
Case Report | DOI: https://doi.org/10.31579/2690-4861/344
Electrophysiology Department, Favaloro Foundation University Hospital, Buenos Aires, Argentina.
*Corresponding Author: Amrein Eugenia, Electrophysiology Department, Favaloro Foundation University Hospital, Buenos Aires, Argentina.
Citation: Mysuta Mauricio A, Amrein Eugenia, Galizio Nestor O, Carnero Guillermo, Alvarez C Mariel., et al, (2023), Benefit of the Combined use of Three-Dimension Anatomical Mapping and Intracardiac Echocardiography in Catheter Ablation of Premature Ventricular Contraction Coming from the Moderator Band of the Right Ventricle: A Case Report, International Journal of Clinical Case Reports and Reviews, 15(1); DOI:10.31579/2690-4861/344
Copyright: © 2023, Mysuta Mauricio A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 October 2023 | Accepted: 25 October 2023 | Published: 01 November 2023
Keywords: Key words: case report; ventricular arrhythmias; moderator band; intracardiac echocardiography; three-dimension anatomical mapping
Introduction: The moderator band connects the anterior papillary muscle of the tricuspid valve with the free wall of the right ventricle. It is associated with sudden cardiac death risk. Radiofrequency ablation is the treatment of choice for this type of arrhythmias.
Description: An 18-year-old patient with no structural heart disease, 17% of premature ventricular contraction in holter. An ablation using three-dimension electroanatomical system was performed with recurrence after 48 hours. Due to the absence of response to antiarrhythmic drugs a new catheter ablation was performed combining three-dimension electroanatomical system and intracardiac echocardiography. The arrhythmia was interrupted 6 seconds after the start of the application. During follow-up, 48 hours Holter monitoring demonstrated no ventricular arrhythmias at 3, 6, 12, and 18 months.
Conclusion: It is very important to combine the use of three-dimension anatomical mapping system and intracardiac echocardiogram while performing premature ventricular contraction ablation originated in the moderator band in order to obtain better outcomes in this type of arrhythmias, associated with risk of sudden cardiac death.
The septomarginal trabecula, also known as the moderator band (MB) is a myocardial tissue structure that connects the anterior papillary muscle of the tricuspid valve with the free wall of the right ventricle (RV) [1].
This structure usually has two insertions, a septal and a lateral one, which leads to the fact that the arrhythmias originated in them can have two different exits and two different ventricular premature contraction morphologies in the electrocardiogram, one with a superior axis and the other with an inferior axis [2].
There is a direct association between MB and severe ventricular arrhythmias (ventricular tachycardia or ventricular fibrillation) in the absence of structural heart disease. They are often triggered by premature ventricular contraction (PVCs).
Radiofrequency (RF) ablation is the treatment of choice for this type of arrhythmias, due to their risk of sudden death [3]. The use of intracardiac echocardiography (ICE) in combination with three-dimension anatomical mapping allows the identification of the MB and adjacent structures, as well as the correct visualization of the catheter-myocardial contact during the ablation procedure.
We present an 18-year-old patient with no personal or family history of cardiovascular diseases, candidate for the Argentine air force, who presented ventricular arrhythmia in a cardiological control. He referred palpitations associated with dyspnea.
The electrocardiogram (EKG) showed PVCs with inferior axis and left bundle branch block that seemed to come from the lateral region of the RV tricuspid valve. Holter: 17% PVCs, pairs, bigeminy and trigeminy. Echocardiogram: left ventricle of normal size, with preserved ventricular function, normal RV, without valve disease. Cardiac magnetic resonance without late enhancement on T1-T2 sequences.
On August 3rd, 2021, radiofrequency (RF) ablation was performed (three-dimension electroanatomical system - NAVX en SITE - Abbott). PVCs coming front the lateral region of the RV were eliminated. At 48 hours after ablation an EKG showed PVCs with similar morphology (figure 1).
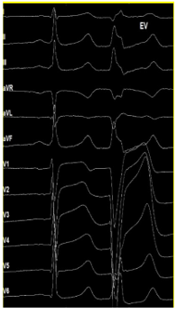
Figure 1: Description: EKG with PVC inferior axis, late transition in precordials (V5), QRS 100ms.
Due to the absence of response to antiarrhythmic drugs a new catheter ablation was performed combining NAVX en SITE - Abbott and ICE.
The following catheters were used: a deflectable quadripolar catheter for coronary sinus recording, an Advisor HD Grid SE for mapping, and a ViewFlex™ Xtra ICE Catheter intracardiac ultrasound.
Reconstruction of the RV anatomy and a map of PVCs prematurity were made (Figure 2A) guided by ICE (Figure 2B), showing an area of greater prematurity (-23ms) (Figure 2C) at the level of the junction of the BM with anterior papillary muscle in the free wall of the RV and a pace-mapping concordance of 97% (Figure 2D).

Figure 2: Description: A: Tridimensional reconstruction of the RV and PVC precocity map in the union between BM, APM and RV free wall. B: ICE: MB insertion from the RV free wall and APM. C: (-) 23 ms precocity to ablation catheter. QS complex in unipolar. D: Stimulation from the ablation cathether with 97% concordance.
RF application was delivered using a TactiCath™ internal irrigated catheter (Abbott) with 35 Watts and a temperature of 42°C. The arrhythmia was interrupted 6 seconds after the start of the application (figure 3). After 30 min and isoproterenol infusion no PVCs were triggered.

Figura 3: Description: A: ICE cathether observing the ablator in the insertion of MB. B: RF aplications with internal irrigated cathether Tacticath (Abbott) in MB.
During follow-up, 48-hour Holter monitoring demonstrated no ventricular arrhythmias at 3, 6, 12, and 18 months.
There is a direct association between PVCs originated from the MB with ventricular tachycardia/ventricular fibrillation, even in asymptomatic patients. Therefore, catheter ablation should be considered as first line therapy.
RF ablation is a challenge for electrophysiologists due to the instability of the catheter and the complex anatomy of the BM. The use of ICE is very important because it allows real-time visualization of MB and guide the tip of the catheter to the proper place in the area of interest.
The combination of ICE, three-dimension anatomical mapping navigators, catheters with high point density to generate voltage and prematurity maps and contact force catheters for ablation, improve the success in this particular PVCs.
It is very important to combine the use of three-dimension anatomical mapping system and ICE while performing PVC ablation originated in the MB in order to obtain better outcomes in this type of arrhythmias that is associated with risk sudden death.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
