
Case Report | DOI: https://doi.org/10.31579/2641-0419/117
*Corresponding Author: Damyan B Boychev, Acibadem City Clinic Cardiovascular center, Sofia
Citation: Ivo Petrov, Zoran Stankov, Damyan Boychev, Valentin Balabanski, Marko Klissurski (2021 Basilar Artery Occlusion. Clinical Evaluation and Contemporary Methods of Treatment. J. Clinical Cardiology and Cardiovascular Interventions, 4(1); Doi:10.31579/2641-0419/117
Copyright: © 2021 Damyan B Boychev, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 December 2020 | Accepted: 19 December 2020 | Published: 08 January 2021
Keywords: posterior circulation stroke; basilar artery occlusion; intravenous thrombolysis; endovascular treatment
Acute occlusion of the basilar artery and its branches is a frequent cause of posterior circulation strokes. Although it accounts for only 1 to 3 % of ischemic strokes, it is a potentially life-threatening condition associated with high mortality rates. Exact clinical diagnosis is still challenging because symptoms such as vertigo, dizziness followed by headache, and neck pain are nonspecific and usually attributed to many other neurological diseases. The onset of symptoms can be abrupt or gradual and progressive. Establishing the time of symptoms onset and making a timely diagnosis is highly important. In case the diagnosis is made promptly, ideally with the help of an advanced neuroimaging, intravenous thrombolysis, or catheter-based endovascular treatment can be performed immediately to improve prognosis and reduce mortality.
Basilar artery occlusion – BAO
Posterior circulation ischemia – PCI
Intra-arterial thrombolysis – IAT
Intravenous thrombolysis - IVT
Basilar artery – BA
Posterior Circulation – PC
Anterior Circulation – AC
Vertebrobasilar ischemia – VBI
Modified ranking score – mRS
Mechanical thrombectomy - MT
Basilar artery occlusion (BAO) accounts for about 1 to 3-4% of all ischemic strokes. [1] BAO is one of the scenarios of posterior circulation ischemia (PCI), and it is associated with high mortality if left untreated. [2-4] BAO symptoms could be non-focal and unspecific, such as headache, dizziness, and vertigo, resulting in a delay in the neurological evaluation. [5-7] Timely made diagnosis and treatment are some of the most difficult tasks. Intravenous thrombolysis (IVT) is still considered standard of treatment when performed within 3 to 4.5 hours after the onset of symptoms. [8] Although novel studies show better results when intra-arterial thrombolysis (IAT) or mechanical thrombectomy (MT) is performed. Early studies of endovascular treatment showed that it is associated with high rates of recanalization success, a better outcome for the patient, and a reduction in mortality rates. [1, 9]
One of the most important arteries of the human body is the basilar artery (BA). [10] It is formed by the convergence of the left and right vertebral arteries at the junction of the pons and medulla. It runs along the basilar sulcus of pons and branches out into numerous ramifications which include the following: anterior inferior cerebellar artery, pontine arteries, labyrinthine artery, superior cerebellar artery, and posterior cerebral arteries. The vertebrоbasilar arterial system supplies the posterior portion of the circle of Willis and receives about 20 % of cerebral blood flow. Its main responsibility is to supply the brainstem, thalami, cerebellum, and parts of the occipital and temporal lobes. [11, 12]
Etiology
The most frequent causes of BAO are local thrombosis and artery-to-artery thromboembolism originating from arteriosclerotic lesions. [4]
Atherosclerosis is one of the main reasons for BAO. BA is the intracranial artery most commonly affected by the atherosclerotic process. [12] Usually, it affects the mid-portion of the basilar artery, followed by the vertebrоbasilar junction. Atherosclerotic BA stenosis is the most common cause of BAO in older patients. [15] Occlusion due to atherosclerosis is usually seen in the sixth and seventh decade of life.
