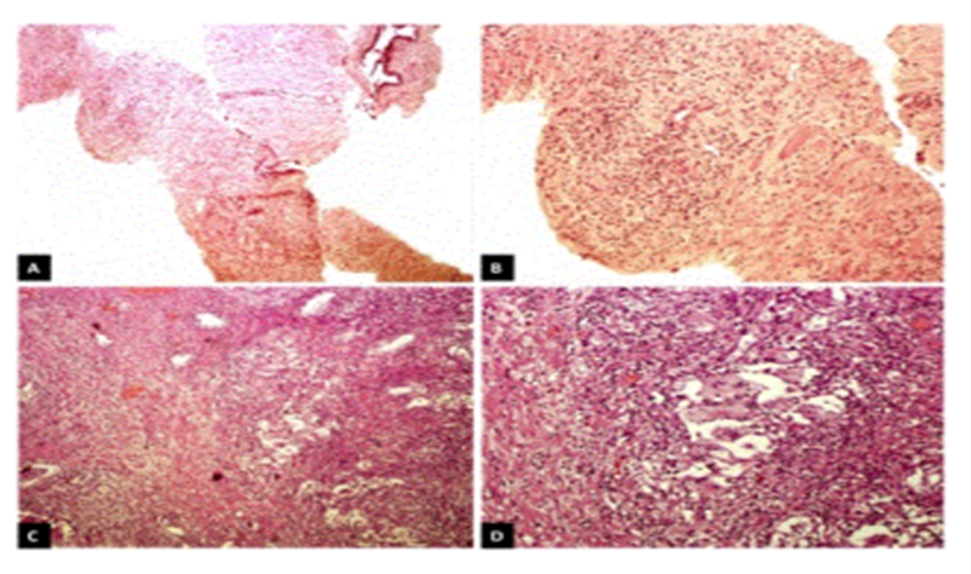
Figure 5: A. Microscopic photograph of transrectal biopsy (x5); in this image scattered inflammatory infiltrate in the stroma predominates. B. At a higher magnification (x10) granuloma with giant cells was identified. C. Histologic panoramic image (x5) of transurethral resection; an inflammatory process is evident in the stroma and surrounding the prostate glands. D. Close-up (x10) to observe the granulomas and giant cells. Reproduced from: [4]

Figure 6: A. Close-up (x40) of multinucleated giant cells with yeast fungal structures in the interior. B. In this Grocott staining, the morphologic characteristics of fungal structures, which characteristically show an ovoid shape with a variable size of 8 to 15 microns and a wide base budding, are better appreciated. Reproduced from: [4]
Yeast fungal structures were identified within these giant cells and granulomatous formations and Grocott staining was undertaken in order to study the morphological characteristics of these fungal structures; they measured 8 microns to 15 microns in width and had shown broad-based budding. these findings had led to the diagnosis of granulomatous prostatitis which was associated with fungal structures that were consistent with the diagnosis of blastomycosis. The diagnosis was confirmed by the undertaking of molecular biology techniques. Total genomic DNA was extracted from a slice of paraffin-embedded tissue which then underwent PCR to amplify fungal ribosomal RNA sequences (ITS1-5.8S ribosomal RNA-ITS2) with the ITS4 (TCCTCCGCTTATTGATATGC) and ITS5 (GGAAGTAAAAGTCGTAACAAGG) consensus primer set [20] The amplification product of 666 base pairs (bp) were sequenced for both borders, assembled, and utilized as a hook in the Basic Local Alignment Search Tool (BLAST) of the NCBI. The results were 100% Ajellomyces dermatitidis (anamorph Blastomyces dermatitidis). Radiology imaging studies were ordered and the patient underwent a thorough clinical examination to exclude a systemic condition. Pulmonary involvement was intentionally evaluated and radiology imaging studies and examination had not identified no abnormalities. The patient commenced medical treatment with 400 mg daily of itraconazole orally for 6 months. After one week of his treatment the patient had demonstrated slight improvement, but due to the persistence of the obstructive symptoms, it was decided to undertake a transurethral resection of the prostate (TURP). Histological tissue sections from the TURP specimen had shown the same findings which had been previously described in the TRB, which had supported the diagnosis of granulomatous prostatitis due to prostatic blastomycosis. the TURP had resolved the obstructive urinary symptomatology and the patient was discharged from the hospital to continue his treatment as an outpatient for at least 6 months. He was asymptomatic at his last follow-up visit prior to publication of the article.
Diagnostic confirmation via molecular biology was strength of their reported case. It did not require fresh tissue and was undertaken out from paraffin-embedded tissue. The methodology employed was based upon amplifying sequences that are common among fungi and customarily utilized for conducting phylogenetic studies.
Labastida et al. [4] made the ensuing conclusions:
Conflict Of Interest – Nil
Acknowledgements
Acknowledgements to:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
