
Research Article | DOI: https://doi.org/10.31579/2768-2757/120
1Consultant Surgeon, Department of General Surgery, Prime Hospital, Dubai, UAE.
2Consultant Gastroenterologist, Department of Medical Gastroenterology, Prime Hospital, Dubai, UAE.
3Consultant General Surgeon, Department of General Surgery, Gladstone Queensland Hospital, Perth, Australia.
4Consultant Surgeon, Department of General Surgery, American Hospital, Dubai, UAE.
5Specialist General Surgeon, Department of General Surgery, Prime Hospital, Dubai, UAE.
6Specialist ENT Surgeon, Department of ENT Surgery, Prime Hospital, Dubai, UAE.
7Specialist General Surgeon, Department of General Surgery, Prime Hospital, Dubai, UAE.
8Specialist General Surgeon, Department of General Surgery, Prime Hospital, Dubai, UAE.
9Undergraduate Student UCL, London, UK.
*Corresponding Author: Vinod Kumar Singhal, Consultant Surgeon, Department of General Surgery, Prime Hospital, Dubai, UAE.
Citation: Vinod K Singhal., Diddi G., Faris D Alaswad., Moussa H., Suleman A., et al. (2024), Bile Duct Injury in Laparoscopic Cholecystectomy; A Multi Centre Experience, Journal of Clinical Surgery and Research, 5(3); DOI:10.31579/2768-2757/120
Copyright: © 2024, Vinod Kumar Singhal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 March 2024 | Accepted: 25 March 2024 | Published: 08 April 2024
Keywords: bile duct injury, laparoscopic cholecystectomy, strasberg classification ecrp, ptc and ryhj
Background: Laparoscopic cholecystectomy (LC), a minimally invasive gallbladder removal surgery, has revolutionized the field with benefits like quicker recovery. However, it is not without risks, and bile duct injury (BDI) is a severe but rare complication. BDI incidence during LC varies (0.4%-0.9%), with potentially life-threatening consequences. Surgeon experience, intraoperative cholangiography, and careful handling are crucial in preventing and managing BDIs.
Aim of the study: This study aims to present and analyze a Multi centre experience regarding the management of these bile duct injuries in LC.
Methods: This retrospective study, conducted at UAE medical institutions from 2014 to 2024, analyzed 2400 Laparoscopic Cholecystectomy surgeries over ten years. Out of 18 patients, thirteen patients were treated with ERCP, while five required additional surgery. Inclusion criteria involved patients aged 30 to 70+, of both genders, with BDIs. Exclusion criteria included minor BDIs and comorbidities. Two diagnostic techniques, including intraoperative cholangiography and postoperative assessments, identified BDIs. Treatment varied based on Strasberg classification, involving suturing, ERCP, stent placement, and Roux-en-Y hepaticojejunostomy. Data analysis employed SPSS, presenting results through tables and graphs with statistical parameters.
Result: The study focused on Laparoscopic Cholecystectomy-related Bile Duct Injuries (BDI), with a cohort primarily aged 51-70 (66.67%). This age group showed higher susceptibility to BDI. The average participant age was 55.21±12.54 years, with a male majority (55.56%). Among 18 Endoscopic Retrograde Cholangiopancreatography (ERCP) cases, five had BDI, diagnosed intra/postoperatively. Two patients with clinical symptoms had postoperative diagnosis through Percutaneous Transhepatic Cholangiography (PTC). Strasberg classification revealed 60% Type A injuries; Types E1 and E2 each constituted 20%. Treatment modalities varied, with ERCP for Type A injuries (60%) and Roux-en-Y Hepaticojejunostomy (RYHJ) for Types E1 and E2.
Conclusion: ERCP is a valuable method for diagnosing and managing Bile Duct Injuries (BDIs). The predominant type of BDIs, specifically Type A, is typically diagnosed after surgery. ERCP demonstrates its efficacy in addressing the majority of Strasberg Type A BDIs. In substantial and intricate BDIs, the Roux-en-Y Hepaticojejunostomy is a secure and efficient approach.
