
Research Article | DOI: https://doi.org/10.31579/2690-4861/253
1 Department of Vascular Surgery, Shahid Beheshti University of Medical Sciences, Shohadaye Tajrish Hospital, Tehran, Iran
2 Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3 Research fellow, Plastic surgery department, Cleveland, OH, USA
4 Master of Architectural Engineering, School of architecture and urban design, Iran University of science and technology, Tehran, Iran
*Corresponding Author: Akbari, Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Citation: SJ Khoshnevis, M Yousefi, M Seraj, F Abbasvandi, P Sadeghi, et. al (2022). Bilateral Commissuroplasty and Primary Repair for Lower Lip Defect (30-80%) After Cancer Excision. International Journal of Clinical Case Reports and Reviews. 12(1); DOI:10.31579/2690-4861/253
Copyright: © 2022 Akbari, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 August 2022 | Accepted: 05 September 2022 | Published: 21 October 2022
Keywords: lip neoplasms; reconstruction; lower lip; primary repair
Introduction: Lip reconstruction is an essential step in lip tumors. In this regard, there are many procedures with good outcomes. Flap problems are the possibility of necrosis and an extensive suture line that wrecks aesthetics. Our technique has no flaps for defects more than 30% of the lip, and the suture line is minimal.
Methods: This study is a surgical technique report from a single center. The original technique was based on our experience with about 100 patients in 25 years. But in this study, 10 patients were included. After excising the tumor, a bilateral 10-15 mm horizontal skin incision beginning from the commissures to lateral sides was made. The skin and mucosa were dissected from the underlying orbicularis muscle, and the muscle was partially cut about 15 mm from each side. Then the remaining sides of the lip were advanced and repaid in three layers. Finally, the released mucosa was sutured to the angle of incised skin.
Results: The patients were followed for at least three years. Oral competence was good, mobility and sensation were well preserved, the scars were less than other flaps, and the aesthetic was satisfying. The patients did not have drooling, flap edema, and pin cushioning.
Conclusion: Among various techniques for lower lip reconstruction, the presented technique in this study seems to be safe and straightforward, but to measure all aspects of it, other surgeons need to use this method and express their opinions.
The lips have essential and diverse function including oral competence, deglutition, articulation, and expression of emotion. The lips are brought together to close the mouth by the role of the orbicularis oris, a complex sphincter muscle [1]. Some of the muscle fibers of the orbicularis oris derive from intrinsic fibers of the lips, whereas others derive from other facial muscles that insert into the lips [2, 3]. Depression and retraction of the lower lip are mainly controlled by the platysma, depressor labii inferioris, and depressor anguli oris muscles. The primary motor nerves of the lips are the buccal and marginal mandibular rami of the facial nerve. The marginal mandibular supplies the lower lip depressors. Sensory innervation of the lips is via the infraorbital and mental branches of the trigeminal nerve [2] and supplies from superior and inferior labial arteries, with venous drainage to the anterior facial vein [2] lymphatic drainage is through submental and submandibular lymph nodes [2]. Researchers have described many reconstructive techniques to overcome significant defects, such as "cross-flap" developed by Abbé and Estlander [4, 5], using the opposite lip with the various modifications suggested [6, 7], and Karapandzic technique [8]. This technique provides the excellent advantage of preserving the nerves and blood vessels of the flaps and allows an excellent sphincteric function to be maintained [9, 10]. Bernard- Burow's method and other versions [fan-flap procedure] are also useful in cases with more lip loss [11]. The purpose of lip reconstruction is to maintain oral competence, mobility and sensation, and obtain the best aesthetic results. When the size of stoma, becomes less than 50
This study is a surgical technique report from a single center. The original technique was based on our experience with about 100 patients in 25 years. A total of 10 patients who were referred to our hospital from 2105 to 2018 were participate in this study and they were followed up for three years. The original technique was based on our experience with about 100 patients in 25 years. Informed consent was obtained from patients before participation in the study. Lower lip defects occurred in all patients following squamous cell carcinoma excision. The patients were in stage 3 of TNM classification and none of them had positive lymph nodes. No antibiotics were given before surgery.