Other etiological factors that lead to ВАО are artery-to-artery embolization (most frequent cardiac origin emboli) and vertebral artery dissections, affecting respectively 30-35% and 6-8% of patients. [4] The typical locations of the obstruction with arterioembolic mechanism [4] are the vertebrobasilar junction and the distal third of the BA, especially at the top of this artery. [13] It is most prevalent in the fourth decade of life. [8, 10, 14-16]
Dissections are more often seen in the extracranial vertebral artery and are most commonly associated with neck injuries, yoga practice, and cervical chiropractic adjustment. Although rare, dissection can also be seen in the intracranial segment, most often spontaneous in these cases. Vertebrobasilar dolichoectasia, an anatomic variant consisting of enlargement and extreme dilatation of the vertebral/basilar artery, has been shown also to predispose to BAO through a reduction in flow velocity leading to local thrombus formation. [5, 17] Other rare causes include meningitis, coagulopathy, arteritis, cervical trauma, aneurysms, hereditary arteriopathies, as well as complications after endovascular procedures and neurosurgery. [4] One recently described case of reversible stenosis of the BA is due to hemoconcentration, a condition that is frequently found in psychiatric patients with severe depression. [7]
Pathogenesis of the disturbances of the Posterior Circulation (PC) disease differs from Anterior Circulation (AC) disease in their pathophysiology, clinical presentation, symptoms development, optimal imaging methods, and the available treatments. It is common to divide diseases of PC into two categories. On one hand, acute BAO has a more rapid onset, the diagnosis must be made quickly and the following treatment should not be delayed because of the extremely poor natural course. On the other hand, BAO is characterized by more slowly developing ischemia in the PC leading to non-specific symptoms and early warnings of PC disease that now can be related to ischemic events in all PC vessels. These signs and symptoms occur much earlier than those in the AC [13]. In both scenarios, the treatment of choice has to be the removal of the BA thrombosis or embolus because if left untreated, the clinical evolution is usually extremely unfavorable.
Epidemiology and risk factors
Available data on the frequency, incidence, and prevalence of the BAO is still insufficient. A posterior circulation obstruction is a common form of stroke affecting in total about 1/5 of all patients with stroke [13]. BA thrombosis accounts for about 27% of the ischemic strokes occurring in the posterior circulation. Men are affected twice as much as women. (10) Acute BAO is a rare stroke syndrome comprising only about 3% of all ischemic strokes. [17, 18]
All the risk factors typical for the development of atherosclerosis can be associated with vertebrobasilar ischemia. [19-21] These include arterial hypertension, diabetes mellitus, dyslipidemia, smoking, age, gender, family history, and genetic factors. Furthermore, patients with a history of coronary artery disease or peripheral artery disease are at increased risk. [22] Other etiological causes may include cardioembolic conditions such as atrial fibrillation, infective endocarditis, vertebral artery dissection, and systemic hypercoagulable states [23].
