
Research Article | DOI: https://doi.org/10.31579/IJBR-2021/064
1. AGH – University of Science and Technology, Cath. Mineralogy, Petrography and Geochemistry, al. Mickiewicza 30, 30-049 Kraków, Poland.
*Corresponding Author: Maciej Pawlikowski, AGH – University of Science and Technology, Cath. Mineralogy, Petrography and Geochemistry, al. Mickiewicza 30, 30-049 Kraków, Poland.
Citation: Pawlikowski M. (2022) Biomineralogy of Kidney Stones Crystallization. International J. of Biomed Research. 2(4): DOI: 10.31579/IJBR-2021/064
Copyright: © 2022, Maciej Pawlikowski, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 January 2022 | Accepted: 23 March 2022 | Published: 23 April 2022
Keywords: biomineralogy; kidney stones; biomineralization
One of the unsolved mysteries is why kidney stones are formed, for example, in one renal pelvis, while other pelvises are not subject to the process of biomineralization, i.e. crystallization on biological media. Stones also crystallize in the ureters and bladder. The study presents details of the crystallization of kidney stones in a place that mineralogy calls the crystallization center. This publication discusses the method of crystallization of stones and their structure.
The basis for understanding the issues of the formation of uric stones and the treatment of kidney stones is answering the questions related to the initiation of crystallization in the renal pelvises (1-24). This applies to both the formation of the so-called crystallization centers, in which stone formation is initiated, and the causes of excessive urine mineralization. Both issues are decisive in the development of urolithiasis. This article presents the results of many years of mineralogical and chemical studies of these phenomena.
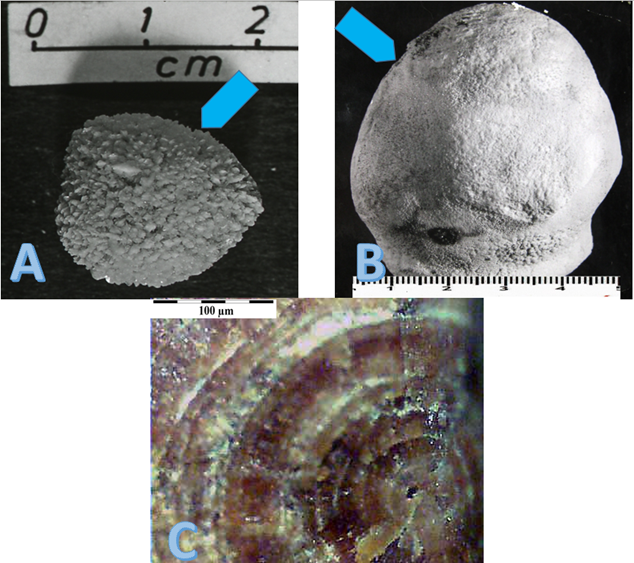
Biomineralogical studies regarding the formation of kidney and bladder stones, recurrent stones and mineralogy of the stones themselves have been conducted at AGH – University of Science and Technology in Krakow – since the 1970s. About 800 stones were examined during this time. The studies prove that urinary stones start to crystallize in crystallization centres. A crystallization center is a place where the surface of the wall of the renal pelvis is damaged (Fig. 1). This damage may be caused by crystals crystallizing from excessively mineralized urine. The edges of these crystals, as they pass through the kidney pelvis with urine, can mechanically damage the pelvic wall, "cutting" the tissues and causing bleeding that appears in the urine. The factor that damages the pelvic wall may also be microorganisms that infect the urinary system (Fig. 1, B.1.). The toxins produced by them in their life processes are aggressive chemicals that can damage the pelvic wall, among other things. There may also be genetic defects in the biological, atomic structure of the pelvic wall, passed down through generations.
