
Case Report | DOI: https://doi.org/10.31579/2768-0487/072
Critical Care Unit, Kafr El-Bateekh Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
*Corresponding Author: Yasser Mohammed Hassanain Elsayed, Critical Care Unit, Kafr El-Bateekh Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
Citation: Yasser Mohammed Hassanain Elsayed. (2022) Bifascicular Block with Electrocardiographic Sisiisiii Pattern in Mild Covid-19 Pneumonia with Slight Pleural Effusion; Differentiation versus Outcome. Journal of Clinical and Laboratory Research. 5(3); DOI:10.31579/2768-0487/072
Copyright: © 2022 Yasser Mohammed Hassanain Elsayed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 January 2022 | Accepted: 29 January 2022 | Published: 25 February 2022
Keywords: COVID-19 pneumonia; bifascicular block; SISIISIII pattern; left anterior fascicular block; pleural effusion
Rationale: Cardiovascular and chest involvement in a pandemic COVID-19 virus infection may be vital.Bifascicular heart block is affecting the conduction delay or block below the AVN in two of the three fascicles. There is a correlation between mortality with sudden cardiac death (SCD) and bifascicular block. SISIISIII pattern is meaning that the S-waves of amplitude is more than 1.5 mm in I, II, and III. It is a variable prognostic electrocardiographic finding.
Patient concerns: A 67-year-old, retired officer, smoker, married, Egyptian male patient was admitted to the intensive care unit with right bundle branch block, left anterior fascicular block, and mild COVID-19 pneumonia with slight pleural effusion.
Diagnosis: Bifascicular block with ECG SISIISIII pattern in mild COVID-19 pneumonia with slight pleural effusion.
Interventions: Electrocardiography, oxygenation, non-contrast chest CT, and echocardiography.
Outcomes: Good response and better outcomes despite the presence of several remarkable risk factors were the results.
Lessons: Associated hypoxia in the current COVID-19 pneumonia may play an essential role in the present new bifascicular heart block. SISIISIII pattern represents a variable prognostic ECG finding such as RVH, pulmonary embolism, and congenital heart disease. The presence of left ventricular septal hypertrophy is considered another risk. The presence of the elderly male sex, heavy smoker, COVID-19 pneumonia, pleural effusion, bifascicular heart block, SISIISIII pattern, and interventricular septal hypertrophy are prognostic factors for the severity of the disease.
Incomplete trifascicular block and Mobitz type II atrioventricular block were reported in the case of COVID-19. Bifascicular block is affecting the conduction delay or block below the AVN in two of the three fascicles [2]. Conduction to the ventricles will be thorough the single remaining fascicle [3]. The ECG will show typical features of the right bundle branch block (RBBB) plus either left (LAD) or right axis deviation (RAD). RBBB in association with a left anterior fascicular block (LAFB) is the most frequent of the two types. This is due to a single coronary artery blood supply (LAD) to the anterior fascicle. RBBB in association with a left posterior fascicular block (LPFB) is less common due to a dual blood supply (right and left circumflex arteries). The above association may be accompanied by more extensive underlying cardiac pathology [3]. It is usually associated with structural heart disease (SHD) in about 50-80 Percentage. But it may present with extensive fibrosis of the conducting system. So, progresses risk to be complete heart block (CHB if there are additional damage to the third remaining fascicle (1-4 Percentage per year). The patients may be asymptomatic. Syncope occurs in a 17 Percentage of annual risk of progression [2]. The presence of syncope or presyncope in the situation of a bifascicular block is a mark for hospitalization. Structural heart disease (SHD) such as ischemic heart disease (40-60 Percentage cases), aortic stenosis, anterior MI (5-7 Percentage of acute AMI), Lenègre-Lev disease, congenital heart disease, and hyperkalemia are common causes of bifascicular heart block [3]. A new-onset bifascicular block in the condition of chest pain is highly associated with proximal LAD occlusion [3]. There is a correlation between mortality with sudden cardiac death (SCD) and chronic bifascicular block [4]. The association of SCD with coronary disease and ventricular dysrhythmia suggested ventricular fibrillation (VF) as a suggested mechanism [4]. But, if idiopathic syncope after work-up, the pacing is recommended [2]. Cardiac affection in COVID-19 virus infection, as if primarily occurred by the virus or its clinical complications, or its medications cannot be ignored [1]. An incidence of pleural effusions is uncommon in COVID-19 [8]. SISIISIII pattern is meaning that the S-waves of amplitude is more than 1.5 mm in I, II, and III. It is one of the traditional findings which is associated with pulmonary embolism [5]. A SIRIIRIII pattern and SIRIIRIII pattern with a QRS-complex less than 0.12 seconds can be produced by right ventricular hypertrophy (RVH) or zonal right ventricular block [6]. about 90% of SISIISIII pattern cases are associated with congenital cardiac defects which were generally associated with manifestations of RVH and RV hypertension. The pattern is most frequent in children with complete transposition of the great vessels (TGA), associated interventricular communications, and in children having VSD with pulmonary hypertension [7]. Pleural effusion is considered an indicator for severe inflammatory state and carries poor clinical outcomes, and might be an integral risk factor in critical COVID-19 infection [9].