Clinical presentation and diagnosis
BAO requires quick diagnosis and immediate treatment. [12] Dizziness and vertigo are the most common findings in the history of the patient, suggesting vertebrobasilar ischemia. Vertigo, which is the most common symptom, is defined as a sensation of spinning and usually indicates dysfunction of the peripheral vestibular or central vestibulocerebellar system. Dizziness is associated with lightheadedness or lack of mental clarity. Vertigo and dizziness caused by BAO are often connected with other brainstem or cerebellar symptoms. When vertigo is the only symptom it is very important to establish whether its origin is central or peripheral. In this case, the head-impulse, nystagmus, test of skew (HINTS) examination is a useful bedside test to distinguish peripheral from a central lesion. In patients with PCI, headache is a common presenting symptom. [3, 7, 17, 24-27]
Other symptoms include syncope, "drop attacks” (patient feels sudden weakness in the knees and fall on the ground), diplopia or loss of vision, paresthesia, confusion, dysphagia, and dysarthria. [4] If vertebrobasilar ischemia (VBI) advances into a brainstem infarction, several syndromes may arise depending on the location: lateral medullary syndrome, medial medullary syndrome, basilar artery syndrome, and labyrinthine artery syndrome. Other aspects of the history that should be noted during the clinical evaluation are reproducible symptoms during positional head changes. For example, a syncope is possible while turning the head laterally (Bow Hunter’s syndrome) or during head extension. [28-30]
In patients with PCI, headache is not an unusual symptom and it seems to be caused by irritation of the trigeminovascular afferents located in the brainstem. Headache has predominantly occipital localization and may occur two weeks before the stroke. [24]
Depending on the onset of symptoms, three major clinical types of BAO presentation have been described:
a) Sudden onset (without preceding events) of severe motor and bulbar symptoms (ophthalmoplegia, quadriplegia, and anarthria) combined with reduced consciousness [7];
b) Abrupt but with prodromal symptoms such as transient double vision, dysarthria, vertigo, paresthesia, which precede the monophasic BAO symptoms by several days or even weeks or months [21];
c) Progressive clinical presentation characterized by a gradual course of posterior circulation symptoms such as blurred vision, balance disturbance, bilateral paresthesia, or motor weakness, which finally are associated with reduced consciousness. [4, 31]
Some differentials with overlapping symptoms should be considered. These include meningitis, basilar migraine, cerebellar hemorrhage with brainstem compression, cerebellar infarct or hemorrhage with edema, space-occupying lesions in the posterior fossa including metastatic disease, and supratentorial mass lesions with mass effect, herniation, and brainstem compression. [32, 33]
Evaluation
The primary goal of the examination is to establish the localization of vascular lesions and specify if acute intervention is indicated to achieve recanalization in a time-dependent manner. Laboratory studies are of little value but may include a complete blood count (CBC), electrolytes, blood urea nitrogen (BUN), creatinine, international normalized ratio (INR), prothrombin time (PT), and activated partial thromboplastin time (aPTT). Young patients with a low possibility of atherosclerosis should be investigated for hereditary procoagulant conditions. These include protein C, protein S, antithrombin III deficiencies, lupus anticoagulant, and anticardiolipin antibodies, and homocysteine levels. Thorough searching for arrhythmogenic etiology on ECG should be done [10].
Imaging methods for diagnosis
Computed tomography (CT) and magnetic resonance imaging (MRI) are commonly used as a screening imaging technique to evaluate posterior circulation disease. Nowadays, 7T MRI angiography (MRA) represents a new valuable imaging method for the evaluation of PCD. [13] All of Doppler sonography, CT, contrast-enhanced CT angiography (CTA), MRI, MRA can be used in the acute setting to evaluate patients with suspected BAO. [4]
CT is usually the first imaging study performed. Hemorrhagic pathology or a large area of ischemic insult can be diagnosed, but it is less effective as a screening tool for evaluation of brainstem, cerebellum, and posterior circulation. Filling defects within the BA could be seen with CTA. However, CT scanning is less sensitive for the detection of early ischemia or vascular occlusion compared to MRI/MRA.
The gold standard for definitive diagnosis of BAO is still conventional cerebral angiography. It is superior to MRI and CT angiography and is more and more used in the context of catheter-based endovascular IA treatments (mechanical thrombectomy/ thrombaspiration procedures).
