
Case Report | DOI: https://doi.org/10.31579/2690-8808/163
1 Specialist of I and II Degree in Comprehensive General Medicine, Assistant Professor, Faculty of Medical Sciences of Sagua la Grande, Cuba.
2 I Degree Specialist in Internal Medicin. Assistant Professor, Provincial General University Hospital “Mártires del 9 de Abril”, Sagua la Grande, Villa Clara, Cuba
3 Doctor of Pedagogical Sciences, Full Professor, Faculty of Medical Sciences of Sagua la Grande, Villa Clara, Cuba
4 6th Year Student of Medicine, Faculty of Medical Sciences of Sagua la Grande. Villa Clara, Cuba
5 3rd Year Student of Medicine, Faculty of Medical Sciences of Sagua la Grande. Villa Clara, Cuba
6 I Degree Specialist in Imaging. Clinical Surgical Teaching Hospital "Abel Santamaría Cuadrado". Pinar del Rio. Cuba.
*Corresponding Author: Claribel Plain Pazos, Specialist of I and II Degree in Comprehensive General Medicine, Assistant Professor, Faculty of Medical Sciences of Sagua la Grande, Cuba
Citation: Claribel Plain Pazos, Anel Pérez de Alejo Alemán, Carmen Rosa Carmona Pentón, Nubia Blanco Balbeito. et all (2023), Bilateral Pulmonary Thromboembolism in a post-COVID Patient. J, Clinical Case Reports and Studies, 4(2); DOI:10.31579/2690-8808/163
Copyright: © 2023 Claribel Plain Pazos, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 November 2022 | Accepted: 30 December 2022 | Published: 04 February 2023
Keywords: COVID-19; pulmonary thromboembolism; right bundle branch block
Pulmonary thromboembolism (PTE) is a disease that is difficult to diagnose, and is a problem in the global health system. It is one of the complications described in COVID-19. We present a case of a 49-year-old man, with a history of being a smoker who, ten days after having suffered from COVID 19, begins with right hemithorax pain, cough with yellowish expectoration, slight shortness of breath and tiredness on exertion. interpreted as post_COVID pneumonia and antibiotic treatment is indicated. He does not improve and an EKG is performed which shows rapid response atrial fibrillation. An AndioCT is performed with which he is diagnosed with bilateral pulmonary thromboembolism. It evolves towards healing with treatment with Fraxiheparin. Pulmonary thromboembolism is a feared complication of COVID-19, which requires rapid diagnosis to ensure adequate treatment to achieve patient recovery and prevent death.
Pulmonary thromboembolism (PTE) is a disease that is difficult to diagnose, and is a problem in the global health system. It is the third leading cause of cardiovascular death, after coronary heart disease and stroke. It is not a disease that can be reliably excluded without the aid of expensive imaging studies and some laboratory tests.[1,2] In epidemiological studies, annual incidence rates of PE are 39-115 per year. 100,000 inhabitants [3].
After December 2019, with the arrival of the coronavirus and COVID-19, an increase in the disease has been seen. One of the complications described in COVID-19 is pulmonary thromboembolism (PTE). The coronavirus increases the risk of suffering from this disease. The annual reported incidence of venous ET is between 23 and 69 per 10,000 population, with approximately one third of patients with pulmonary thromboembolism and two thirds with deep vein thrombosis (DVT) [4]. In a study by García Lledo et al. to the. In Madred Spain in 2020, an increase in the incidence of PTE was determined during the first months of the COVID-19 pandemic, with a risk up to 4.5 times higher than that of the same period of the previous year [5].
Occasionally, PE is observed in patients whose respiratory symptoms rapidly worsen and fall into acute respiratory syndrome, increasing the risk of death. On the other hand, it is suggested that there is a direct relationship between the risk of PTE and D-dimer values [4]. 15% of sudden unexplained death is caused by pulmonary thromboembolism, the mortality rate from undiagnosed PE can be as high as 30%[2].
There is no isolated test to help us confirm or rule out PE;that is why its diagnosis is based on several pillars: clinical suspicion, analytical data and imaging test [1].
The treatment of choice is anticoagulation [2]. All patients with a diagnosis of acute PE, unless there is a contraindication, should be appropriately and promptly anticoagulated with unfractionated heparin or low molecular weight heparin [1].
Presentation of the case
Male patient, white race, 49 years old with a history of being a smoker who began with a fever of 38.5˚C, dry cough, weakness, general malaise, PCR is performed, which is positive for coronavirus, he is diagnosed with Covid-19 carryingsymptomatic treatment, improving symptoms.Ten days later he began with pain in the right hemithorax, cough with yellowish expectoration, discreet shortness of breath and tiredness on exertion.