2.1. Surgical technique
Wide local excision of the lower lip tumors was performed under general anesthesia. Reconstruction was undertaken after the margins were shown to be free of cancer by frozen sections. In this technique, the lower lip defect will primarily be repaired even if the defect was more than 30% of the lip. After excising the tumor, A bilateral 10mm to 15mm horizontal skin incision begins from the commissures to lateral sides (figure 1A). Then the skin and mucosa will be dissected from the underlying orbicularis muscle, and the muscle cut partially about 15 mm on each side (figure 1B). Commonly no vessels needed to be ligated and back cut. Two sides of the lip will be advanced and sutured in three layers separately (figure 1C). Finally, the median of the dissected mucosa in the commissures will be sutured to the angle of incised skin. Then completing mucosa to skin suturing (figure 1C).
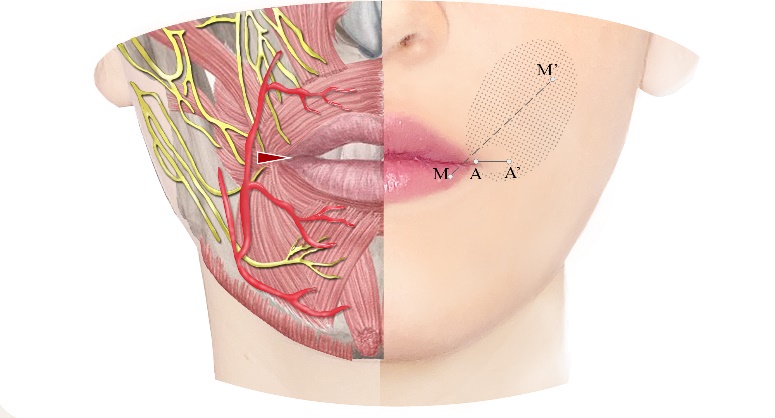
Figure (a)
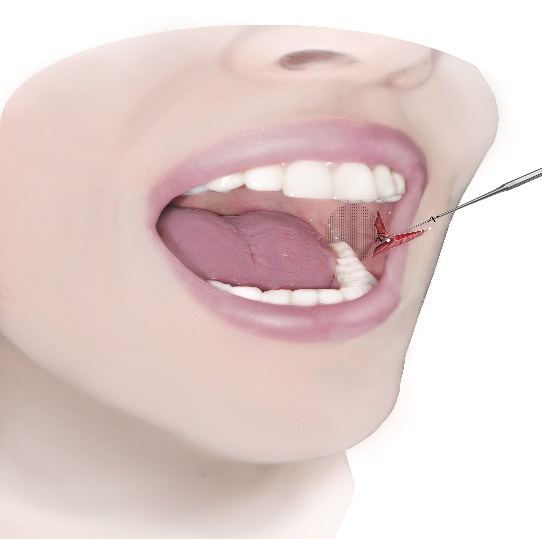
Figure (b)
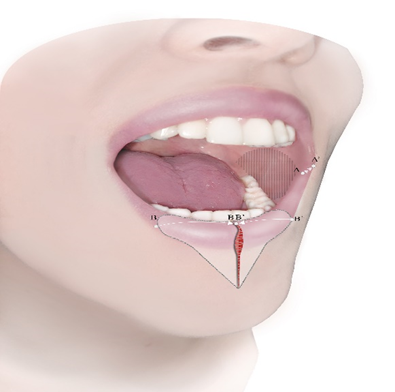
Figure (c)
Figure 1. Surgery steps. All the incisions were bilaterally, but we made the incisions on one side to show inside the mouth in the pictures. A) First, an incision is made from A to A1. Then, an M to M1 incision will be made in the mouth. B) The muscle has been excised from the skin and mucosa and then back cut. C) Two sides of the lip will be approximated and sutured in three layers separately. The median of the dissected mucosa in the commissures sutured to the angle of incised skin from A to A1.
