
Case Report | DOI: https://doi.org/10.31579/2690-4861/197
1 Senior Physiotherapist, the Royal London Hospital, Barts Health NHS Trust, London, United Kingdom.
2 Speech and Language Therapist, the Royal London Hospital, Barts Health NHS Trust, London, United Kingdom.
3 Clinical Specialist Physiotherapist, Critical Care Outreach Team, the Royal London Hospital.
*Corresponding Author: Amanda Thomas, FCSP, Clinical Specialist Physiotherapist, Critical Care Outreach Team, the Royal London Hospital.
Citation: Hussain Z, Adshead B and Thomas A.J. (2022) Barriers to Tracheostomy Weaning: A Case Report of Sialorrhea in a Patient with Persistent Seizure Activity and Head Injury. International Journal of Clinical Case Reports and Reviews. 10(4); DOI: 10.31579/2690-4861/197
Copyright: © 2022 Thomas Amanda J, This is an open access article distributed under the Creative Commons Attributiosn License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 December 2021 | Accepted: 19 January 2022 | Published: 27 January 2022
Keywords: tracheostomy weaning; sialorrhea, hypersalivation; seizures; dysphagia; anti-epileptic drugs
We describe a single case following the acute hospital journey of a 54 year old admitted due to seizure activity and associated traumatic brain injury. The patient was cared for in a specialist neurosurgical centre. The hospital stay was complicated by difficulty managing seizure activity. The patient had several failed extubations due to high oral secretion burden, resulting in a percutaneous tracheostomy. Prolonged tracheostomy weaning ensued due to the impact of seizure activity, pharmacological interventions to manage both seizure activity and secretion management (including the use of Botulinum Toxin to the salivary glands), and dysphagia. Successful decannulation of tracheostomy was achieved 141 days after insertion and was associated with a reduction in anti-epileptic drug administration.
Glossary, Acronyms and Medical Abbreviations
Computed Tomography (CT), One Way Valve (OWV), Anti-epileptic drugs (AED’s), Nil By Mouth ( NBM), Electroencephalogram (EEG), Glasgow Coma Scale (GCS), Fibreoptic Endoscopic Evaluation of Swallowing (FEES), Pro re nata (PRN), Once a day (OD), Twice a day ( BD), Three times a day (TDS), Four times a day (QDS), Arterio Venous Malformation (AVM), Sub Dural Haemorrhage (SDH), Fibreoptic Nasendoscopy (FNE), no abnormality detected (NAD), Magnetic Resonance Imaging (MRI), Central Nervous System (CNS), One Way Valve (OWV), Activities of Daily Living (ADL), Multi-Disciplinary Team (MDT), Hospital Acquired Pneumonia (HAP), Percutaneous Gastroscopy (PEG), Nasogastric Tube (NGT).
Introduction
Sialorrhea is defined as excessive saliva or hyper-salivation commonly associated with drooling. Some neurological conditions can cause autonomic changes leading to primary sialorrhea [1], and impairments in swallow which may affect oral secretion clearance [2]. Studies have also demonstrated hyper-salivation in patients who are post ictal [3, 4]. The post-ictal presentation can also be associated with symptoms such as impaired consciousness, sensory and motor responses, hypersalivation and cognitive impairment [5].These symptoms have been shown to last from 3 seconds to 12.3 days [5]. There is a deficit of literature on the impact of excessive saliva production (or clearance) secondary to seizure activity on the tracheostomy weaning process.
Effective management of saliva permitting the removal of a tracheostomy can reduce the secondary complications of Tracheostomy insertion. Decannulation of tracheostomy restores physiological processes such as speech and swallow and may reduce the risk of aspiration, promote activities of daily living, progress physical rehabilitation, improve overall quality of life, facilitate hospital flow and reduce nursing/carer burden [6]. While management of sialorrhea with pharmaceutical agents such as anticholinergic drugs are often the first line approach, these have been associated with undesirable systemic effects due to inability to act specifically on salivary gland receptors (7). They have also been shown to affect the central nervous system, causing increased confusion, drowsiness and disorientation, which may be undesirable in the neurologically affected population [7]. Evidence demonstrates the efficacy of Botulinum Toxin for the management of excessive oral secretions with fewer systemic effects due to the direct effect on the salivary glands and longer duration of action [1, 2, 8].
We present a single case of tracheostomy weaning which was excessively prolonged by the impact of seizure activity, pharmacological intervention to manage seizures, excessive oral secretion and dysphagia.