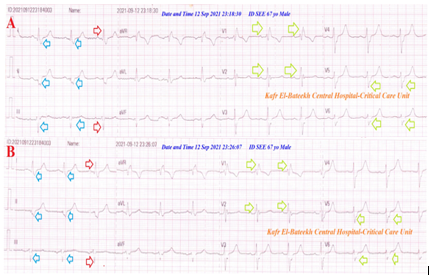
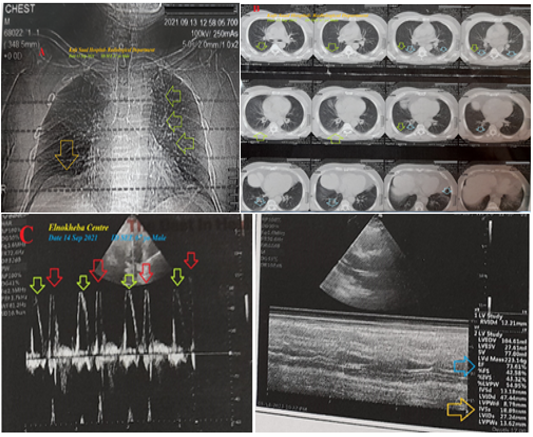
A 67-year-old, retired officer, smoker, married, Egyptian male patient was presented to the emergency department (ED) with dizziness, palpitations, and acute confusion state. He gave a recent history of fever, fatigue, dry cough, generalized body aches, anorexia, and loss of smell 3 days ago. There is a recent contact with a confirmed case of COVID-19 pneumonia. He gives a history of chronic hypertension on captopril (5mg; OD). He is smoking about 20 cigarettes for 28 years. The patient denied a history of other cardiovascular diseases, drugs, or other special habits. Informed consent was taken. Upon general physical examination; generally, the patient was anxious, distressed, with a regular pulse rate of VR; 74 bpm, blood pressure (BP) of 150/90 mmHg, respiratory rate of 23 bpm, the temperature of 37.7 °C, and pulse oximeter of oxygen (O2) saturation of 89%. Currently, the patient was admitted to the critical care unit with right bundle branch block (RBBB), left anterior fascicular block (LAFB), and mild COVID-19 pneumonia with slight pleural effusion. Initially, the patient was treated with O2 inhalation by O2 cylinder (100%, by nasal cannula, 5L/min). The patient was maintained treated with cefotaxime; (1000 mg IV every 8hours), azithromycin (500 mg PO single daily dose), oseltamivir (75 mg PO twice daily only for 5 days), and paracetamol (500 mg IV every 8 hours as needed). SC enoxaparin 80 mg twice daily), aspirin tablet (75 mg, once daily), clopidogrel tablet (75 mg, once daily), and hydrocortisone sodium succinate (100 mg IV every 12 hours) were added. The patient was daily monitored for temperature, pulse, blood pressure, and O2 saturation. Serial ECG tracings through the hospital admission stay were done. The initial ECG tracing was done on the ICU admission of VR; 74 showed NSR with RBBB, LAFB, and SISIISIII pattern (Figure 1A). The second ECG tracing was done within 8 minutes of the above tracing of VR; 76 showed the same abnormalities (Figure 1B). Laboratory workup was done during the third day of the presentation. The initial complete blood count (CBC); Hb was 14.4 g/dl, RBCs; 5.10*103/mm3, WBCs; 6.19*103/mm3 (Neutrophils; 61.9 %, Lymphocytes: 27.6%, Monocytes; 8.9%, Eosinophils; 1.3% and Basophils 0.3%), Platelets; 184*103/mm3. S. Ferritin was high; 478 ng/ml. D-dimer was high (0.756 ng/ml). CRP was high (41 g/dl). LDH was high (500 U/L). SGPT was normal (21.45 U/L), SGOT was normal (20.72 U/L). Serum albumen was low (2.5 gm/dl). Serum creatinine was normal (0.78 mg/dl) and blood urea was normal (17 mg/dl). RBS was normal (119 mg/dl). Plasma sodium was normal (139mmol/L). Serum potassium was normal (4.4 mmol/L). Ionized calcium was normal (1.3 mmol/L) and total calcium was normal (10.4 mg/dl). The troponin test was negative (0.03 U/L). CK-MB was normal (8 U/L). The initial CXR plain film was done during the second day of the presentation showing mild right pleural effusion and mild left parahilar ground-glass opacities (Figure 2A). The first chest CT without contrast was done during the second day of the presentation showing mild right pleural effusion and mild left perihilar ground-glass opacities (Figure 2B). Echocardiography was done during the third day of the presentation with EF; 73.61 % showed diastolic dysfunction with reversed EA ratio, IVS hypertrophy (18.89 mm), and mitral regurgitation (Figure 2C). Bifascicular block with ECG SISIISIII pattern in mild COVID-19 pneumonia with slight pleural effusion was the most probable diagnosis. The patient was discharged within 3 days of hospital admission nearly, after clinical and workup improvement. The patient was continued on aspirin tablets (75 mg, OD) and captopril tablets (5 mg; OD). Further cardiac and chest follow-up was advised.