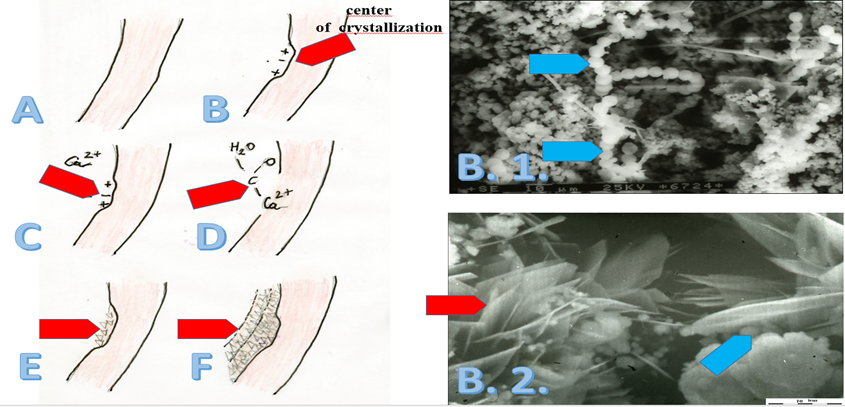
All these damages, regardless of their genesis, lead to the occurrence of "broken" interatomic bonds in the crystallization center, in biological structure of the pelvic wall. This leads to the formation of free, electrically charged bonds. These charged bonds "catch" cations and anions from the urine. Upon attachment to the biological structure, the attached ions become initiators of stone crystallization (Figure 1, B.2.). Further attachment of calcium, CO2 groups, etc. causes further growth of a staghorn stone that "copies" the shape of the renal pelvis (Figure 1, B.–F.).
Development of such mineralization in the crystallization center may be caused by increased urine mineralization, e.g. as a result of a malfunctioning kidney causing excessive re-sorption of water from the urine. The causes of excessive urinary mineralization may also be due to processes outside the kidneys. These include "overproduction" of PTH, i.e. disorders of the parathyroid and thyroid glands. It results in the removal of Ca, but also P from the bone. The excess of Ca2+ in the blood plasma may also be the result of