
case report | DOI: https://doi.org/10.31579/2690-4861/451
Department of Fundus Disease, Nanning Aier Eye Hospital, Nanning City, China.
*Corresponding Author: Li Li, Department of Fundus Disease, Nanning Aier Eye Hospital, No. 63 ChaoYang Road, Xingning District, Nanning 530012, China.
Citation: Xuemei Liang, Hongmei An, Dongmei Ding, Li Li, (2024), Bilateral Persistent Serous Macular Detachment as Initial Presentation of Waldenström’s macroglobulinemia: case report, International Journal of Clinical Case Reports and Reviews, 19(4); DOI:10.31579/2690-4861/451
Copyright: © 2024, Li Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 April 2024 | Accepted: 05 August 2024 | Published: 15 November 2024
Keywords: waldenstöm’s macroglobulinemia; hyperviscosity retinopathy; serous macular detachmen; silent fluorescein angiography
Background/Purpose: To report a case of bilateral persistent serous macular detachments and vision loss as the first presentation, which turned out to be a malignant lymphoproliferative disorder.
Methods: A case report of a 59-year-old man female patient with vision loss as initial presentations of Waldenstrom macroglobulinemia (WM).
Results: A patient with presented with bilateral persistent serous retinal detachments before diagnosis with WM). The abnormal elevation of serum IgM in the initial stages of her disease course, leading to dramatic ocular findings and images on optical coherence tomography. Even though a session of adequate plasmapheresis and chemotherapy did not reverse the macular detachment, and his visual acuity became worsened because the persists serous retinal detachments leading to a poor visual prognosis.
Conclusion: Our case highlights the importance of maintaining awareness of uncommon initial presentations of WM, which can minimize delay in diagnosis.
Waldenström macroglobulinemia (WM), a rare and incurable lymphoproliferative malignancy, is the result of a clonal B proliferation in the marrow, which casues monoclonal immunoglobulin M (IgM) overproduction in serum.1 Excessive IgM in the peripheral blood may result in hyperviscosity syndrome (HVS). At the time of diagnosis, 30% to 67% of WM patients were found to have HVS-related retinopathy. [2, 3] However, very rarely WM patient presented with bilateral visual complaints as an initial presenting symptom in the setting of undiagnosed WM. We are aware of only one previous case report of a patient without any previous medical history presenting with bilateral decreased vision and persistent SMD due to WM.4 Moreover, in patients with no prior diagnosed WM, these symptoms may possibly be misdiagnosed as other kinds of retinopathy, such as chronic central serous chorioretinopathy (CSC) and autoimmune retinopathy. Herein, we report a case presenting with bilateral visual impairment and persistent SMD as the first clue to the diagnosis of WM.
A 59-year-old man presented with bilateral decreased vision for 1 month. Visual acuity was 20/40 in the right eye (RE) and 20/80 in the left eye (LE). Scanning laser ophthalmoscopy (SLO) showed bilateral white centered retinal hemorrhages (Figure 1 a and 2 a). Optical coherence tomography (OCT) showed significant schisis-like intraretinal fluid and cystoid space in the RE (Figure 1 c), and a large characteristic serous macular detachment (SMD) associated with intraretinal fluid in the LE (Figure 2 c). Fluorescein angiography (FA) demonstrated retinal blood vessels were dilated and segmented, late FA illustrated numerous remarkable microaneurysms and capillary non-perfusion, but without leakage in the macula (“silent FA”) (Figure 1 b and 2 b). Blood investigations showed anemia of 54 g/L and immunoglobulin M (IgM) markedly elevated >25 g/L. Six months later, bone marrow biopsy showed an extensive proliferation of plasmocyte and later lymph node biopsy confirmed the diagnosis of lymphoplasmacytic lymphoma. His underwent local retinal laser photocoagulation and 5 courses of chemotherapy.
At 14 months follow-up, his general health status deteriorated and his vision decreased to 20/250 in the RE and count finger in the LE. SLO showed bilateral minimal retinal hemorrhages and numerous laser photocoagulation spots (Figure 3 a and c). SD-OCT demonstrated schisis-like intraretinal fluid involved macular fovea in the RE (figure 3 b) and persistent SMD in the LE (figure 3 d).
