
Research Article | DOI: https://doi.org/10.31579/2641-5194/038
1Hepatopancreaticobiliary Unit , Department of General Surgery , Royal Blackburn Hospital, East Lancashire NHS Hospital Trust, Blackburn, Lancashire, UK. BB2 3HH.
2Department of Radiology, Royal Blackburn Hospital, East Lancashire NHS Hospital Trust, Blackburn, Lancashire, UK. BB2 3HH
3Blackburn Research Innovation Development Group in General Surgery, Royal Blackburn Hospital, East Lancashire NHS Hospital Trust, Blackburn, Lancashire, UK. BB2 3HH
*Corresponding Author: Osborne Vaz, Hepatopancreaticobiliary Unit, Department of General Surgery , Royal Blackburn Hospital, East Lancashire NHS Hospital Trust, Blackburn, Lancashire, UK. BB2 3HH.
Citation: Vaz O., Shofiq Al – Islam,Khan Z. ,Neil Wilde , Lowe B.Magilton A Subar D., (2022) Bio-Degradable Stents: Primary Experience in a Tertiary HPB Centre in the United Kingdom. J. Gastroenterology Pancreatology and Hepatobilary Disorders 6(1) DOI:10.31579/2641-5194/038
Copyright: © 2022, Osborne Vaz, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 June 2021 | Accepted: 17 November 2021 | Published: 04 January 2022
Keywords: benign biliary strictures, biodegradable stents, percutaneous transhepatic cholangiography
Background: Management of benign biliary strictures (BBS) post bilioenteric anastomoses requires a multidisciplinary approach including surgical, radiological and/or endoscopic input. Patients often need multiple hospital visits for treatment with the long term possibility of restenosis. Conventionally BBS have been treated with serial percutaneous transhepatic biliary dilatations necessitating repeat procedures for drain exchange or removal Surgery may become necessary in refractory strictures. In the last decade there has been increasing reports of the use of biodegradable stents (BDS) in treating biliary strictures mainly to address the need for repeated procedures for drain exchange.
Aims: This study aimed to report the early outcomes in patients with benign biliary strictures treated with biodegradable stents.
Methods: Retrospective analysis of prospectively collected data was performed of patients who had a bilioenteric anastomosis presenting with an anastomotic stricture and were intended to be treated with BDS. The primary end points reported on were technical success (defined as successful resolution of stricture on repeat cholangiogram) and clinical success (defined as absence of repeated cholangitis). Clavien– Dindo grade of complication were reported.
Results: Twelve patients presented with BBS and nine patients had BDS. Three patients were not considered suitable for BDS stenting due to a non-traversable stricture and had surgery. The male female ratio was 1:2. There was 100% technical and clinical success with one patient having stent migration not needing intervention. The procedure took an average of 45 minutes. In seven (77.7%) patients, it was safely performed under local anaesthesia with sedation. Two patients preferred general anaesthesia. There was no restenosis noted at a median follow up of 11 months.
Conclusion: The use of BDS in the treatment of BBS is a safe and effective procedure. Longer term follow-up with multi-institutional reporting on a national database is needed to assess its long term benefits.
CBD: Common Bile Duct.
BBS: Benign biliary stricture
BDS: Biodegradable stent.
ERCP: Endoscopic Retrograde Cholangiopancreatography.
HJ: Hepaticojejunostomy
LC: Laparoscopic cholecystectomy
PTBD: Percutaneous transhepatic biliary dilatation.
PTC: Percutaneous transhepatic cholangiography.
Benign biliary strictures (BBS) post bilioenteric anastomosis are seen in 2.6% - 17% of patients [1]. Those due to injuries post laparoscopic cholecystectomy (LC) are seen in 0.3% to 0.7% of patients [2,3]. Management requires a multidisciplinary approach including cross abdominal imaging including magnetic resonance cholangiopancreaticography (MRCP) and or computerised tomography (CT). These help delineate the anatomy with respect to location, number of strictures, length and associated anatomical anomalies including vascular injuries. While there is no standard accepted classification for BBS, the application of the Bismuth classification in BBS may assist in clinical treatment decision making [3].
Historically surgery was the only option but since the 1970s non operative management is generally now considered the first treatment of choice [4 - 6]. It is less invasive, has lesser morbidity and shorter hospital stay when compared to surgery [6]. The success rates are comparable to surgery [6].However there is no gold standard in treatment of BBS.
In patients with no prior bilioenteric anastomosis endoscopic retrograde cholangiopancreatography (ERCP) conventionally remains the first intervention of choice 3. However, in those with an altered anatomy due to bilioenteric anastomosis or an endoscopically non traversable stricture, percutaneous transhepatic cholangiography with biliary decompression (PTBD) is the first intervention of choice [4,7]. PTBD has been reported to be less invasive and pose lesser risk than surgery [2, 8]. However, classically PTBD needs repeated procedures to sequentially upsize the drains and serially dilate the stricture which has led to the increasing interest in the use of biodegradable stents (BDS). Placement of BDS has many advantages over PTBD as it removes the need for repeated procedures, improves quality of life as the patient has no external drainage catheter to manage and reduces the risk of complications associated with external drainage [9].
