
Review | DOI: https://doi.org/10.31579/2693-2156/024
* Professor of Physiology and Medicine, Nabanji Medical Centre, Lusaka, ZAMBIA.
*Corresponding Author: Nightingale Syabbalo, Professor of Physiology and Medicine, Nabanji Medical Centre, Lusaka, ZAMBIA.
Citation: Nightingale Syabbalo (2021). Biologics in the Treatment of Severe Uncontrolled Asthma in Children. J Thoracic Disease and Cardiothoracic Surgery, 2(2); DOI:10.31579/2693-2156/024
Copyright: © 2021, Nightingale Syabbalo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 June 2021 | Accepted: 17 June 2021 | Published: 30 June 2021
Keywords: airway remodeling; biologics; childhood asthma; interleukins; eosinophilic asthma; severe exacerbations; pathophysiology; obesity
Asthma is the most common chronic disease in children, currently affecting about 7 million children. Severe uncontrolled asthma is rare in children with a prevalence of about 2.1% to 5%, but inflicts a disproportionate health burden. Children with severe asthma have increased risk of life threatening exacerbations, frequent hospitalization, worsening health-related quality of life, and impaired physical activity. Severe asthma in childhood is associated with long-term morbidities, such as bronchiolitis obliterans, impaired airway development, and development of chronic obstructive pulmonary disease in adulthood. Childhood asthma like adult-onset asthma, is classified into four cellular inflammatory phenotypes using induced sputum cytometry. The four phenotypes of asthma include eosinophilic asthma, neutrophilic asthma, paucigranulocytic asthma, and mixed cellularity asthma. The pathophysiological mechanisms of asthma involve airway inflammation and remodeling. Inflammatory mediators such as cytokines, chemokines, adhesion molecules, and growth factors play a key role in orchestration airway remodeling. During airway inflammation, cytokines secreted by type 2 helper (Th2) lymphocytes, such as interleukin-5 (IL-5), IL-4, IL-13, IL-25, IL-33, and thymic stromal lymphopoietin (TSLP) play a key role in the pathogenesis of eosinophilic asthma. Whereas, the Th17 axis cytokines, including IL-17, IL-23, and IL-8 are responsible for the pathophysiology of neutrophilic asthma. The airway structural changes due to airway remodeling lead to thickening of the airway wall, narrowing of the bronchiolar lumen, airway obstruction, and decline in pulmonary function. Most of the children with asthma respond to low and medium inhaled corticosteroids, however a significant proportion still have severe asthma uncontrolled on the standard of care. The most common asthma phenotype in children is eosinophilic asthma, which responds superbly to biologic therapy. Children with severe asthma require add-on targeted interleukin antagonists (ILA), such as mepolizumab (anti-IL-5), benralizumab (anti-IL-5Rα), and dupilumab (anti-4Rα). ILAs have been shown to ameliorate asthma symptoms, reduce moderate and severe exacerbations, and improve pulmonary function. Additionally, ILAs have been demonstrated to improve the health-related quality of life, and have steroid sparing effect.
Asthma is a significant public health problem, affecting more than 358 million people globally [1], and is the most common chronic disease among children [3,4], affecting about 7 million children [4]. Asthma is a heterogeneous chronic airway disease with several distinct phenotypes characterized by different immunopathological pathways, clinical presentation, physiology, co-morbidities, biomarker of allergic inflammation, and response to treatment [5-10]. There are four cellular inflammatory phenotypes of asthma classified using induced sputum cytometry. The four phenotypes of asthma include eosinophilic asthma, neutrophilic asthma, paucigranulocytic asthma, and mixed cellularity asthma [7,11]. Patients with eosinophilic asthma have an eosinophil count ≥3% [12-14], whereas patients with neutrophilic asthma have elevated sputum neutrophil count between ≥61% [14,] and ≥64% [15], depending on the study. Mixed cellularity phenotype is typified by increase in both eosinophils (>3%), and neutrophils (>61% or >64%) [15]. Paucigranuocytic phenotype includes patients with very few eosinophils (<3>
Approximately 40-60% of patients with severe asthma have eosinophilic phenotype [17-21], whereas, the remaining patients have the non-eosinophilic phenotype. Eosinophilic asthma is the most common phenotype in children presenting with severe acute asthma; representing about 50% of the patients [22,23]. Paucigranulocytic asthma is most common in children and adults with stable asthma [23], however, acute severe neutrophilic asthma is most common in adult patients [22,23].