Treatment
Treatment of BAO aims to recanalize the occluded artery and salvage the brain tissue. BA recanalization can reduce mortality and increase the patient’s chances of functional recovery through reperfusion therapy. The reperfusion therapy includes IVT, IAT, and mechanical endovascular thrombectomy/thrombaspiration. [34] After the diagnosis of BAO is made, IVT or endovascular treatment can be performed to recanalize the occluded artery depending on the treatment time-window. Despite the lack of large scientific evidence, in the majority of patients with BAO, IAT or IVT has to be performed because if left without any reperfusion treatment the natural prognosis of BAO is extremely poor. The earlier the intervention is performed, the better are the results. [35-39]
The IVT is contraindicated in patients with acute ischemic stroke with the onset of symptoms of more than 4.5 h, in patients with head trauma in the last 3 months before the acute ischemic stroke, in patients with intracranial or subarachnoid hemorrhage, blood pressure ≥185/110 mmHg, or low serum glucose levels ≤2,8 mmol/l. Small case series and trials have shown IAT is a highly prospective intervention in patients with contraindications for IVT because of its higher recanalization rate and lower bleeding risk. [34]
In the management of acute ischemic stroke, IVT still is considered standard strategy. Three large multicenter studies – SITS-MOST, the IST-3 and ECAS III evaluated the safety and efficacy of IVT, with a therapeutic window of 3, 4.5, and 6 hours, respectively. A point should be made that most of the patients in these studies had anterior circulation ischemia because the localization of stroke in posterior circulation is often quoted as an exclusion criterion. [40, 41] According to nowadays American Stroke Association guidelines for the early management of patients with acute ischemic stroke - IV alteplase is recommended for selected patients who can be treated within 3 and 4.5 hours of ischemic stroke symptoms onset or patient last known well. [42]
Some uncontrolled studies, in which IAT was used, showed a high recanalization rate, around 65%. (31) The efficacy of fibrinolytic treatment with IVT or IAT in posterior circulation strokes was evaluated in only one prospective, observational study of patients with BAO-BASICS (The basilar artery interventional cooperation study). [43] In this study, the modified Ranking score (mRS) was used as an endpoint of the comparison in the efficacy between these treatments. In patients with mRS 0-2, with mild to moderate BA stroke, IVT treatment showed better outcomes compared to intra-arterial treatment, 53% to 30%, respectively. When considering patients with severe stroke, with a high mRS score (at least 2 or more), the outcome did not differ significantly. Recanalization occurred in 72 % of patients treated with endovascular procedures compared to 63% of patients treated with IVT and that was associated with increased functional independence. [44]
In a multicenter, randomized study evaluating 131 Chinese patients, both per-protocol and as-treated analysis showed that thrombectomy was superior to the best medical treatment in BAO. [45] In a recently published single-center observational study, a Swedish group reported 73% of successful recanalization with combined catheter-based intra-arterial interventional techniques in patients presenting with BAO. [46]
Our group published a case of successful combined catheter-based treatment (mechanical recanalization, balloon angioplasty with a non-compliant balloon, and low dose intra-arterial fibrinolysis) in a 67-year-old patient with BAO causing tetraplegia and coma. [47] We showed the result of a particular case of successful consecutive contact thrombaspiration of BAO and the two posterior cerebral arteries performed with Penumbra 5 MAX (Penumbra, Inc., USA) thrombaspiration catheter in a patient admitted 2 hours after a sudden onset of dizziness, deep somnolence, and fluctuating blurred speech.
According to the European Stroke Organization, there is consensus among the panel (11/11 votes) that in analogy to anterior circulation large vessel occlusion (LVO) and with regard to the grim natural course of BAO, the therapeutic approach with IVT plus MT should strongly be considered [48].
According to 2018 Guidelines for the Early Management of Patients with Acute Ischemic Stroke: (AHA/ASA): Although the benefits are uncertain, the use of MT with stent retrievers may be reasonable for carefully selected patients with acute ischemic stroke in whom treatment can be initiated (groin puncture) within 6 hours of symptom onset and who have causative occlusion of the anterior cerebral arteries, vertebral arteries, BA, or posterior cerebral arteries - IIb. The use of MT devices other than stent retrievers as first-line devices for MT may be reasonable in some circumstances, but stent retrievers remain the first choice – Iib [42].