54 year old admitted following witnessed tonic-clonic seizure and a fall. CT demonstrated right tentorial SDH with subarachnoid extension to the quadrigeminal cistern and posterior quadrant. Cerebral angiogram was NAD. The SDH was conservatively managed. Past medical history included alcohol excess and outpatient investigation for six month history of left sided odynophagia, voice change and weight loss. Pre-admission FNE and MRI were largely normal. Seizures persisted during the first 3 days of admission despite medical management with Levetiracetam (2g BD), Lacosamide (250mg BD), Lorazepam (1mg QD) and PRN Midazolam. On the 3rd day the patient was transferred to critical care with on-going seizure activity and reduced GCS, requiring propofol and fentanyl sedation and intubation. Sodium Valproate was added to the AED’s and ceftriaxone and acyclovir prescribed to cover possible CNS infection.
Ventilation requirements were minimal and a first trial of extubation occurred 4 days after critical care admission. This attempt failed due to high oral secretion load and on-going reduced GCS affecting airway protection. Two subsequent failed extubations in the following 5 days were due to an inability to manage oral secretions despite a trial of Hyoscine Hydrobromide. 11 days after critical care admission, a percutaneous tracheostomy with subglottic port was inserted. This step enabled liberation from mechanical ventilation and critical care discharge 5 days later.
Following critical care discharge, Hyoscine Hydrobromide was ceased in favour of Propantheline Bromide to help manage on-going high subglottic aspirates, oral and pulmonary secretions. Multiple AED’s were prescribed to control seizure activity (Levetiracetam 2g BD, Lacosamide 250mg BD, Sodium Valporate 1g BD, Clonidine 25mg QDS, Lorazepam PRN). Tracheostomy weaning commenced 6 days after insertion and progressed to 24 hours cuff deflation and OWV tolerance on the 17th day after insertion. At this time the patient exhibited a GCS of 14, was mobile with therapist assistance, participating in ADL and had been started on thin fluids. High oral and chest secretion persisted despite demonstrating effective swallow and strong cough.
Unexpectedly, the patient then experienced multiple seizures and a reduced GCS. EEG findings were consistent with status epilepticus requiring increased dosages of Sodium Valproate and Lacusomide, and the introduction of Clobazam and Tropitramate when seizures were refractory. Tracheostomy weaning was suspended and an increased oral secretion burden required an increased dose of Propantheline Bromide. Over the next 3 weeks focal seizure activity reduced on serial EEG’s but high oral secretion load persisted. Coupled with an ineffective swallow and drowsiness the patient was intolerant of short periods of cuff deflation and tracheostomy weaning was limited. At this stage, measured subglottic aspirates were in excess of 170mls over a 24hour period (see Figure 1).

46 days after tracheostomy insertion the MDT requested Botulinum Toxin to the bilateral submandibular glands, to reduce oral secretion and facilitate Tracheostomy weaning. Propantheline Bromide persisted (30mg TDS) but there was no significant change to oral secretion volume and after a further 14 days Hyociene Hydrobromide was recommenced (1.5mg patch). Tracheostomy weaning continued to be significantly limited by oral secretion load and prolonged coughing with cuff deflation. AED’s were gradually weaned at this time including Topitramate, Clobazam, and Levetiracetam. There was no further seizure activity reported and the patient was able to follow single stage commands, with minimal verbal output.
60 days after tracheostomy insertion, FEES revealed severe motor and sensory dysphagia and a score of 7 on the New Zealand Secretion Scale (see first assessment Table 1). There was frank aspiration of thin fluids, puree diet and secretions. There was no cough response to aspiration, voluntary cough was ineffective. There was moderate-severe arytenoid oedema bilaterally with the right appearing slightly worse and an abnormality noted on the right vocal fold, thought to be due to repeated intubation oedema.

67 days post tracheostomy insertion, the patient had a second injection of Botulinum Toxin, on this occasion both submandibular and parotid glands were injected bilaterally. 21 days following these injections there was a dramatic decrease in measured subglottic aspirates (to 7.5ml over 24 hours, see Figure 1) but the patient remained highly productive of pulmonary secretions and tracheostomy weaning remained limited. AED’s continued to be adjusted with increased doses of Levetiracetam and Clobazam.
88 days post tracheostomy insertion, cuff deflation had progressed to 1 hour twice a day. Bedside swallow assessment revealed improved tolerance to thin fluids with no overt signs of aspiration. Videofluoroscopy was unable to be completed due to lack of patient alertness for the procedure, but repeat FEES revealed a reduction in the volume of secretions penetrating the laryngeal vestibule with all consistencies trialled (see second assessment, Table 1).
100 days post tracheostomy insertion, the patient had progressed to 12 hours cuff deflation with OWV tolerance, but respiratory deterioration temporarily suspended weaning progress. Transient motor seizures accompanied this HAP required further adjustments to prescribed AED’s (Levetiracetam, 2g BD, Sodium Valoprate, 1.3g BD, Clobazam, 20mg BD, Lacosamide, 300mg BD).