The pathophysiological mechanisms of asthma involve airway inflammation and remodeling. Inflammatory mediators such as cytokines, chemokines, adhesion molecules, enzymes, and growth factors play a key role in propagating airway remodeling. During airway inflammation, cytokines secreted by type 2 helper (Th2) lymphocytes, play a key role in the pathogenesis of Th2-high eosinophilic asthma. On the other hand, the Th17 axis cytokines are responsible for the pathophysiology of Th2-low neutrophilic asthma [24].
Most children with asthma respond to low and moderate doses of inhaled corticosteroids (ICS). However, about 5% of children have severe uncontrolled asthma despite maximal standard of care, including high dose ICS, which are associated with serious side effects. Children with severe uncontrolled asthma require add-on biological treatment, such as omalizumab (anti-IgE), mepolizumab (anti-IL-5), benralizumab (anti-IL-5Rα), and dupilumab (anti-4Rα). ILAs have been shown to ameliorate asthma symptoms, reduce moderate and severe exacerbations, and improve pulmonary function. Additionally, ILAs have been demonstrated to improve health-related quality of life, and have steroid-sparing effects [25]. This review highlights targeted treatment of severe uncontrolled asthma using the currently approved biologics for the treatment of childhood asthma.
Pathophysiology of Asthma
The pathophysiology and immunological mechanisms in the pathogenesis of childhood asthma and adult-onset asthma are basically similar. Airway inflammation and remodeling plays a key role in the pathogenesis of childhood asthma. During airway inflammation, cytokines secreted by type 2 helper (Th2) lymphocytes (CD4+), and innate lymphoid cells group 2 (ILC2), such as interleukin-5 (IL-5), IL-4, IL-13, IL-25, IL-33, and thymic stromal lymphphopoietin (TSLP) play an important role in the pathogenesis of eosinophilic asthma [26-36]. On the other hand, Th17 cytokines (IL-17, IL-17F), IL-23, and IL-8 play a pivotal role in the pathophysiology of neutrophilic asthma [24, 37-39]. However, there is some cross-talk between the Th2 and the Th17 axes in the pathogenesis of asthma [40]. Several excellent schematic diagrams on the mechanisms and characteristic pathological features of asthma immunopathology are given elsewhere [41].
Inflammation cells, such as eosinophils, mast cells, neutrophils, basophils, and structural cells including epithelial cells, fibroblasts, myofibroblasts, and airway smooth muscle (ASM) cells also secrete inflammatory cytokines, chemokines, adhesion molecules, enzymes, and growth factors which orchestrate airway remodeling. Airway remodeling is an active process which occurs early in childhood asthma [42-45], and correlates with the severity of asthma [46-48], and is associated with fatal pediatric and adolescent asthma [49]. It occurs in both eosinophilic and non-eosinophilic asthma [50].
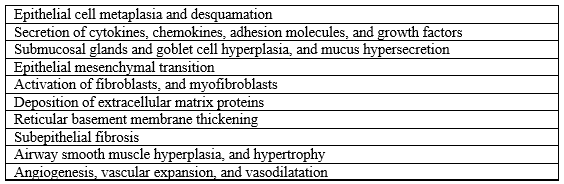
Airway remodeling is a complex pathophysiological process involving structural changes, such as epithelial cell metaplasia and desquamation [51]; deposition of extracellular matrix proteins by fibroblasts and myofibroblasts [52-55]; thickening of the reticular basement membrane [42,52]; subepithelial fibrosis [56]; ASM cells hyperplasia and hypertrophy [57]. Additionally, airway remodeling is accompanied by submucosal glands and goblet cells hyperplasia, and mucus hypersecretion [58,59]; and angiogenesis [50,60]. The structural changes lead to thickening of the airway wall, airway narrowing, excessive bronchoconstriction, and severe, uncontrolled asthma. Table 1 summarizes the pathophysiologic mechanisms of airway remodeling in severe childhood asthma.
Childhood Asthma
Asthma is the most common chronic disease in childhood, affecting about 10-15% of school-age children [61]. It is most common in boys [1,62]. Severe uncontrolled asthma in children only accounts for 2 to 5% of childhood asthma [63-65], but contributes to huge costs, and utilization of health care resources [66,67]. Severe asthma is associated with significant morbidity, such as increased risk of life threatening exacerbations, frequent hospitalization, worsening health-related quality of life, and impaired physical activity [68-70]. Severe asthma in children may impair airway development and reduce maximally attained lung function, and the lung function loss may persist in adult life [62]. It is also associated with long-term morbidities, such as bronchiolitis obliterans [71]; progressive airflow limitation [70]; and development of chronic obstructive pulmonary disease in adulthood [72-75]. Furthermore, children with asthma are more susceptible to medication-related side effects, particularly with the new biologics [75].