The aim of this study was to report the early outcomes in patients with benign biliary strictures treated with biodegradable stents.
This is an observational study with retrospective analysis of prospectively collected data at a tertiary HPB centre in the United Kingdom.
All patients who had a request for radiological treatment of a biliary stricture with BDS between January 2017 to June 2020 were recorded on a database. These patients were considered potentially suitable for BDS after a multidisciplinary team discussion. Patient details were acquired from the records of the radiology and surgical departments of the hospital. The details of the procedure were accessed from the procedure notes kept in the patient records and the electronic patient record (EPR) system. Details on follow up were accessed via the EPR and outpatient clinic notes.
The stent used was a polydioxanone stent and all were custom made and procured from SX-ELLA ®, S.R.O, Hradec Kralove Czech Republic. All stent insertions were done by qualified interventional radiologists.
The protocol followed for the patients with biliary stricture was cross sectional abdominal imaging, followed by a per cutaneous transhepatic cholangiogram with biliary decompression (Fig 1 demonstrating a stricture seen on MRCP). The patient then underwent serial dilatations with up- sizing of the external drain to 16Fr. If the stricture persisted, they were considered for insertion of a BDS. The dilated stricture was mapped for dimensions and a custom-made stent procured from the aforementioned company. The procedure was performed by two interventional radiologists. Post BDS placement, a check cholangiogram was carried out after 7 days. (Figure 2 cholangiogram post stent placement) The external biliary drain was removed if the cholangiogram was satisfactory and the stent tract filled with Avitene ® for haemostasis and reduce the chances for bile leak.
Descriptive statistical analysis was done for all patients. Variables included age, gender, and primary surgical procedure, number of PTBDs, attempts at BDS placement, technical and clinical success, complications and follow up. The complications included but not limited to bleeding, bile leak, drain displacement, cholangitis, drain obstruction, vascular injury, biliary peritonitis, injury to intra-bdominal viscera and pleural complications. The Clavien Dindo (CD) classification was used to categorise grade of complication.
There were twelve patients identified with benign biliary strictures, eleven of whom had bilioenteric anastomosis. One patient had a common hepatic duct stricture post laparoscopic cholecystectomy.

Three patients did not qualify for a BDS. In these three patients the bilioenteric stricture was refractory to PTBD and the stricture could not be traversed radiologically. All three patients had a bile duct injury post laparoscopic cholecystectomy, two of whom had undergone a hepaticojejunostomy and has a HJ stricture. All 3 underwent successful redo hepaticojejunostomies with no post-operative complications to date (Table B).


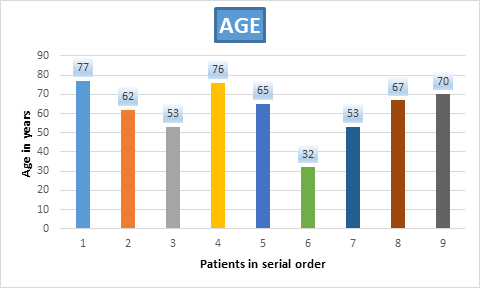
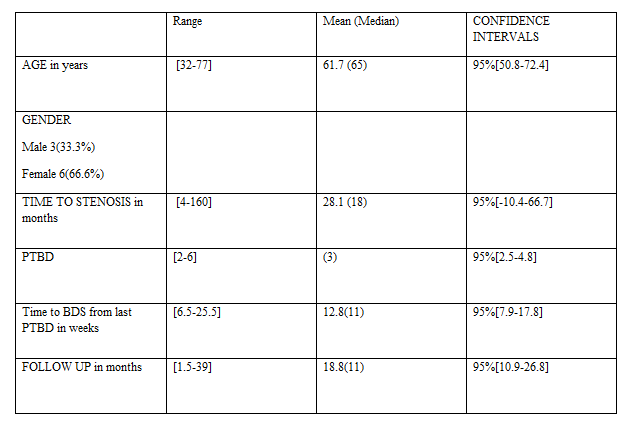
Nine patients had BDS with a male female ratio of 1:2. The median age was 65 years [range 32 – 77 years]. All nine (100%) had undergone a hepaticojejunostomy in the past which had stenosed. Three (33.3%) had a Whipple’s procedure for pancreatic malignancies, one (11.1%) had a reconstruction after right hepatectomy for colorectal liver metastases with Roux en Y reconstruction. The bile duct was not involved with malignancy in any of these patients and there was no evidence of disease recurrence at the time of BDS insertion. Four (44.4%) patients had a CBD injury post laparoscopic cholecystectomy and one (11.1%) had bilio enteric reconstruction post-surgery for Mirizzi’s syndrome (Table B).
