
Review Article | DOI: https://doi.org/10.31579/2692-9406/108
1RBVRR Women’s College of Pharmacy, Barkatpura, Hyderabad, Telangana, India.
2Dr. B.R.K.R Government Ayurvedic college Hyderabad, Telangana, India.
*Corresponding Author: Jangampally Vedhashree, RBVRR Women’s College of Pharmacy, Barkatpura, Hyderabad, Telangana, India.
Citation: Shailaja K, Kanth S, Vedhashree J, Kirthi R, Deepa R. M. (2022). Ayurvedic Formulations for the Treatment of Covid -19. Biomedical Research and Clinical Reviews. 6(4); DOI: 10.31579/2692-9406/108
Copyright: © 2022 Jangampally Vedhashree, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 February 2022 | Accepted: 12 March 2022 | Published: 17 March 2022
Keywords: acuterespiratorysyndrome (ARS); molecular docking; molecular dynamics; withaniasomnifera (ashwagandha); corona virus (cov-2)
Background and objective: To recognize natural phytochemicals from medicinal plants, in order to reutilize them against COVID-19 by the virtue of molecular dynamics (MD) simulation study and molecular docking study COVID-19 is a transmissible disease that is initiated and propagated through a new virus strain SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus-2). Since 31st December 2019 in Wuhan city of China and the infection has outspread globally infecting many countries.
Methods: Molecular dynamics MD simulation interaction analysis, Salt bridge analysis, Flexibility analysis, Ace-2- rbd complex electrostatic component of binding energy calculation method.
Results: Molecular docking studies has shown to be having two inhibitors against SARS-CoV-2 Mpro (Main protease), from Withania somnifera (Ashwagandha) (Withanoside V [10.32 kcal/mol] and Somniferine [9.62 kcal/mol]). Inconsolably, SARS-CoV-2 infection in patients with pre-existing disease conditions (e.g., hypertension and diabetes) can cause severe complications and, as a result, mortality.
Conclusion: Hence from the present study it could be suggested that, the active phytochemicals from medicinal plants could potentially inhibit Mpro of SARS-CoV-2 and further equip the management strategy against COVID-19-a global contagion. Active phytoconstituents of Ayurvedic medicinal plants Withania somnifera (Ashwagandha) predicted to significantly hinder main protease (Mpro or 3Clpro) of SARS-CoV-2.Through molecular docking and molecular dynamic simulation study, Withanoside V, Somniferine were observed to impede the activity of SARS-CoV-2 Mpro.
As per Ministry of Health and Family Welfare India, till 26th July 2020 there are 1,385,522 confirmed cases, and 467,882 active cases, among which 32,063 deaths and 885,576 recovered cases have been reported. Corona viruses (CoV) are from the family Coronaviridae(beta strain) which leads to maladies of the vital organs like respiratory, enteric, hepatic and neurological systems if not treated. CoV is a single stranded RNA virus (having diameter of 80–120 nm), among which not long ago SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus-2) has arose as a universal contagion ( infecting humans )with 3–4% mortality rate (Zhu et al., 2020). , .Bats (Owing to zoonotic origins and genetic similarity), are pondered as the natural hosts of SARS-CoV-2 having four structural proteins namely Spike (S), Envelope (E), Membrane (M) and Nucleocaspid (N). Corona virus recognizes the receptor on the target cell, fusion with membrane receptor causing infection and further transmission within the host. Affinity of SARS -CoV with novel SARS-CoV-2 which binds ACE2 far greater than threshold requisite for virus infectivity, but the pathological effects for causing organ damage remained to be elucidated. This binding factor is the vital reason for swift transmission potentiality of the SARS-CoV-2 as compared to SARS-CoV [4,10].
The first line of action is to obstruct the locking of virus towards the host ACE-2 receptors by blocking the Spike proteins, which would help to cut down the figure of new cases. But in so far infected cases to provide remedy, target for main proteases (Mpro) is being searched out as it translates the viral RNA into functional polyproteins altering the normal physiology by development of viral RNA polymerase, exoribonuclease and endoribonuclease. Mpro, also called 3CLpro (3C-like protease or chymotrypsin-like protease) has two parts owning six stranded antiparallel β barrels, holding substrate binding site in the middle of them, with cluster of five helices which are majorly responsible for dimerization of the enzyme. The majority of the Coronaviridae genome has two types of polyproteins, pp1a and pp1ab. With the help of two proteases 3CLpro and PLproencoded by the open reading frame, the indicated polyproteins are cleaved and further transformed in mature non-structural proteins (NSPs).