diseases, including inflammation, but also neoplastic changes. The effect of excessive pancreatic calcium bicarbonate synthesis is unknown. Their excessive amount that enters the duodenum along with pancreatic juice may, through intestinal absorption, increase the level of ionized calcium in the blood.
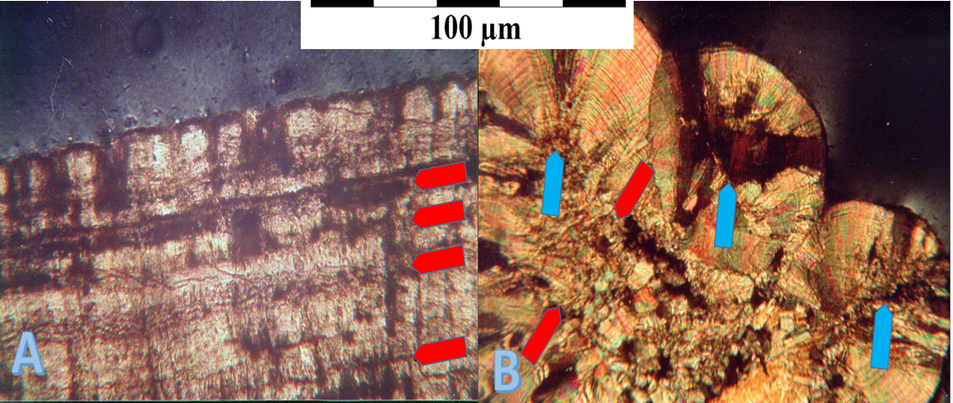
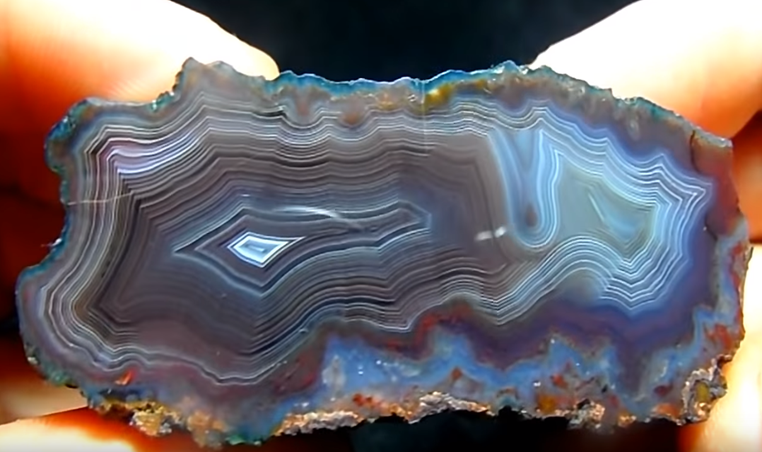
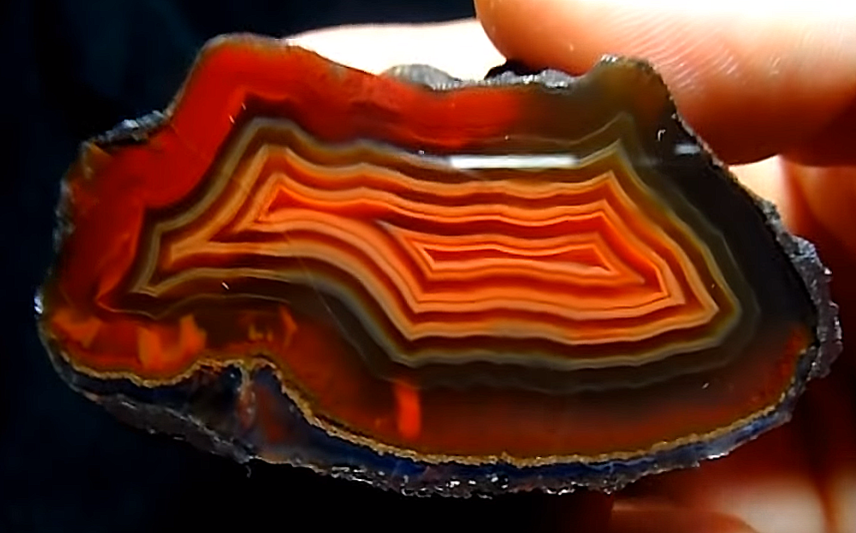
The stones growing cyclically in the renal pelvis (Figure 2, A, B) have the structure of wet sand. They can break down quite easily under the influence of natural or artificially induced shocks (lithotripsy). This applies especially to "young" stones, because "old" stones harden when recrystallized, which makes breaking them much more difficult.
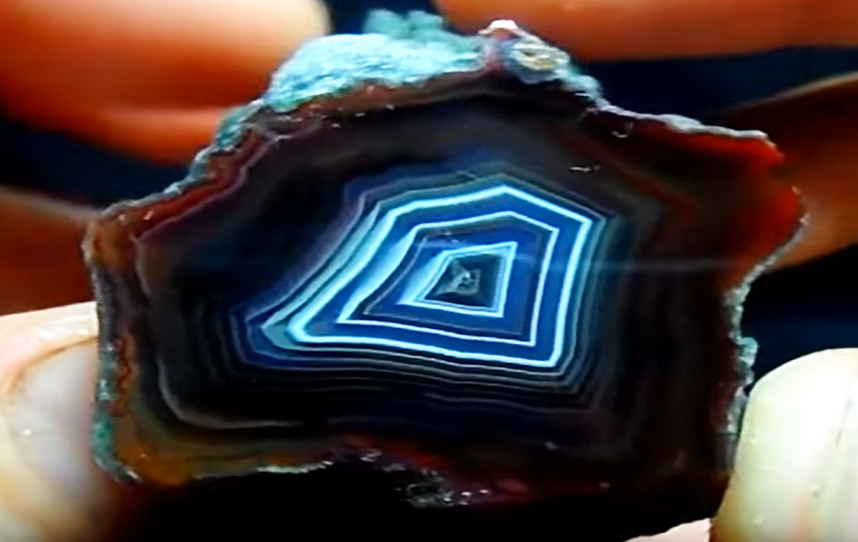
The "kidney sand" left after disintegration or breakdown of stones is flushed out by the urinary system. However, if a grain of "sand" remains in the ureter or bladder (Fig. 3 A., A.1., A.2., A.3., B, C, D), it may form another center of crystallization, where minerals crystallizing from urine (oxalates, phosphates, urates, etc.) keep growing.