• Overview:
• A 67-year-old, retired officer, smoker, married, Egyptian male patient was admitted to the intensive care unit with right bundle branch block, left anterior fascicular block, and mild COVID-19 pneumonia with slight pleural effusion.
• The primary objective for my case study was the presence of a patient who presented with a right bundle branch block, left anterior fascicular block, and mild COVID-19 pneumonia with slight pleural effusion in the ICU.
• The secondary objective for my case study was the question of; how did you manage the case at home?
• There was a history of contact with a confirmed COVID-19 case. The presence of confirmed COVID-19 case, left ground-glass consolidation, and laboratory COVID-19 suspicion on top of clinical COVID-19 presentation will strengthen the COVID-19 diagnosis.
• Interestingly, associated hypoxia in the current COVID-19 pneumonia may play an essential role in the present new bifascicular heart block.
• The dramatic response of the associated symptoms may be strengthening this suggestion.
• There is an existence of SISIISIII pattern with the S-waves of amplitude is more than 1.5 mm in I, II, and III. It represents a variable prognostic ECG finding such as RVH, pulmonary embolism, and congenital heart disease [5-7].
• The presence of left ventricular septal hypertrophy is considered another risk.
• Elderly male sex, heavy smoker, COVID-19 pneumonia, pleural effusion, recurrent ischemic cerebrovascular stroke, renal impairment, ischemic heart disease, hypocalcemia, diabetes, ischemic variant premature ventricular contractions, and QRS-complex fragmentation are risk factors.
• Acute myocardial infarction was the most probable electrocardiographic differential diagnosis for the current case study. Butthere is no ST-segment elevation that characterized AMI involving at least two consecutive leads.
• I can’t compare the current case with similar conditions. There are no similar or known cases with the same management for near comparison.
• The only limitation of the current study was the unavailability of coronary catheterization.
• Associated hypoxia in the current COVID-19 pneumonia may play an essential role in the present new bifascicular heart block.
• SISIISIII pattern represents a variable prognostic ECG finding such as RVH, pulmonary embolism, and congenital heart disease.
• The presence of left ventricular septal hypertrophy is considered another risk.
• The presence of the elderly male sex, heavy smoker, COVID-19 pneumonia, pleural effusion, bifascicular heart block, SISIISIII pattern, and interventricular septal hypertrophy are prognostic factors for the severity of the disease.
• The clinical and electrocardiographic response after using anti-COVID19 measures the signifying its role and suggest the diagnosis of COVID19 infection as a causation.
There are no conflicts of interest.
COVID-19: Coronavirus disease 2019
ECG: Electrocardiogram
ED: Emergency department
ICU: Intensive care unit
LAFB: Left anterior fascicular block
LPFB: Left posterior fascicular block
O2: Oxygen
RBBB: Right bundle branch block
SCD: Sudden cardiac death
SGOT: Serum glutamic-oxaloacetic transaminase
SGPT: Serum glutamic-pyruvic transaminase
SHD: Structural heart disease
VR: Ventricular rate
I wish to thank the team nurses of the critical care unit in Kafr El-Bateekh Central Hospital who make extra-ECG copies for helping me. I want to thank my wife to save time and improving the conditions for supporting me.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
