
Case Report | DOI: https://doi.org/10.31579/2641-0419/501
Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
*Corresponding Author: Amit Mandal, Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
Citation: Amit Mandal and Oommen George, (2025), Beating the Natural History: A Rare Case of Unrepaired Truncus Arteriosus Type I in a 22-Year-Old, J Clinical Cardiology and Cardiovascular Interventions, 8(12); DOI:10.31579/2641-0419/501
Copyright: © 2025, Amit Mandal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 August 2025 | Accepted: 25 August 2025 | Published: 29 August 2025
Keywords: truncus arteriosus; congenital heart defect; echocardiography
Type I Truncus Arteriosus is a rare congenital heart defect characterized by a single arterial trunk arising from the heart, which causes mixing of oxygen-rich and oxygen-poor blood. Prompt surgical correction is essential to separate the pulmonary and systemic circulations, significantly enhancing patient outcomes. In this report, we present the case of a 22-year-old man who exhibited digital clubbing and cyanosis, along with a history of chronic exertional dyspnoea. He was diagnosed with Type I Truncus Arteriosus. This case offers important insights for healthcare professionals managing similar conditions, emphasizing the critical need for early diagnosis and timely intervention in patients with congenital heart disease (CHD) at risk of progressing to Eisenmenger syndrome. Clinicians should be well-informed and vigilant in identifying the signs and symptoms of pulmonary hypertension, as well as the possible complications that can develop as the disease advances.
Truncus Arteriosus (TA) is a rare congenital heart defect where a single common artery emerges from the heart through one semilunar truncal valve, delivering blood to the systemic, pulmonary, and coronary circulations. The pulmonary arteries branch off from this common arterial trunk, located just beyond the coronary arteries and before the first brachiocephalic branch of the aortic arch.
In this report, we discuss the case of a 22-year-old man who presented with digital clubbing and cyanosis, accompanied by long-standing exertional shortness of breath. He was diagnosed with Type I Truncus Arteriosus and mild pulmonary arterial hypertension (PAH). Additional findings included a right-sided aortic arch, truncal valve regurgitation, mild mitral regurgitation (MR), major aortopulmonary collateral arteries (MAPCAs) supplying both lungs, and anomalous coronary arteries
A 22-year-old male was assessed in the cardiology department after presenting with digital clubbing and cyanosis, accompanied by long-standing exertional shortness of breath. The cyanosis was described as chronic, central, and persistent. The patient had been diagnosed with Eisenmenger syndrome for a prolonged period. Clubbing was clearly visible in all fingers and toes.
Due to a lack of awareness and neglect during childhood, the condition progressed to a stage where surgical correction was no longer feasible. The patient had no history of prior surgeries, and there was no known family history of similar cardiac conditions. At the age of two, a paediatrician suspected a cardiac anomaly; however, the parents did not follow up on the recommendation. By age four, further evaluation confirmed the presence of severe pulmonary hypertension
On examination, he appeared cyanotic, exhibited grade 2 digital clubbing, and had a continuous murmur along the right parasternal border.