Asthma in children is associated with co-morbities [76,77], such as allergic rhinitis [78,79], chronic rhinosinusitis and nasal polyps [80,81], atopic dermatitis [82,83], gastroesophageal reflux disease [84,85], obstructive sleep apnea [86,87], food allergy [88], and obesity [89,90]. Obesity is associated with decreased response to inhaled corticosteroids in overweight and obese asthmatic children [91]. Co-morbid diseases associated with asthma may make asthma control difficult, they require medical and/or surgical treatment [36].
Children with severe asthma have elevated biomarkers of Th2 eosinophilic inflammation, such as high sputum and blood eosinophil counts, high IgE levels [92-94], high fractional exhaled nitric oxide (FeNO) [95,96], and elevated serum periostin concentration [92]. Biomarkers of eosinophilic inflammation should be assessed for selection of asthmatic children for add-on treatment with biologics [96,97]. Children with persistent symptoms, and exacerbations despite correct inhaler technique and adherence should be referred to an asthma specialist with expertise in severe asthma [70].
Treatment of Severe Asthma in Children
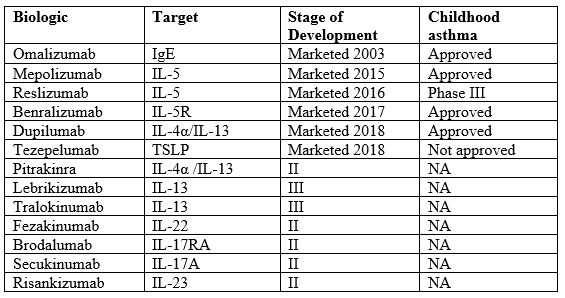
Childhood asthma is usually controlled with low to moderate doses of inhaled corticosteroids. However, about 5% of children experience severe uncontrolled asthma despite maximal standard of care, including high dose ICS (GINA steps 4 and 5) [1]. High dose ICS have serious side effects in children including impaired growth velocity, decrease bone mineral density, and pneumonia. Children with severe uncontrolled asthma may require targeted add-on biologic treatment, which has been available for adults since the approval of omalizumab (Xolair®) on June 30, 2003. Although most of the clinical trials on biologics have been conducted in adult patients with asthma [98], biologics are very effective and safe as add-on treatment for severe eosinophilic asthma in children. Currently, there are four biologics which have been approved for add-on treatment of severe childhood asthma [99]. They include omalizumab (anti-IgE) [100,101], mepolizumab (anti-IL-5) [102,103], benralizumab (anti-IL-5Rα) [104,105], and dupilumab (anti-4Rα) [106,107]. Table 2 shows the list of the current approved biologics for the treatment of childhood asthma, and some ILAs still in development, or phased out of the clinical trials.
Add-on biologics have been shown to reduce asthma symptoms, decrease moderate to severe exacerbations, and improve pulmonary function in children with severe asthma [108-114]. Additionally, biologics improve health-related quality of life, and have been used to taper or stop oral corticosteroids in patients with severe asthma [102,104,115]. The dosages of the currently approved biologics by the US Food and Drug Administration (FDA) are shown in Table 3.
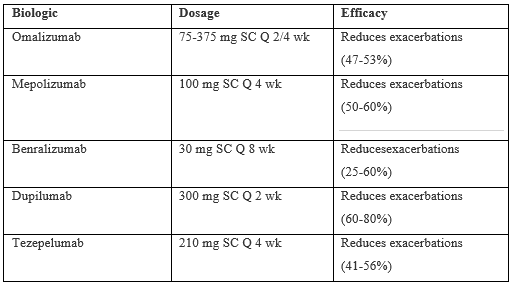
Children and adolescent dosages vary with age and weight of the patient, and also vary with authors.
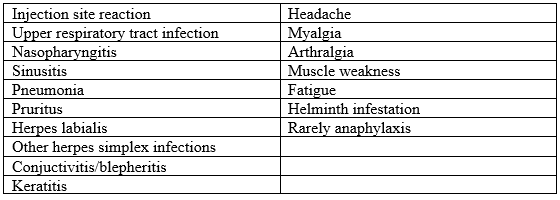
Biologics are safe for add-on treatment of severe asthma in children. They have almost similar manageable side effects because of their immunological effects on eosinophils, and other systemic effects, such as injection site reaction, respiratory tract infection, nasopharyngitis, sinusitis, conjunctivitis, headache, arthralgia, myalgia, muscle weakness, parasitosis, and rarely anaphylaxis (Table 4) [36].
Eosinophils play an important role in protection against parasitic infection, including helminth infestation. Patients with pre-existing helminth infections should be treated for the infection before initiating biologic therapy. If individuals become infected whilst receiving treatment with biologics and do not respond to anti-helminth treatment, temporary discontinuation of the biologic should be considered [36].