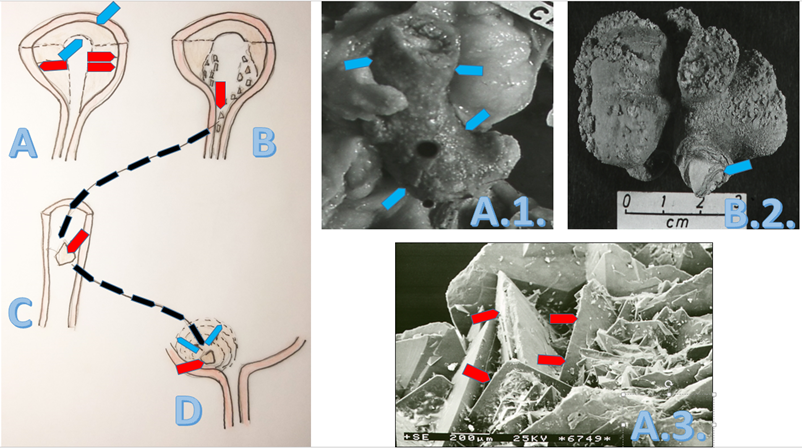
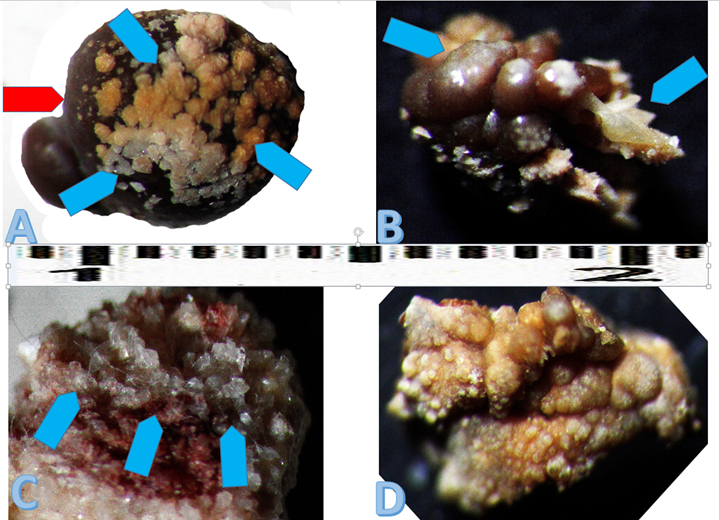
The stone that forms in the ureter on a grain of kidney sand hinders the flow of urine from the kidney to the bladder (Fig. 4). The stone may, after reaching the appropriate size, close the urine outflow (Figure 5).
Disintegration or breakdown of a kidney stone in the renal pelvis is not a guarantee that the problem of recurrent crystallization will be fully solved. Removal of the stones eliminates pain, blockage of urine flow, etc., but to deal with recurrent urolithiasis, liquidation of the crystallization center in the renal pelvis and reduction of excessive urine mineralization must be achieved. The decision how to do that is up to the doctors.
Mineralogical studies of kidney stones provide a large amount of information important in their diagnosis and treatment. The obtained results indicate that crystallization of stones in the renal pelvis begins at a site where its wall has been damaged. It may be the result of mechanical damage caused by crystals crystallizing from urine. The damage can also be caused by aggressive compounds formed during infection, produced by various microorganisms that infect the urinary system.
One or more crystallization centers may form and be subsequently mineralized. The place where damage to the pelvic wall forms, i.e. the formation of the crystallization center, is accidental.
Research indicates that there is a need for standard analysis of kidney stones and sharing the results with a urologist. Further research on urolithiasis should focus on experimental dissolution of stones in vitro and on selecting substances that block crystallization centers of stones, which will prevent recurrence of urolithiasis.
A separate scope of research should be diagnosis of non-renal causes of excessive blood and, consequently, urine mineralization, from which kidney stones crystallize.





Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