Conventional pharmaceuticals and bioactive natural compounds have good biocompatibility, bioavailability and less toxic. Papain-like protease(s) Mpro is essential for dispensing polyproteins at 11 various sites to produce proteins that are translated from the viral RNA. Restraining of the pursuit of Mpro would impede viral replication process in the core of the host. Considering there is no other human protease enzyme known with similar cleavage specificity at sites of Leu-Gln↓(Ser, Ala, Gly) is known till date, the inhibitors of these targets are likely to be non-toxic. Among all the prospective protease inhibitors, the antivirals Nelfinavir, Remdesivir, Lopinavir and Ritonavir and α-ketoamide are peculiarly striking as therapeutics to battle the new corona virus. Apart from these, various combinations of anti-vials such as Lopinavir, Ritonavir, Favipiravir, anti-malarial (Chloroquine, Hydroxychloroquine) and corticosteroid (Dexamethasone), therapy are being used for controlling COVID-19. Thus, SARS-CoV-2 Mpro have recently emerged as the better targets in inhibiting virus replication. The present study captivated on the main proteases of SARS-CoV-2 as potential macromolecular target for COVID-19 management using active phytoconstituents mentioned in Ayurvedic scriptures [1].
Pathophysiologyof Corona Virus:
Mechanism of SARS-CoV-2 invasion into host cells:
Corona viruses are anenvelope, single-stranded RNA viruses of ~30 kb. They are known to infect a wide variety of host species. They are widely divided into four genera (α, β, γ, and δ) based on their genomic structure. α and β corona virusesare observed to infect only mammals. Human corona virus 229E, NL63 is responsible for common cold and belongs to α corona virus. In contrast, SARS-Covid, Middle East respiratory syndrome corona virus (MERS-Covid) and SARS-CoV-2 are classified to β corona viruses.
The life cycle of the virus within the host consists of 5 steps: attachment, penetration, biosynthesis, maturation and release. Once a virus binds to the host receptors (attachment), they enter host cells through endocytosis or membrane fusion (penetration), viral contents are then released inside the host cells, and viral RNA enters the nucleus for replication. By using viral mRNA viral proteins are made (biosynthesis). These new viral particles are made (maturation) and released. Corona virus consists of four structural proteins; Spike (S), membrane (M), envelope (E) and Nucleocapsid (N). Spike consists of a transmembrane trimetric glycoprotein protruding from the viral surface and internally comprises two functional subunits; S1 subunit is responsible for binding to the host cell receptor and S2 subunit is for the fusion of viral as well as cellular membranes. ACE 2 was identified as one of the functional receptor for SARS-Covid. Structural and functional analysis showed that the spike for SARS-CoV-2 also bound to Angiotensin converting enzyme. This expression was found to be high in lung, heart, ileum, kidney and bladder. SARS-CoV-2 may or may not bind to an additional target need further investigation. Once the binding of SARS-CoV-2 to the host protein is done, the spike protein undergoes protease cleavage. A two-step protease cleavage to activate spike protein of SARS-Covid and MERS-Covid was proposed as a model (consisting of cleavage at the S1/S2 cleavage site for priming and a cleavage for activation at the S′2 site), the position adjacent to a fuse the peptide within the S2 subunit.Postcleavage at the S1/S2 cleavage site, S1 and S2 subunits remain non-covalently bound. The distal S1 subunit contributes towards the stabilization of the membrane-anchored S2 subunit at the perfusionstate. The next cleavage at the S′2 site presumably activates the spike for membrane fusion via irreversible, conformational changes. The corona virus spike is unusual among viruses because a range of wide spread proteases can cleave and activate it. The uniquecharacteristicsofSARS-CoV-2 is the existence of furin cleavage site (“RPPA” sequence-Reverse phase protein array) at the S1/S2 site, which was entirely subjected to cleavage during biosynthesis in a drastic contrast to that of SARS-CoV spike, which was incorporated into assembly without cleavage.Nonetheless,the S1/S2 site was also subjected to cleavage by different proteases such as transmembrane protease serine 2 (TMPRSS2) and cathepsin L, the ubiquitous expression of furin likely makes this virus clearly pathogenic.