Endovascular treatment both with stent retriever and contact aspiration thrombectomy as a first-line approach was safe and effective methods in a multicenter retrospective observational study which included 212 consecutive patients with acute BAO treated with one or the other technique. [49] In the published small trials MT was associated with low rates of mortality (13%), procedure-related complications (4.2%), or symptomatic hemorrhage (1.9%). The application of MT in BAO was associated with high rates of favorable outcomes (44.8%) and high rates of successful reperfusion (91.5%). [49-51]
The treatment window for acute BA thrombosis is not well defined yet. The commonly accepted time window is at least 12 hours potentially up to 24 hours. A well-accepted common opinion is that the treatment window of MT for BAO window has to be much longer than the accepted recommendation for treatment of large vessel occlusion in the anterior circulation stroke - 6 to 8 hours [35-38, 52] probably because of the extremely poor prognosis for patients left without recanalization attempt.
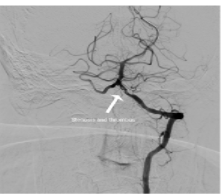
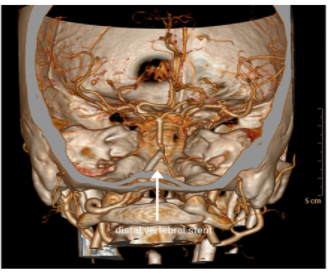
To demonstrate the efficiency of the endovascular treatment of stroke we present a case of a 62-year-old male who was referred to the clinic due to one-week symptoms of left hemiplegia, dysarthria, vertigo, ataxia, and balance problems. Duplex and Doppler ultrasound examination of the neck arteries showed absence of flow in the right vertebral artery, significantly reduced post-stenotic pattern of blood flow in the left V2 segment of the vertebral artery, 70% stenosis of the left internal carotid artery (LICA) and normal flow in the right internal carotid artery (RICA). Angiography confirmed the ultrasound findings (Figure 1): occlusion of the right vertebral artery, subtotal occlusion of the proximal left vertebral artery, 70% stenosis of LICA and patent RICA. Using Fielder XT (Asahi Intecc, Japan) wire for chronic total occlusions, the proximal left vertebral stenosis was passed through. (Figure 2) After pre-dilatation, Resolute Onyx 4.5/22 mm stent (Medtronic. USA) was implanted in the proximal left vertebral artery, V0/1 segment. A second subtotal occlusion at the distal left vertebral artery was revealed in the V4 segment. (Figure 3) It was treated by pre-dilatation followed by implantation of the Resolute Onyx 2.75/22 mm stent (Medtronic, USA). Final angiography showed excellent results and restored TICI-3 flow in the vertebrobasilar system. (Figure 4) Two months were needed for the patient to improve his ataxia and dysarthria, and to recover from hemiplegia. The follow-up CTA showed preserved flow and patent vessels. (Figure 5) The patient had gone back to his normal life.



Methods
Our in-hospital protocol is to evaluate all patients with BAO for endovascular treatment. All the patients with onset of stroke for less than 6h are treated by thrombaspiration and/or IAT. Our primary endovascular treatment method is ADAPT - A Direct Aspiration First Pass Technique. Patients with the onset of stroke for more than 6h but less than 24h are carefully evaluated and treated by the same means as the <6h group if they do not match one of these criteria: bilateral mydriasis, absent brainstem reflexes, hemorrhage on brain imaging, profound coma, limited life-expectancy despite stroke treatment. Patients with BAO older than 24h are evaluated individually and treated by endovascular means only if they fall into the group with progressive symptom presentation or they have enough retrograde circulation from the posterior communicating arteries, visualized on CTA, ensuring the viability of the infarction zone.
Conclusion
The BAO is related to high mortality rates and a severe reduction in the quality of life. With the advancement of pharmacological treatment and endovascular therapy, reduction in mortality and disability rates in these patients can be achieved. There is a gap in the evidence about the best method for the treatment of BAO. New methods have a proven role in the treatment of anterior brain circulation disease, but small patient case series and some systematic protocols showed that endovascular treatments were also safe and effective for BAO, when performed by experienced operators. Modern methods of treatment applied on time are related to a significant reduction of mortality and better prognosis in this otherwise unfavorable group of patients.
Funding
The authors received no funding for this work.
Disclosures
The authors have no disclosures.
Acknowledgements
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