Laparoscopic cholecystectomy (LC), a minimally invasive surgical procedure for gallbladder removal, has significantly transformed the surgical landscape due to its associated benefits, such as reduced recovery times and smaller incisions [1]. LC has become the gold standard for treating symptomatic gallstones, presenting advantages over traditional open cholecystectomy, including decreased pain, shorter hospital stays, and faster recovery [2]. Despite its widespread use and generally high success rates, LC is not without potential complications, with bile duct injury (BDI) being one of the most severe [3]. BDI during LC is a rare but potentially devastating complication that can result in substantial morbidity and mortality [4]. The reported incidence of BDI varies widely, ranging from 0.2perecentage to 2.0perecentage, with an overall rate of approximately 0.4perecentage, influenced by differences in surgical technique, patient characteristics, and the definition of BDI [5,6]. Recent studies indicate an incidence of BDIs during cholecystectomy ranging from 0.4perecentage to 0.9perecentage [7,8]. While the rate of BDIs may have been considered low before the LC era (0.1perecentage to 0.2perecentage) [9,10], cholecystectomy's widespread prevalence makes BDIs an essential and potentially life-threatening complication [11]. Consequences of BDI include severe complications like bile leakage, sepsis, cholangitis, liver abscess, and even death [12]. Although most cholecystectomies are now performed laparoscopically, some complex cases still necessitate open cholecystectomy (OC) [13]. LC is the preferred method for uncomplicated gallstone disease and early acute cholecystitis. BDIs are classified based on severity, ranging from minor to primary, and around 20perecentage of BDIs are overlooked during cholecystectomy [14,15]. Neglected BDIs may lead to severe postoperative complications, including fluid collection, biliary peritonitis, sepsis, hepatic or multiple organ failure, and death. Management of BDI depends on its severity and may involve endoscopic or surgical repair to restore bile flow and prevent further complications [16]. The risk of BDI is influenced by factors such as the surgeon's experience, patient anatomy, and the presence of risk factors like inflammation, adhesions, and a small gallbladder [17]. Surgeons with extensive LC experience exhibit lower BDI rates than their less experienced counterparts [18]. Recognizing and preventing BDI during LC is crucial [19]. The use of intraoperative cholangiography, involving contrast agent injection into bile ducts for anatomical visualization, has been shown to reduce BDI risk [20]. Meticulous dissection and careful bile duct handling are essential to minimize injury risk. Despite advances, BDI remains a potential LC complication, emphasizing the importance of surgeon awareness and appropriate measures to prevent and manage BDI, ensuring patient safety and well-being. This study aims to present and analyze a single-centre experience regarding the management of these bile duct injuries in LC.
This retrospective was conducted at the Department of Surgery within Prime Hospital, UAE primarily. Over ten years, from 2014 to 2024, a comprehensive examination was conducted on 2400 Laparoscopic Cholecystectomy surgeries. Throughout the study duration, 18 patients experienced Bile Duct Injuries (BDIs) because of Laparoscopic Cholecystectomy. All 18 patients were diagnosed using ERCP. Out of 18 patients, 13 were treated by ERCP and 5 patients needed further surgery. The relevant data was retrospectively gathered from hospital records, and ethical approval was obtained from the institution's ethics committee.
Diagnostic Approaches:
To identify bile duct injuries (BDI), we employed a comprehensive set of four diagnostic techniques. Intraoperative diagnosis relied on detecting bile leakage from tubular structures, and confirmation was obtained through intraoperative cholangiography. Postoperative diagnosis involved a series of assessments, including complete blood count, C-reactive protein (CRP), bilirubin levels, aspartate transaminase (AST), alanine transaminase (ALT), abdominal ultrasonography, and Multislice Computed Tomography (MSCT) scans. When a definitive BDI diagnosis was not established, Magnetic Resonance Cholangiopancreatography (MRCP) was conducted. If MRCP was unavailable, Percutaneous Transhepatic Cholangiography (PTC) was an alternative for evaluating biliary obstruction. When both MSCT and MRCP results were inconclusive for detecting bile leaks, Endoscopic Retrograde Cholangiopancreatography (ERCP) was employed. The identified types of BDI were then classified according to the Strasberg classification [21].
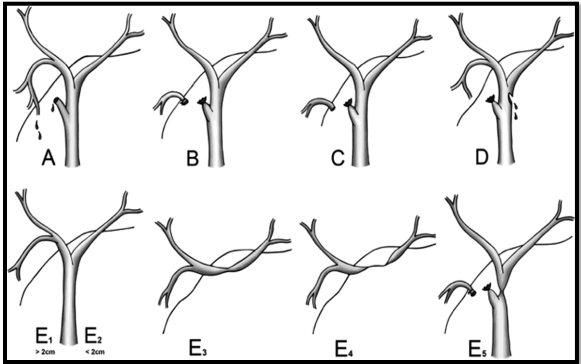
Figure 1: Strasberg classification of bile duct injury [22].
Treatment Approach:
In cases where bile duct injuries (BDIs) are identified during surgery, the approach involves suturing the injury either with or without choledochotomy. Postoperatively diagnosed BDIs are addressed through endoscopic retrograde cholangiopancreatography (ERCP) and stent placement, particularly for minor leaks without peritonitis. If ERCP proves ineffective and the bile leakage is well-drained, conservative treatment is pursued. For Strasberg A injuries, percutaneous drainage is employed. In Strasberg E (E2 and E3), injuries lead to Roux-en-Y hepaticojejunostomy (RYHJ). Incomplete stenosis of the CBD and common hepatic ducts is addressed through ERCP with stent placement or percutaneous transhepatic biliary stenting.
The data were organized and visually represented in appropriate tables and graphs based on their relationships. Detailed descriptions for clear comprehension accompanied each table and graph. Statistical analysis was conducted utilizing the Statistical Package for the Social Sciences (SPSS) program on a Windows platform. Mean values with standard deviations were used to express continuous parameters, while categorical parameters were presented as frequencies and percentages.