The technique used in this study has a history of 25 years' experience and almost as not had any complications in these few years. Since our data during those 25 years is not complete, we have conducted the study on 10 patients. The patients included 2 female and 8 males with the mean age of 61 years old. The defect size was all above 50% except one case. Five patients had hypertension and 5 had diabetes mellitus (Table 1). The average operation time was about 70 minutes. Sutures were drawn between 5 and 7 days. Early and late postoperative results were satisfactory. No second surgery for modification was needed. At a 3-year follow-up, the patients were doing well with excellent functional and aesthetic outcomes and there was no recurrence. Lip apertures and movements were normal, with sufficient mouth opening and oral competence and good volume and quality of the vermillion. The patients have no complaint of drooling. Speech and sensation were preserved, and highly pleased with the outcome. Figure 2 shows a case in pre-surgical and post-surgical (figure 2).
| cases | age | sex | Etiology | Defect size | Follow up period | HTN | DM | Complication | Recurrence after 3 years |
| 1 | 48 | M | SCC | 50% | 36 months | - | - | None | None |
| 2 | 52 | F | SCC | 65% | 36 months | - | - | None | None |
| 3 | 50 | F | SCC | 70% | 24 months | - | + | None | None |
| 4 | 68 | M | SCC | 60% | 36 months | + | + | None | None |
| 5 | 62 | M | SCC | 70% | 36 months | + | - | None | None |
| 6 | 65 | M | SCC | 80% | 36 months | + | + | None | None |
| 7 | 71 | M | SCC | 40% | 36 months | + | - | None | None |
| 8 | 75 | M | SCC | 55% | 36 months | + | + | None | None |
| 9 | 60 | M | SCC | 65% | 36 months | - | + | None | None |
| 10 | 58 | M | SCC | 70% | 36 months | - | - | None | None |
F: female, M: male, SCC: squamous cell carcinoma, HTN: hypertension, DM: diabetes mellitus
Table 1: demographic data of the patients

Figure 2: Case 6. A) before surgery. B) in operation, the tumor is resected. C) Early post-operation. D) Post-operation year 2. E) Post-operation year 3.
There are many surgical techniques for the reconstruction of the lower lip. The results of the traditional methods have been adequate and sometimes excellent, especially in elderly patients with thin lips. However, the patients, especially young patients, have suboptimal aesthetic problems. For defects less than 30%, a primary repair is an acceptable option, and it's not challenging. For defects of more than 30% of the lower lip, which is the most challenging between surgeons, several flaps are proposed: the Abbe flap [15], the neurovascular Karapandzic flap [8], and Bernard-Webster flap [16]. For more significant defects, not including the angles of the mouth, Gillies's fan is a good choice [17]. One of the choices for Defects involving the commissure is the Estlander flap [5]. All of them have advantages and disadvantages. In the case of local flaps, flap loss, blunting of the repaired commissure, lip asymmetry, sensory loss, hypersensitivity, edema, microstomia, poor oral competence with drooling, undesirable scarring, and flap necrosis must be considered. The Karapandzic flap has the potential risk of microstomia and blunting of the oral commissure [18]. With Karapandzic flap, we have to maintain lip mobility with preserved sensation and competence, but reconstruction of significant defects inevitably results in microstomia, necessitating secondary commissuroplasty [19]. The Webster-Bernard procedure using cheek advancement flaps can give an appropriate lip reconstruction but involves a sizeable perioral tissue loss. Also, it has significant perioral scarring with contour deformity [20]. In addition, effacement of gingivo-buccal sulcus and notching of the central lip have been described as common aesthetic disadvantages [21]. In the Estlander flap, rotation of a lateral area of the upper lip to the commissure is done first, and a second surgery is necessary to reconstruct the commissure angle. Therefore, it needs two operations. The Gillies fan flap has enough tissue to repair with no tension, but the commissure is distorted and becomes blunted, and the lower lip gets short [22]. Also, it has a long suture line, distorting the cosmesis. Analysis for aesthetic results was based on those with pre-and postoperative photographs. Oral competence was measured by muscular integrity and aperture. The orbicularis muscle was partially cut and correctly functioned, and the muscular integrity was preserved. . The aperture and mobility were patient-reporting and asked by dentures and eating problem when eating by spoons or big morsels No drooling was reported, and the severity of drooling was measured by the Blasco index [23]. Fortunately, none of the above problems were reported by patients. And over all the oral competence was good.
Among various techniques for lower lip reconstruction, this technique seems to be safe and straightforward, but to measure all aspects of it, other surgeons need to use this method and express their opinions.
This work was carried out in collaboration between all authors, and all authors read and approved the final manuscript.
Authors have declared that no conflict of interests exists.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