107 days post tracheostomy insertion the patient showed improvements in alertness and engagement, responding to questions and following single stage commands. Cuff deflation remained at 15 minute tolerance due to prolonged coughing, reduced swallow frequency and anterior loss of secretions (drooling) although measured subglottic aspirates remained minimal over a 24 hour period.
130 days post tracheostomy insertion, the patient had a failed PEG insertion due to iatrogenic bowel perforation and was made NBM, preventing administration of NGT Clobazam. Subsequently a 55 minutes seizure occurred requiring the addition of Phenytoin. Pulmonary secretions remained high, though measured subglottic aspirates had not been significant and all drying agents were stopped. No Tracheostomy weaning occurred during this period.
141 days post insertion tracheostomy weaning was recommenced, and quickly progressed to 12 hours cuff deflation during daylight hours with OWV tolerance. Repeat FEES 148 days post tracheostomy insertion (see third assessment, Table 1) showed significantly improved secretion management, nil aspiration or penetration and the patient was recommended to commence thin fluids and easy chew diet. Seizure activity was well controlled with AED’s weaned to a therapeutic dose: Levetiracetam 2g BD, Sodium valproate 1.3g BD, Lacusomide 300mg BD with continuation of Escitalopram 15 mg OD for mood. Tracheostomy weaning, alertness and engagement continued to progress and 159 days post tracheostomy insertion the tracheostomy was replaced with a mini-tracheostomy to accommodate ongoing pulmonary secretion requirements. The mini-tracheostomy was removed 6 days later.
Challenges with oral secretion management can be a barrier to tracheostomy weaning and decannulation. In our case, tracheostomy weaning was limited by high volumes of oral and chest secretion evidenced by frequent coughing of secretions from the tracheostomy and frequent tracheal suctioning requirements. Conservative management of sialorrhea usually includes MDT input for erect posture maintenance, mobilisation, swallow rehabilitation and biofeedback [6]. In our case, use of these approaches was limited by the patient’s reduced GCS, therefore pharmaceutical agents were considered. There is limited evidence for the use of drying agents during the acute management of patients with acquired brain injury. The use of these medications is derived from research describing their use in other populations such as Cerebral Palsy, Parkinson’s disease, Motor Neurone Disease and Palliative Care.
The accepted pharmaceutical management of Sialorrhea are anticholinergic drugs due to their ability to bind to muscarinic receptors. Anticholinergic drugs are also favoured due to ease of availability and administration. However, anticholinergic drugs may cause undesirable systemic parasympathetic effects, such as; cardiac arrhythmias, constipation, headaches, blurred vision, urinary retention and drowsiness (Table 2) [7]. Some anticholinergic drugs such as glycopyrronium and propantheline show a reduced affinity to cross the blood brain barrier and are often the agent of choice in the neurological cohort [9]. In cases where use of anticholinergic drugs have been shown to be ineffective or unsuitable due to side effects, the administration of Botulinum toxin should be considered [1,6].
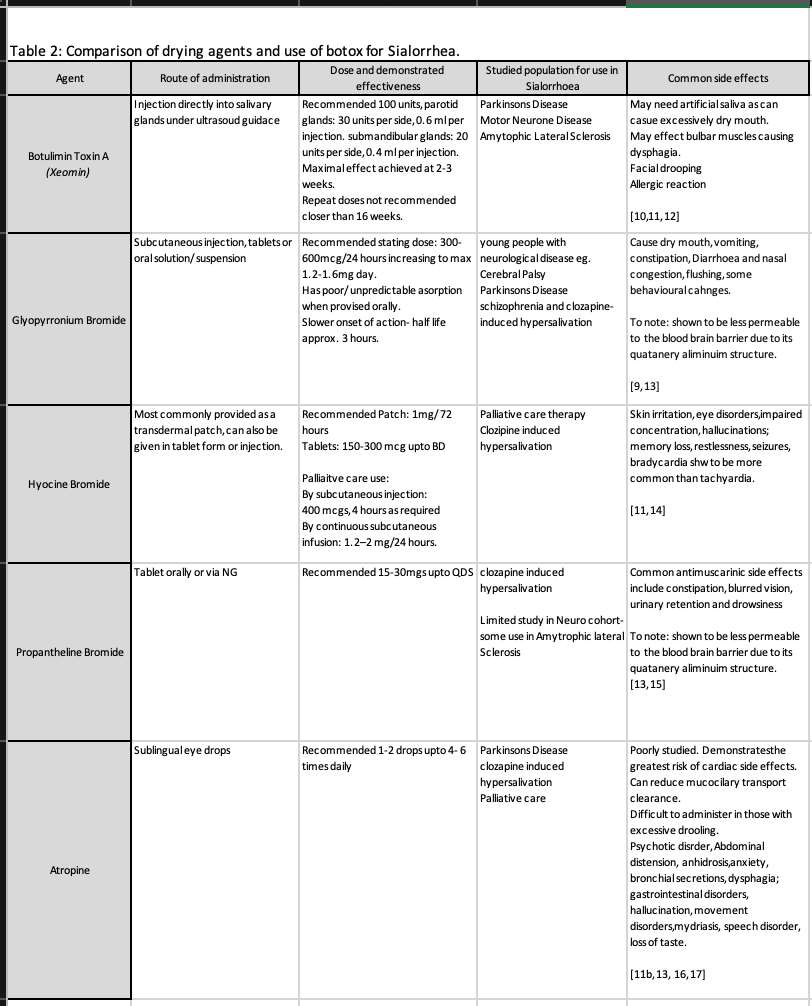
Botulinum Toxin is a neurotoxic protein produced by the bacterium clostridium botulinum. It has been used since the 1970’s for the therapeutic management of conditions such as dystonia, spasticity, strabismus and eye spasms. It has shown to have good efficacy on hyper-salivation when administered directly to the salivary glands [2, 6]. Botulinum prevents the release of the neurotransmitter acetylcholine at the neuromuscular junction causing irreversible functional denervation which may last until the growth of new synapses [8]. Saliva production is mediated by parasympathetic nervous system control of three major paired salivary glands, two parotid, two submandibular and two sublingual. Research suggests the highest efficacy of secretion reduction is targeted Botulinum to the parotid and submandibular glands bilaterally [1] with the parotid glands receiving a higher dosage [18]. Botulinum can last an average of 3-6 months when administered under ultrasound guidance [19, 20]. There is evidence in some populations that drooling scores do not return to baseline for 12 months following Botulinum injection [20].