The demographic composition of our study cohort revealed a predominant presence of individuals aged 51-70 years, constituting 66.67% of the population. This age group exhibited a higher susceptibility to Bile Duct Injury during Laparoscopic Cholecystectomy. The average age of the participants was 55.21±12.54 years (Table 1). The majority of the study population was male (55.56%), while females accounted for 44.44% (Figure 2). Among the 18 patients diagnosed with Endoscopic Retrograde Cholangiopancreatography (ERCP), only five instances of Bile Duct Injury (BDI) were identified. Three BDIs were diagnosed intraoperatively, while the remaining two were identified postoperatively. Notably, two patients presented with clinical symptoms such as abdominal pain, jaundice, and fever, but their BDIs were not detected during the initial surgery. These two were diagnosed by Percutaneous Transhepatic Cholangiography (PTC) postoperatively. Applying the Strasberg classification, Type A injuries comprised 60% of the cases, with Types E1 and E2 constituting each 20% (Table 2). Table 3 presents a comprehensive summary of the treatment modalities corresponding to Bile Duct Injuries (BDIs) types. For Type A injuries, Endoscopic Retrograde Cholangiopancreatography (ERCP) served as the exclusive treatment method, accounting for 60% of the cases. Meanwhile, Roux-en-Y Hepaticojejunostomy (RYHJ) was employed to address Type E1 and E2 injuries.
Cholecystectomy stands out as one of the most frequently performed abdominal surgical procedures. Laparoscopic Cholecystectomy (LC) is recognized as the preferred method for surgically managing gallstone disease, often referred to as the "gold standard." LC is associated with benefits such as reduced postoperative pain, improved cosmetic outcomes, shorter hospital stays, and less work-related disability than open cholecystectomy [23,24]. In such cases robust training of surgeons in Gastrointestinal and Hepatobiliary procedures, particularly Laparoscopic Cholecystectomy (LC) surgery, involves comprehensive hands-on experience, simulation-based training, and mentorship must be needed. Over the past two decades, LC has gained popularity in the United Arab Emirates (UAE) as a preferred intervention for addressing symptomatic and complex gallstone disease. In cases of symptomatic gallstones, LC is the primary choice. For gallstone-induced cholecystitis, the decision between LC and a two-stage surgical approach (involving percutaneous transhepatic gallbladder drainage in the first stage followed by LC in the second stage) is made based on the patient's condition, following the guidance of the 2018 Tokyo guidelines [25]. Establishing early thresholds for converting laparoscopic to open surgery in complex cases of laparoscopic cholecystectomy is imperative for ensuring optimal patient outcomes. Surgeons must recognize challenging situations and be prepared to make timely decisions, prioritizing safety over the continuation of minimally invasive procedures. Hospitals must prioritize comprehensive readiness for intricate surgeries. Cutting-edge technology, advanced surgical instruments, and highly skilled medical teams are imperative. Bile Duct Injury (BDI) emerges as a severe complication of LC, significantly impacting the patient's quality of life [26,27]. Managing BDI depends on factors such as the timing of diagnosis, locally available devices, and the surgeon's expertise. Recent studies indicate a higher likelihood of biliary tract reconstruction procedures in patients aged 40 to 50 [28–30]. In our study, the mean patient age was 55.21±12.54 years, with the majority falling within the 51-70 age range at 66.67%. These results imply an increased vulnerability to BDI in Laparoscopic Cholecystectomy among individuals aged 51-70. The findings further support the notion that older patients are more prone to requiring post-cholecystectomy biliary reconstruction, aligning with earlier research [27,31,32]. The gender distribution in our study showed 55.56% male and 44.44
This study investigates the management of bile duct injuries (BDIs) during laparoscopic cholecystectomy (LC) through a single-center experience. The research reveals a higher susceptibility to BDIs among individuals aged 51-70. Predominantly, the identified BDIs were Strasberg Type A, with effective management demonstrated through endoscopic retrograde cholangiopancreatography (ERCP). For more intricate injuries (Types E1 and E2), the study successfully employed Roux-en-Y hepaticojejunostomy (RYHJ). Accurate diagnostic methods, such as intraoperative cholangiography and postoperative assessments, are emphasized for identifying and classifying BDIs. The study underscores the significance of surgeon experience and skill in preventing and managing BDIs, highlighting the need for continuous training and awareness in LC procedures.
Based on the findings, the study recommends enhancing surgeon training programs, primarily focusing on recognizing and preventing bile duct injuries during laparoscopic cholecystectomy. A well-equipped hospital ensures optimal patient outcomes, instilling confidence in healthcare professionals and the community. Adequate preparation for complex procedures is deemed paramount for delivering quality healthcare services. In instances where expertise is lacking, the study advocates for the referral of patients to specialized centers for complex procedures. Timely transfer is essential to guarantee access to skilled professionals, ultimately enhancing patient outcomes and safety. Furthermore, the study advocates for collaborative efforts between primary and tertiary care facilities to optimize healthcare delivery. This collaborative approach ensures comprehensive and proficient treatment, contributing to an overall improvement in the quality of healthcare services.
No funding sources
None declared
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