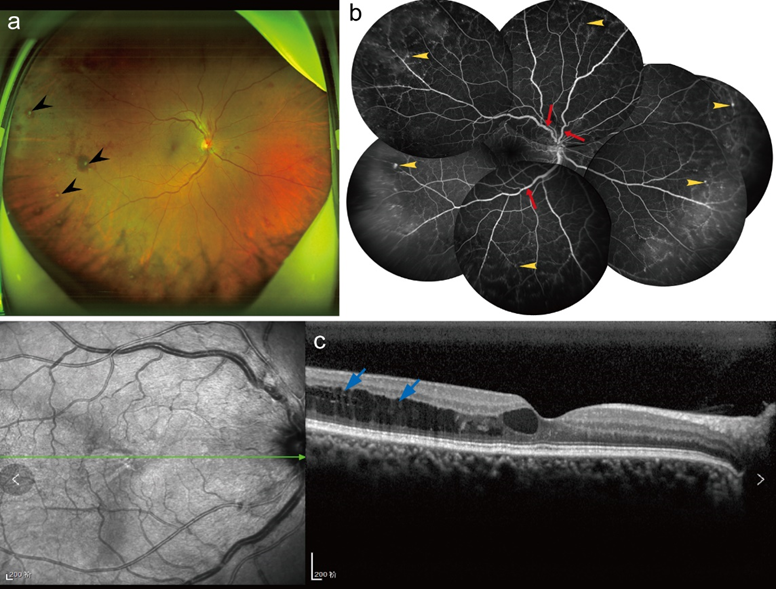
Figure 1. Multimodal imaging of the RE. (a) SLO: White centered retinal hemorrhages (black arrowheads) and retinal venous tortuosity, without macular exudate. (b) FA: venous dilation, segmented, beaded or tortuous with a“sausage link”appearance (red arrowheads), scattered hyper-fluorescent microaneurysms (yellow arrowheads) and peripheral capillary non-perfusion but no macular leakage. (c) SD-OCT: schisis-like significant intraretinal fluid and intraretinal cystoid space in perifovea (blue arrowheads).
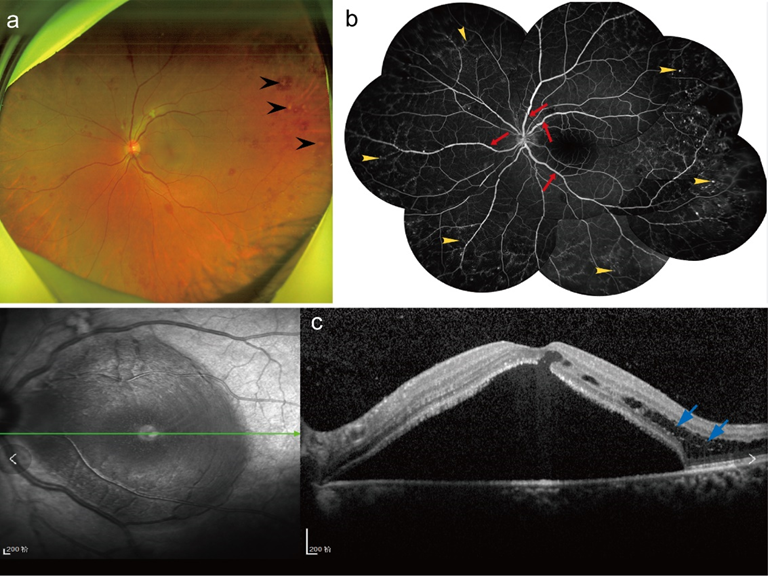
Figure 2. Multimodal imaging of the LE. (a) SLO: White centered retinal hemorrhages (black arrowheads), and macular detachment associated with retinal venous tortuosity. (b) FA: venous dilation, segmented, beaded or tortuous with a“sausage link”appearance (red arrowheads), scattered hyper-fluorescent microaneurysms (yellow arrowheads), peripheral capillary non-perfusion but no leakage in the central macula. (c) SD-OCT: characteristic serous macular detachment and schisis-like intraretinal fluid (blue arrowheads).