Our case demonstrated significant improvement in saliva production as evidenced by the reduction in daily subglottic aspirate volume 3 weeks after the second round of Botulinum was administered (see Figure 1). The second administration targeted both parotid and submandibular glands in comparison to the first round, when only the submandibular glands were injected. Evidence suggests the maximum response to Botulinum is achieved 2-4 weeks after administration [20, 21]. Reduced saliva production in our case was correlated with progression of the tracheostomy wean but final progression toward decannulation readiness continued to be limited by the patients reduced cognitive function, engagement and reliance on high doses of AED’s for the management of seizures. AEDs have been known to affect salivary gland function and can cause both sialorrhea and salivary gland hypofunction [22].
Typically, patients compensate for increased secretions through an increased frequency of swallow. In our case dysphagia impacted the ability to do this effectively. There were multiple factors which may have contributed to dysphagia, including; presence of an acquired brain injury, reduced GCS related to seizure activity, poly-pharmacy for seizure management, decompensation from a period of prolonged intubation and a prolonged period of NBM. Medications that depress the central nervous system such as AEDs (Sodium Valproate and Lorazepam) and Benzodiazepines can negatively impact swallow causing reduced awareness, reduced voluntary muscle control and difficulty initiating a swallow [23]. Dysphagia has been a noted side effect in 20% of patients on either single or multiple AEDs [24]. Dysphagia can manifest itself in terms of movement disorders, myopathy and salivary changes [25]. In addition to causing increased drowsiness, benzodiazepines may induce or exacerbate pharyngeal dysphagia by suppressing brainstem swallowing regulation [25]. In the case presented here, improved swallow function appeared in conjunction with therapeutic weaning of AED’s. While it is difficult to attribute a single cause for successful tracheostomy weaning in the case presented, improved seizure status, reduction of secretion volume (with Botulinum toxin) and improved swallow following the reduction in AED’s combined to allow the Tracheostomy to be removed.
Tracheostomy presence has been associated with significant impacts on quality of life [2, 26] and patient flow through a rehabilitation pathway. The MDT management of tracheostomy therefore focuses on the goal of successful decannulation. There are a number of criteria that must be fulfilled prior to considering decannulation, including prolonged tolerance to cuff deflation, and management of oral secretion load through functional swallow. In the case presented, secretion management and coughing associated with salivary aspiration significantly impacted the ability to progress the tracheostomy wean. Both oral secretion volume and dysphagia appear to have been negatively impacted by the use of multiple AED’s to manage seizure activity. These drugs also impacted on the patients level of alertness and ability to engage consistently in rehabilitation sessions (sitting out of bed and mobilisation). In the case presented, pharmacological management of excessive oral secretion using Botulinum toxin and improved dysphagia coincident with the reduction of AED’s appeared to remove the barriers preventing decannulation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