Physical examination found nothing relevant.FR 20´
Complementary Exams:
WBC: 14.9X109neutrophils 74,6 %.
D-dimer 80
Electrocardiogram: Normal.sinus rhythm
Chest radiography: Image of inflammatory condensation at the level of the right ilium (Figure 1).
It is interpreted as post-covid pneumonia and antibiotic treatment is indicated.

Figure 1. Chest X Ray: Image of inflammatory condensation at the level of the right ilium
After starting treatment, the cough and expectoration decreased, although it did not completely disappear, he continued with pain in the right hemithorax and in the interscapular region, in addition to dyspnea and tiredness on exertion.
After six days of antibiotic treatment, as symptoms persisted, an electrocardiogram was performed, diagnosing atrial fibrillation with rapid response.FC 150 X´.Echocardiogram with normal systolic function and slight pulmonary hypertension.
AngioCT was decided to perform due to suspicion of PE given the patient's history and the results of the EKG and Echocardiogram, finding partial condensation of the lower segment of the left lower lobe (Figure 2 A) and posterior and lateral of the right lower lobe (Figure 2 B) corresponding to bilateral PET.
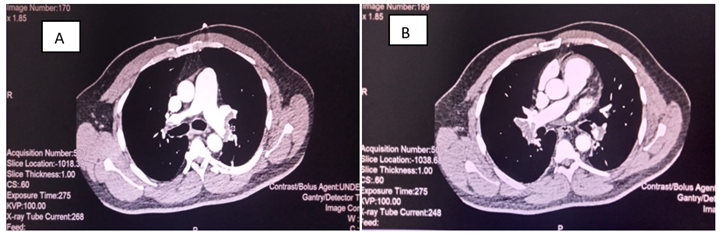
Figure 2: A left PET.B right PET
Anticoagulant treatment with low molecular weight heparin (Fraxiheparin 1mg/kg SC), Digoxin 0.25mg IV daily, Amiodarone 200mg Oral daily was indicated.At 48 hours, the rhythm becomes sinus and the symptoms improve.
The patient presents a satisfactory evolution, completing the scheme with therapeutic anticoagulation with low molecular weight heparin, without dyspnea or chest pain.Medical discharge with outpatient management with oral anticoagulants Oral Warfarin 7 mg daily is considered.The patient is currently being followed up for a symptom-free consultation.
COVID-19 increases the risk of PTE production, which can appear during the course of the disease or after it,[4] as occurred in the present case.
The most frequent symptom is dyspnea, it manifests when the clot obstructs proximal portions of the pulmonary vasculature, it can manifest pleural irritation and pleuritic-type pain in up to 50% of patients, sometimes accompanied by cough and hemoptysis [1]. The patient studied presented dyspnea, pain and cough, but since these symptoms are common for pneumonia and it is a post-COVID patient, who had a chest X-ray suggestive of pneumonia and a negative D-Dimer, it is suspected initially from Post-COVID Pneumonia.
Several bibliographies indicate PE as one of the complications described in COVID-19. The coronavirus increases the risk of suffering from this disease [4]. The non-improvement of the patient's clinical picture despite antibiotic treatment and the appearance of Atrial Fibrillation with rapid response leads to suspicion of the presence of PE.
D-Dimer is the product of fibrin proteolysis in the thrombus. It has a high negative predictive value and as such is used to exclude thromboembolic disease [6]. In this case, initially at the onset of symptoms, the D-Dimer was negative, so this diagnosis was wrongly excluded.
The electrocardiogram in the context of a massive PTE shows a series of pathophysiologically interesting findings, although not very specific from the diagnostic point of view, such as the following in frequency of appearance: 1. Sinus tachycardia 2. T wave inversion 3. Block right bundle branch of His 4. S1Q3T3 pattern [6]. However, other authors report that a finding of unknown atrial fibrillation can lead to suspicion of PE [1], coinciding with what was found in the current case.
Computed tomography angiography, or AngioCT allows the visualization of the thrombus in the pulmonary vasculature through the use of contrast medium, although the fact that the presence of the thrombus cannot be demonstrated does not exclude the disease [4,6]. AngioCT in this patient showed a partial condensation of the lower segment of the left lower lobe and posterior and lateral of the right lower lobe, which allowed the diagnosis of bilateral PE.
The main management of this disease consists of anticoagulation, for which the use of low molecular weight heparins is preferred [1,4,6]. The patient studied was prescribed anticoagulant treatment with low molecular weight heparin (Fraxiheparin 1mg/kg SC), Digoxin 0.25mg IV daily, Amiodarone 200mg Oral daily, achieving recovery.
Pulmonary thromboembolism is a feared complication of COVID-19, which requires rapid diagnosis to ensure adequate treatment to achieve patient recovery and prevent death.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