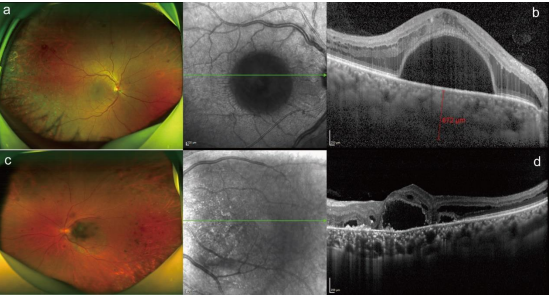
Figure 3: Multimodal imaging of the RE after 14 months. (a) SLO: Numerous retinal punctuate hemorrhages and many laser photocoagulation spots in the temporal periphery (a and c). SD-OCT: schisis-like intraretinal fluid accumulation became aggravated and involved macular fovea in the RE (b). Serous macular detachment, intraretinal fluid, outer retinal atrophy and hyper-reflective material deposits on the internal surface of the retinal pigment epithelium in the LE (blue arrows) (d).
WM is an indolent and chronic progressive lymphoplasmacytic lymphoma characterized by an overproduction of monoclonal IgM1. However, very rarely WM patient presented with bilateral visual complaints as an initial presenting symptom in the setting of undiagnosed WM. Hyperviscosity from accumulation of IgM pentamers resulting in hypoperfusion and vascular stasis that can lead to diffuse intraretinal hemorrhages, retinal exudates, venous sausaging, microaneurysms, serous macular detachment (SMD), even central retinal vein occlusion (CVRO) [5]. The unique and striking finding of serous macular detachment (SMD) with schisis-like intraretinal fluid without dye leakage on angiography (silent FFA) is important to identify as it can be a relevant clinical clue toward identification of WM. OCT showed a significant schisis-like apparence and SMD, unlike other types of serous macular effusion such as CSC and wet age-related macular degeneration (wAMD) that result in SMD, WM-related SMD revealed on evidence of leakage or staining on FFA. Angiographically “silent macula” has become the hallmark of immunogammopathy-induced macular detachments.[6] The pathogenic mechanisms of SMD remains unclear. Many hypothesize that IgM extravasation in the subretinal space results in an osmotic gradient that draws fluid into the subretinal compartment. [7, 8] Furthermore, the chronic toxicity of IgM to the retinal pigment epithelium (RPE) may impede the normal function of RPE for clearing subretinal proteins and fluids. 9 Meanwhile, elevated levels of IgM increased intravenous pressure and gradually reduced retinal blood flow, patients with HVS-related retinopathy will clinically manifest as a status of intravascular stasis, causing venous dilation and tortuosity, retinal exudates and hemorrhages .[3, 10]
Theoretically, HVS-related retinopathy can often be reversed and resulted in improvement of visual dysfunction by timely introduction of chemotherapy and well control of the serum IgM concentration. However, reduction of serum IgM levels and plasma viscosity with systemic therapy has little effect on SMD, On the other hand, traditional treatments for macular edema (i.e. anti-VEGF injections and corticosteroids) may provided no additional benefit. [11, 12] Thus, in order to prevent retinal neovascularization, only retinal laser photocoagulation was performed on the peripheral capillary non-perfusion area of our patient. However, even though a session of adequate plasmapheresis and chemotherapy did not reverse the macular detachment, and his visual acuity became worsened because the persists SMD leading to a poor visual prognosis by permanent RPE and photoreceptor damage. the prognosis for visual function is poor. Li et al. [13] reported similar results that the combination of systemic treatment and intravitreal ranibizumab injection did not have any benefit of visual acuity recovered but even worsened because of increased SMD. Previous studies also reported that persists in most patients even after successful reduction of IgM levels and hyperviscosity with plasmapheresis and chemotherapy. [4, 14]
In conclusion, this 59-year-old man complained of bilateral decreased vision as the first presentation, which turned out to be a malignant lymphoproliferative disorder. The unique and striking finding of SME with schisis-like intraretinal fluid accumulation without dye leakage on angiography (silent FFA) is important to identify as it can be a relevant clinical clue toward identification of WM. Ophthalmologist should be aware of any possibility of underlying malignant diseases when encounter patients with such manifestation. In general, reduction of serum IgM levels and plasma viscosity with systemic therapy has little effect on SMD, and the prognosis for visual function is poor.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