The laboratory test results are summarized in Table 1, and the echocardiographic findings are outlined in Table 2 and illustrated in the accompanying figures (Figure 1)
| Test | Result |
| Total WBC Count | 9,600 /µL |
| Hemoglobin (Hb) | 16.4 g/dL |
| Platelet Count | 247,000 /µL |
| Serum Creatinine | 0.82 mg/dL |
| Uric Acid | 6.3 mg/dL |
| TSH | 3.632 µIU/mL |
| Sodium (Na⁺) | 140 mmol/L |
| Potassium (K⁺) | 4.3 mmol/L |
Table 1: Laboratory test results
| Parameter | Findings |
| Situs & Cardiac Position | Situs solitus, Levocardia |
| Diagnosis | Truncus Arteriosus Type I |
| Ventricular Septum | Large conoventricular VSD with bidirectional shunt |
| Truncal Vessel | Common truncus overriding the ventricular septum |
| Truncal Valve | Trileaflet with a large posterior sinus |
| Truncal Valve Regurgitation | Moderate (Pressure Half Time: 362 ms) |
| Main Pulmonary Artery (MPA) | Arising from the posterior sinus of truncal valve; tortuous course |
| Pulmonary Artery Bifurcation | Severe stenosis (possibly membrane/valve-like) proximal to bifurcation |
| Stenosis Gradient | Peak Gradient: 82 mmHg |
| Branch Pulmonary Arteries (PAs) | Continuous flows seen |
| Aortic Arch Anatomy | Right-sided aortic arch |
| MAPCAs | Present |
Table 2: The echocardiography findings

Figure 1: ECHO showing Large conoventricular VSD with bidirectional shunt Common truncus seen overriding the ventricular septum. (White arrow)
He underwent MRI cardiac and that suggested the presence of a common arterial trunk originating from the left ventricle, associated with a large subaortic ventricular septal defect (VSD). (Figure 2) His CT cardiac showed that the common trunk has three cusps, with the left and posterior-facing cusps being enlarged and giving rise to the main pulmonary artery. The main pulmonary artery was notably elongated and tortuous, forming a near semicircular arc before assuming its typical anatomical position to the left of the ascending aorta. (Figure 3)
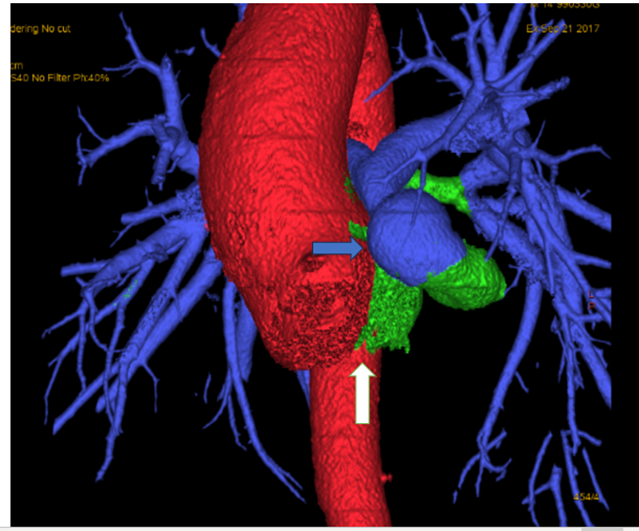
Figure 3: Common trunk (White arrow) which continues as ascending aorta, main pulmonary artery (Blue arrow) which is tortuous and elongated arising from the posterior aspect.
The right coronary artery (RCA) originates from the anterior and slightly left-facing sinus of the common trunk. Shortly after its origin, it gives rise to the infundibular branch and then continues along the atrioventricular groove. At the inferior portion of this groove, it gives off the acute marginal branch, which runs along the free wall of the right ventricle. The posterior descending artery (PDA) also arises from the RCA.
The left anterior descending (LAD) and left circumflex (LCx) arteries originate from the main pulmonary trunk and follow their normal anatomical courses. The LAD exhibits a Type 3 course. (Figure 4)
Truncus Arteriosus (TA), also known as a common arterial trunk or common aortico-pulmonary trunk, represents approximately 0.7% to 1.4% of all congenital heart defects in live-born infants, with an incidence rate of 0.03 to 0.056 per 1,000 live births.(1)
The aortopulmonary septum develops as inward growths within the wall of the truncus arteriosus, shifting position as they move from distal to proximal. This process results in a spiral-shaped septum that separates the truncus arteriosus into two equal vessels: the aorta and the pulmonary trunk. In cases of persistent truncus arteriosus, however, this septum fails to form, allowing both deoxygenated and oxygenated blood to mix and flow through a single common trunk.(2)
The cause of truncus arteriosus is multifactorial and may be linked to conditions such as DiGeorge syndrome, a 22q11.2 deletion, maternal diabetes during pregnancy, and exposure to teratogens like retinoic acid. A non-restrictive ventricular septal defect (VSD) is always present, allowing both ventricles to empty into the common trunk. Cyanosis in truncus arteriosus is generally mild due to the high pulmonary blood flow and pressure. However, without timely treatment, elevated pulmonary vascular resistance (PVR) can develop early, leading to pulmonary hypertension, decreased lung perfusion, and worsening cyanosis.