Host response to SARS-CoV-2
Major symptom of the patients infected with SARS-CoV-2 ranges betwixt minimal symptoms to severe respiratory failure with multiple organ failure. On Computerized tomography scan, the characteristic pulmonary ground opacification can be seen even in asymptomatic patients. SinceACE2 is highly expressed on the apical side of lung epithelial cells present in the alveolar space; this virus can likely enter and destroy them. This tones down with the fact that the early lung injury was often seen in the distal airway. The Epithelial cells, alveolar macrophages and dendritic cells are the three main components for innate immunity. Dendritic cells reside beneath the epithelium and Macrophages are located at the apical side of the epithelium. Dendritic cells and macrophages serve as innate immune cells to fight against viruses till adaptive immunity is involved.
T cells show mediated responses against corona virus which has been previously reviewed. T cell responses are initiated by an antigen presentation via Dendritic cells and macrophages. A question rises, how does SARS-CoV-2 enter APCs? Dendritic cells and macrophages can phagocytise apoptotic cells infected by virus. For instance, virus-infected apoptotic epithelial cells can be phagocytised by Dendritic cells and macrophages, which further leads to an antigen presentation to T cells. Or Dendritic Cells and macrophages may be infected with virus primarily? Depending on the Immunological Genome database (http://rstats.immgen.org), the expression of ACE2 on dendritic cells and alveolar macrophages is limited but is present. Determining if SARS-CoV-2 uses another protein or not to bind to APCs helps to answer this question. SARS-CoV can also bind to dendritic cell specific intercellular adhesion molecule-3-grabbing non-integrin (DC-SIGN) and its related protein (DC-SIGNR, L-SIGN) in addition to ACE2. DC-SIGN is highly interpreted by expression on dendritic cells and macrophages. Collateral target for SARS-CoV-2, if any, can help the virus to directly infect Dendritic Cells and alveolar macrophages. Though This needs further research. These antigen presenting cells reach the draining lymph nodes to present viral antigens to T cells. CD4+ and CD8+ T cells play a vital role where CD4+ T cells activate B cells to promote the production of virus-specific antibody, while CD8+ T cells can kill viral infected cells.
Immunological studies were only reported in patients with severe COVID-19. Patients with severe underlying diseases showed lymphopenia, mostly the reduction in peripheral blood T cells and the patients were reported to have increased plasma concentrations of pro-inflammatory cytokines, including interleukin (IL)-6, IL-10, granulocyte-colony stimulating factor (G-CSF), monocyte, chemo attractant protein 1 (MCP1), macrophage inflammatory protein (MIP)1α, and tumour necrosis factor (TNF)-α. The more severe the condition is, the higher their IL-6 levels were. CD4+ and CD8+ T cells were activated in only those patients as suggested. Mostly by higher expression of CD69, CD38 and CD44. High percentage of checkpoint receptor Tm3+PD-1+ subsets in CD4+ and CD8+ T cells showed that T cells were also exhausted. NK group 2 member A (NKG2A), another marker for exhaustion was elevated on CD8+ T cells. Exhaustion of T cells could have led to the progression of the disease. Another interesting finding was that aberrant pathogenic CD4+ T cells with co-expressing interferon (IFN)-γ and granulocyte-macrophage colony-stimulating factor (GM-CSF) were seen in COVID-19 patients with severe disease. GM-CSF production from T cells has been formerly reported as a response to virus infection. GM-CSF helps to differentiate between innate immune cells and augment T cell function, but it can initiate tissue damage at excess.To sum up GM-CSF+IFN-γ+ CD4+ T cells were previously seen upon highT cell receptor (TCR) responses in experimental autoimmune encephalomyelitis models, where the CD8+ T cells expressing GM-CSF were found at greater percentage and secreted IL-6. It is to mention that these immunological studies were exclusively reported from adult patients. Immunological responses in paediatric population needs more detailed examination. This study of SARS-CoV showed that virus which infected lung epithelial cells produced IL-8 in addition to IL-6, where IL-8 is a well-known chemo attractant for neutrophils and T cells. Infiltrations of a very large number of inflammatory cells were noticed in the lungs of severe COVID-19 patients, and these cells supposedly consist of a constellation of innate immune cells and adaptive immune cells. Among innate immune cells, we expect that the majority of them to be neutrophils, they can act as double-edged sword as they can induce lung injury. The majority of the observed infiltrating adaptive immune cells were likely to be the T cells. CD8+ T cells are primary cytotoxic T cells. Severe patients showed pathological cytotoxic T cells derived from CD4+ T cells, which can kill virus but also contribute to lung injury. Circulating monocytes respond to GM-CSF which is released by these pathological T cells. CD14+CD16+ are the inflammatory monocyte subsets, which seldom exist in healthy controls and were also found at significantly higher percentage in COVID-19 patients. These inflammatory CD14+CD16+ monocytes have high expression of IL-6, which are likely accelerated the progression of systemic inflammatory response.