The average time to development of anastomotic stenosis was 28.1 months from primary repair [range 4-160]
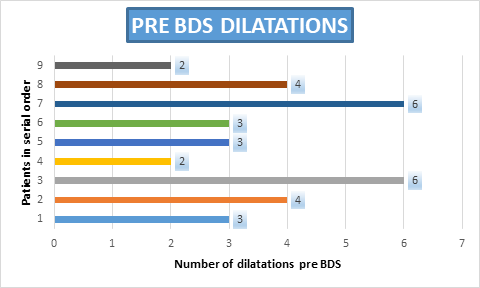
The median number of dilatations needed prior to insertion of the BDS
were three (range 2-6). The median time taken in weeks for stent procurement and insertion from last PTBD was 11 weeks [range 6.5 – 25.5]
Seven (77.7%) of the stent placements were carried out as day case procedures and two (22.2%) had a 24 hour stay. Local anaesthesia and sedation were used in seven (77.7%) of the patients whilst two (22.2%) needed general anaesthesia. the procedure took an average of 45 minutes. Technical and clinical success was 100% .All patients needed only one BDS placement.
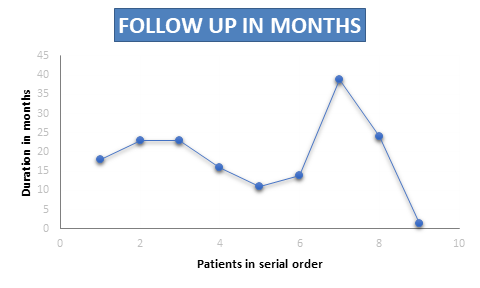
One patient had a stent migration that did not require any intervention (CD1). The median follow-up was 11 months [range 4 – 39 months]. No patients required further intervention and no cholangitis and restenosis were noted at follow up (Table C).
The incidence of benign biliary strictures post bilioenteric reconstruction have been reported in the literature to be between 2.6% - 17% % 1,4 and those post laparoscopic cholecystectomy between 0.3 %– 0.7% 3.
Whilst PTBD with serial dilatations with or without stenting has been the mainstay in BBS post bilioenteric anastomosis [1,5,8,10-12] , there has been an emergence in the use of biodegradable stenting in the past decade [7,9,13-16]
The use of biodegradable stents was first described in interventional cardiology and thereafter in oesophageal and urethral strictures. Recently, there have been increasing reports of its use in the treatment for biliary strictures. This is mainly to address the need for reinterventions to exchange or remove stents and refractory stenosis. [3, 17, 18]
The first published case report of usage of a biliary BDS was via ERCP and demonstrated technical and clinical success [19]. Thereafter these stents have been used for endoscopic treatment of biliary strictures usually post cholecystectomy biliary injuries 3, 17 before gaining usage via the percutaneous methods [9, 13].
Manufacturer studies [7] suggest that the radial strength of the stent is maintained for the first five weeks which gradually recedes to two thirds the initial value at week seven post insertion and one thirds at week nine. The degradation products are not harmful to human tissues. Studies have shown that BDS express proteins which tend to be similar to those observed in intact bile ducts [19-21].
Our study reflects similar outcomes to what is published in the literature to date. The largest study by de Gregorio et al [9] suggests that a stent patency of 78.9% is observed at 60 months. Of those with restenosis, 12% patients needed a second stent and 14.6% needed definitive operative repair. None of their patients had major complications due to stent placements. Another study by Mauri et al [13] also demonstrated similar outcomes with stricture recurrence in 18% of patients with estimated time to re-stricture of 38 months [13].
To the best of our knowledge, this is the largest series in the United Kingdom reported to date.Our study included a small cohort and a short follow up period. The efficiency of the procedure is limited by the unavailability of a local manufacturing source and the fact that stents are made to order. The stents are off label and need a special prescription. The process of stent acquisition and insertion took a median of 11 weeks. There is also special permission needed for cost reimbursement which prolongs treatment time.
The cost of metal stenting is £2900 and each PTC episode pre- and post-stenting costs £890. Bilioenteric bypass surgery costs £13606. Comparitively the average cost of PTBDs followed by BDS insertion in the patients from this study amounted to £7837. BDS is evidently more cost effective than surgery. The cost of multiple plastic stenting and metal stentings increases with each additional procedure. Complications due to repetitive procedures also add to the financial burden in fully covered self-expanding metal stenting and multiple plastic stenting.
Biodegradable stent insertion via percutaneous transhepatic route can safely be performed as a day case procedure, is cost effective and has high success rates. The post procedural complication rates are minimal. These factors contribute immensely to improving patient outcomes and reducing hospital costs. Larger multicentre trials are needed and a consensus needs to be arrived at for standardisation of the selection criteria in what is a small number of patients presenting at any single HPB unit.
The authors of this original paper declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