The Van Praagh classification system categorizes Truncus Arteriosus (TA) based on the origin of the branch pulmonary arteries from the common trunk, the development of the aortic arch, and the presence of a patent ductus arteriosus (PDA).(3)
The index patient was diagnosed with type III truncus arteriosus. Clinical presentation varies depending on the child's age and pulmonary vascular resistance (PVR). In the first month of life, signs of heart failure and cyanosis are generally absent. As PVR decreases, symptoms of heart failure usually appear during the second month. Common findings include a hyperdynamic precordium, cardiomegaly, and a single, loud second heart sound. Infants typically present with symptoms such as tachypnoea, tachycardia, and failure to thrive.
Truncus arteriosus can be assessed using multiple imaging techniques, each highlighting characteristic features of the condition. For example, a chest X-ray may reveal an enlarged cardiothoracic ratio, right-sided aortic arch in about 50% of cases, and signs of pulmonary over circulation. An electrocardiogram often shows evidence of right ventricular hypertrophy. Echocardiography remains the primary diagnostic tool, typically identifying a large truncal artery overriding a ventricular septal defect. Increasingly, computed tomography (CT) is used alongside echocardiography to aid in detailed preoperative planning. (4)While cardiac catheterization was once central to diagnosis, it is now mainly reserved for therapeutic interventions or for evaluating hemodynamic in older patients.(5) It is no longer considered a first-line diagnostic method for newborns with truncus arteriosus.
It is advised that infants with truncus arteriosus begin anti-heart failure treatment within the first week of life. Surgical correction should ideally be performed within the first month, with the Rastelli procedure recommended before three months of age to prevent the onset of pulmonary vascular disease. During the operation, the ventricular septal defect (VSD) is closed, and the pulmonary artery is separated from the truncus. A homograft conduit is then used to establish a connection between the right ventricle and the pulmonary artery. While surgical outcomes are generally very good, the implanted conduits often develop stenosis or regurgitation as the child grows, necessitating future replacement.
Surgery is contraindicated in patients with severe pulmonary arterial hypertension accompanied by irreversible pulmonary vascular occlusive disease. Indicators of inoperability include age over one year, resting systemic oxygen saturation below 85%, and the absence of cardiomegaly. (6)Patients who are borderline operable due to advanced pulmonary vascular disease should be referred to a specialized centre for further assessment. The decision to proceed with surgery should be individualized, considering the patient's medical history, physical examination findings, and results from all relevant investigations.
Current data show perioperative mortality rates between 7% and 11%.(7) Long-term survival has significantly improved over time, with studies reporting 10-year survival rates between 80% and 90%, and a 30-year survival rate of approximately 74%.(8,9)
Patients with truncus arteriosus who do not receive surgical treatment generally have a poor prognosis. However, survival may be prolonged in individuals with associated pulmonary stenosis, as it can limit excessive pulmonary blood flow and reduce the risk of developing pulmonary vascular disease. Although rare, there are isolated reports of long-term survival without surgery, and most of these cases involve the presence of pulmonary stenosis.(10)
Causes of death may include metabolic acidosis, cardiac arrest, arrhythmias, impaired heart function, and failure of multiple organs.
Truncus arteriosus is a complex and life-threatening cyanotic congenital heart defect, with most affected children not surviving beyond their first year without intervention. However, this case illustrates that some patients may live longer, prompting important questions about the factors contributing to extended survival in a small subset compared to the majority. In conclusion, this case report highlights the complex management challenges involved in caring for a 22 year-old male with Eisenmenger syndrome, marked by severe pulmonary hypertension and digital clubbing. Due to the irreversible progression of the disease and lack of surgical treatment options, a conservative approach was implemented. Management focused on continuous monitoring and preventive care, both of which are essential for improving outcomes and reducing the risk of complications.
This case offers meaningful insights for healthcare providers managing similar conditions, emphasizing the critical importance of early diagnosis and timely intervention in patients with congenital heart disease (CHD) who may be at risk of developing Eisenmenger syndrome. Clinicians must be well-prepared to identify the signs and symptoms of pulmonary hypertension and understand the potential complications that can arise.
Looking ahead, future research should focus on developing new treatments to improve quality of life for patients with Eisenmenger syndrome and studying the long-term outcomes of conservative care. Creating multidisciplinary care guidelines and exploring genetic and environmental factors could enhance prevention and management. Ultimately, these efforts may lead to better therapies, improved patient education, and more effective self-care.
Written informed consent was obtained from the patient for the publication of this case report, including all accompanying images and videos.
Not applicable
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