Notably, some of the biologics, such as omalizumab, and dupilumab also ameliorate, and are approved for the treatment other co-morbid conditions associated with childhood asthma, such as allergic rhinitis, chronic rhinosinusitis with nasal polyps, and atopic dermatitis [116-119]. Dupilumab (Dupixent®) has been nicknamed “magic bullet’’ because it is the only biologic which has been approved by the FDA for the treatment of eosinophilic asthma [117,118]; chronic rhinosinusitis with nasal polyps [117,119]; atopic dermatitis [117,120]; and eosinophilic esophagitis [118,121,122].
The different immunopathological pathways of dupilumab in the treatment of asthma, allergic rhinitis, atopic dermatitis, and chronic rhinosinusitis are explained in detail elsewhere [123]. Dupixent® has been shown to be very effective and safe in the treatment of these conditions, and to improve the quality of life in children and adults [124].
The latest approved biologic for the treatment of severe refractory asthma is telezepelumab [125,126]. Tezepelumab is a fully human monoclonal Ig2ʎ antibody that specifically ligates TSLP by binding to its receptor TSLPR, thereby blocking human TSLP-TSLPR interaction [127]. Menziew-Gow et al. [128] have shown that tezepelumab significantly reduces the annualized asthma exacerbation in adolescent and adult asthmatics by 56% in patients with eosinophil count ≥ 300 cells.µl1, and by 41% in patients with eosinophil count < 300>
Severe, uncontrolled childhood asthma may also be treated with Complementary and Integrative Medicine (CIM), including Traditional Chinese Medicine (TCM). In order to treat severe asthma, one must understand the function of the body as a whole, in its energy level [131]. Oriental Medicine theories, such as Yin Yang and Five Elements, aligned with homeopathy may be used to achieve treatment success of severe asthma [132]. Traditional Chinese Medicine using the theory of Five Elements (wood, fire, earth, metal, and water), and Yin and Yang theory may improve the symptoms of asthma, improve whole physical, mental, and emotional picture of children with asthma [131,133,134]. TCM not only addresses the underlying condition of the patient but, also focuses on other body systems, such as the kidney (son) which may worsen lung (Qi, mother) disorders, such as asthma if not treated [131]. Many patients with chronic allergic diseases, such as asthma seek complementary and alternative therapies including Traditional Chinese Medicine. TCM is one of the oldest practice and has been used for many centuries for the treatment of asthma. There are a number of well-controlled studies on Chinese herbal formulas which have been found to be effective, safe, and have immunomodulatory effects on asthma. They include modified Mai-Men-Dong-Tang (mMMDT, five herbs), Ding-Chuan-Tang (DCT, nine herbs), and anti-asthma herbal medicine intervention (ASMI) [135].
The active ingredients in Chinese herbal medicine have multilevel effects by regulating the immunologic equilibrium mechanisms and signaling pathways, thereby regulating the progression of asthma [136]. The possible signaling pathways regulated by the ingredients of TCM herbal medicine include IL-4-IL-13-JAK-STAT-MAP kinases, adiponectin-iNOS-NF-kB, PGD2-CRTH2, PI3K/AKT, T-bet/gata-3, and Fox3-RORγt [137]. All the above signaling pathways are involved in the pathogenesis of asthma [137], and the effects of various ingredients in TCM herbal remedies are illustrated superbly by Wang and coworkers [136].
Asthma is the most common chronic disease in childhood, affecting about 10-15% of school-age children. Severe uncontrolled asthma in children is not common, but contributes to huge costs, and utilization of health care resources. It is associated with significant morbidity, such as increased risk of life threatening exacerbations, frequent hospitalization, and worsening health-related quality of life. Cytokines secreted by Th2 lymphocytes, and Th17 cells, such as IL-5, IL-4, IL-13, IL-25, IL-33, and TSLP; and IL-17, respectively play an important role in the pathogenesis of asthma. Most children with asthma are controlled on low to moderate dose of ICS. However, a significant proportion of children have severe asthma uncontrolled on high dose ICS. Children with severe persistent asthma require add-on treatment with biologics targeting the instigating interleukins. Interleukin antagonists have been shown to reduce asthma symptoms, decrease moderate to severe exacerbations, and improve pulmonary function in children with severe asthma. Additionally, they improve health-related quality of life, and have corticosteroids-sparing effects. Dupilumab is also effective in the treatment of childhood asthma-associated disorders, such as chronic rhinosinusitis with nasal polyps, eczema, and eosinophilic esophagitis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