An interesting fact here is that ACE2 was significantly expressed on innate lymphoid cells (ILC)2 and ILC3.As NK cells are a part of ILC1, which contain a large portion of ILCs in the lung (~95%). ILC2 and ILC3 work for mucous homeostasis. So far there is a very limited study of ILC2 and ILC3 in corona virus infection.
In addition to the respiratory symptoms, thrombosis and pulmonary embolism was observed in severe diseases. This is in relation with the finding that elevated d-dimer and fibrinogen levels were observed in severe diseases. The function of the endothelium includes promotion of vasodilation, fibrinolysis, and anti-aggregation. Since endothelium plays a significant role in thrombotic regulation, hypercoagulable profiles seen in severe diseases likely indicate significant endothelial injury. Endothelial cells also express ACE2. Of note, the endothelial cells represent the one third of lung cells. Micro vascular permeability is a result of the endothelial injury can facilitate viral invasion.
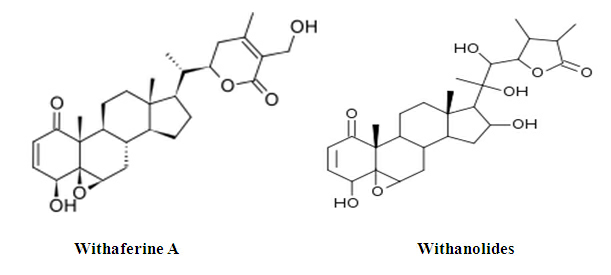
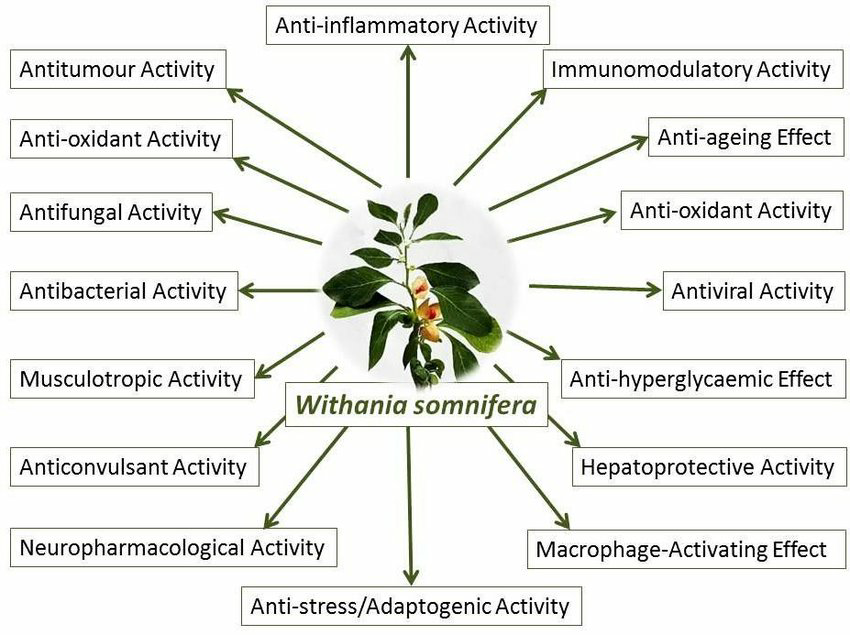
AyurvedaApproaches for studying antimicrobial susceptibility and discovering new antimicrobial agents from the plants and other natural sources have been extensively utilized. Withaniasomnifera, commonly known as Ashwagandha or Indian ginseng or winter cherry, is a popular medicinal plant in Ayurvedic medicine. The principal active compounds include several withanolides. Various plant parts, like roots and leaves and fruits of Ashwagandha, have been used as plant-derived medicines. The plant possesses various different therapeutic and pharmacological activities including antimicrobial activity. Many bacterial, fungal and viral species have been used as a test microorganism for the assessment of the antimicrobial activity of extracts and purified compounds of various plant parts of Ashwagandha.
