
Case Report | DOI: https://doi.org/10.31579/2641-0419/387
1Aswan Heart Centre, Aswan, Egypt.
2Cairo university, Kasr Eleiny medical school, Cairo, Egypt.
*Corresponding Author: Eslam Ahmed, Cardiology department – Clinica Candela – Palermo.
Citation: Eslam Ahmed, Tarek Hammouda, Ahmed Nasr, Wessam Ali, Mahmoud Abdel Fatah, et al, (2024), Beyond the usual challenges; a case of incessant papillary muscle VT ablation in an 11.5 kg child, J Clinical Cardiology and Cardiovascular Interventions, 7(4); DOI: 10.31579/2641-0419/387
Copyright: © 2024, Eslam Ahmed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 May 2024 | Accepted: 31 July 2024 | Published: 14 August 2024
Keywords: prevalence; population; cardiovascular risk; SCORE scale
Ablation of papillary muscle ventricular tachycardia (PM-VT) has been associated with unsatisfactory results owing to the complex anatomy & difficulty in maintaining catheter contact and stability. Many more challenges could be faced in pediatrics with small hearts.
Objectives:
To report incessant PM-VT ablation associated with haemodynamic instability in a 2-year-old child.
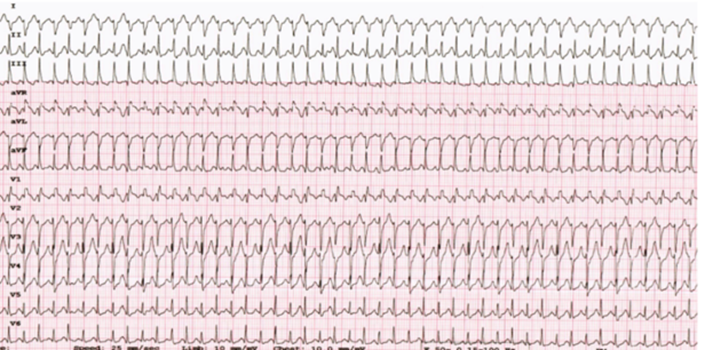
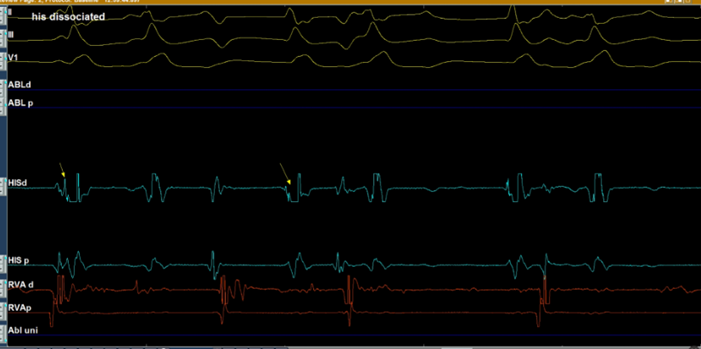
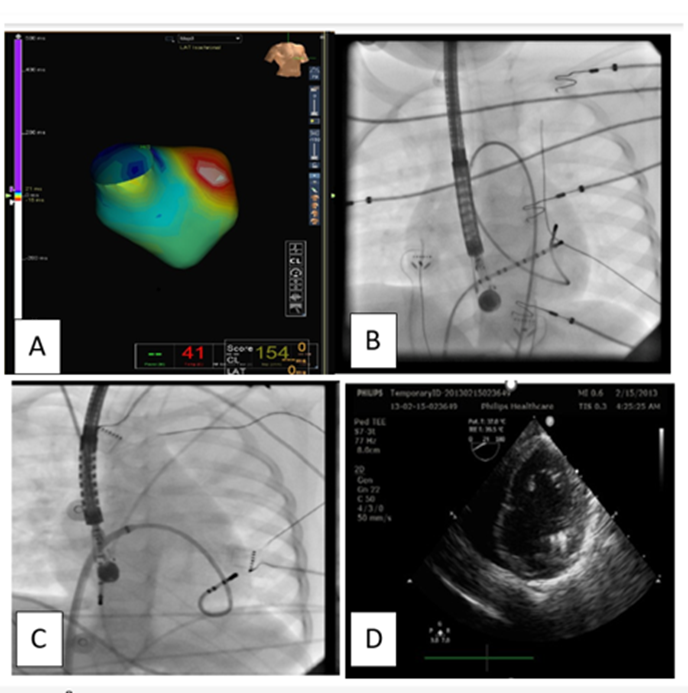
A 20-month-old female patient of 11.5 kg was referred to our centre with incessant tachycardia refractory to medical treatment & cardioversion. On presentation, her blood pressure was maintained on IV supports, Echo revealed fair function. After parents counselling, EP study was done & confirmed the diagnosis of VT. Right femoral artery accommodated hardly a 5F sheath hence, 5F dry tip ablation catheter was used for retrograde LV mapping with the guidance of Navix system. (A, B) An early signal was detected at the anterior PM where the tachycardia was mechanically bumped, RF energy was applied there however, power was limited to 15 Watts due to high temperature, yet the VT wasn’t inducible. 4 hours later, VT recurred So, we decided to go for the antegrade approach via trSSanseptal puncture using an irrigated tip ablation catheter. (C) Moreover, due to unavailability of ICE, TEE was used for better visualization of PM.(D) RF ablation was applied at 35 watts with immediate termination of the VT. Smooth extubation was done with no recurrence of tachycardia. Nevertheless, the patient started to show signs of acute lower limb ischemia for which thrombolytic therapy was initiated with good response. However, one day later, hemoglobin drop and increased abdominal girth were observed. Abdominal CT revealed retroperitoneal hematoma. Conservative management was adopted with regressive course of the hematoma. 5 days later, the patient was discharged home safely. The patient had no arrhythmia recurrence over one year follow up.
Ablation of PM -VT is challenging especially in pediatrics. Access limitation & catheters mobility are the main obstacles, multidisciplinary team collaboration & getting benefits of the available equipments (like TEE) are the keys for success and managing complications in such cases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