Ashwagandha: animportantmedicinalplant
Withaniasomnifera, commonly known as Ashwagandha or Indian ginseng or winter cherry, is a renowned medicinal plant in Ayurvedic medicine. The principal active compounds include several withanolides. Due to the great medicinal value and nonhazardous property, it is commonly used all over the world. Roots (mostly used), and leaves and fruits (less often), have been used as phytomedicines in the form of decoction, infusions, ointment, powder, and syrup. These days, it is cultivated and used as a crop to maintain the high demand of biomass and a sustainable eminence for the requirements of pharmaceutical industry. Ashwagandha is an important herb in the Ayurvedic and indigenous medicine system for over 3000 years. It belongs to the family Solanaceae and possess a chromosome number 2n=48. In the India, only two species of Withania are found i.e. W. somnifera and W. coagulans. This plant shows use as a home remedy for numerous diseases in India and many parts of the world. In India grown abundantly in regions like Rajasthan, Madhya Pradesh, Himachal Pradesh, Punjab and Uttar Pradesh. It is considered as ‘Indian ginseng’ in the conventional Indian medicine. It is used as a liver tonic, anti-inflammatory, antioxidant, antimicrobial agent and cure for asthma. Withaferin-A has been receiving a good deal of attention because of its antibiotic and antitumor activity19. In Unani system of medicine, roots of Withaniasomnifera usually known as Argand are utilized for the medicinal properties. In Ayurvedic system of Medicine, Ashwagandha is claimed to have effective aphrodisiac rejuvenating and life extending properties. It has an overall animating and regenerative abilities and is used among others, for the treatment of nervous exhaustion, insomnia, memory related conditions, skin problems, tiredness potency issues and coughing. The traditional use of Ashwagandha was to escalate immunity, energy, youthful vigor, strength, endurance, health, increase vital fluids, nurture the time elements of the body, muscle fat, lymph, blood, cell production and semen. It helps to counteract chronic fatigue, dehydration, weakness, bone weakness, impotency, thirst, premature aging emaciation, muscle tension, debility and convalescence. It aids invigorate the body by rejuvenating the reproductive organs, just as a tree invigorates by feeding the roots.The biologically active chemical constituents are alkaloids (ashwagandhine, Ana hygrine, Cusco hygrine, tropine etc.), steroidal compounds i.e., withaferin A, withasomniferin A, ergostane-type steroidal lactones, withanolides A-Y, withasomniferols A-C, withasomidienone, Withanone etc. Withaferin and withanolide A are the chief withanolidal active components isolated from the plant. These compounds are chemically similar but varied in their chemical constituents [9].
Ethanolic extract of the dried roots or leaves of the plant was preparedandconcentrated under pressure at 50 ± 5 °C and was analyzed for main compounds (withanolides and Withaferin A) by HPLC. All the important components were found to be present in accessions (AGB 002, AGB 009, RSS 009, RSS 033). Correlation of these components with their genetic factors, was undertaken using AFLP (amplified fragment length polymorphism) markers. Out of 64 primers 7 yielded optimum polymorphism [5].
Withaniasomnifera for the treatment of Covid:
Molecular docking:
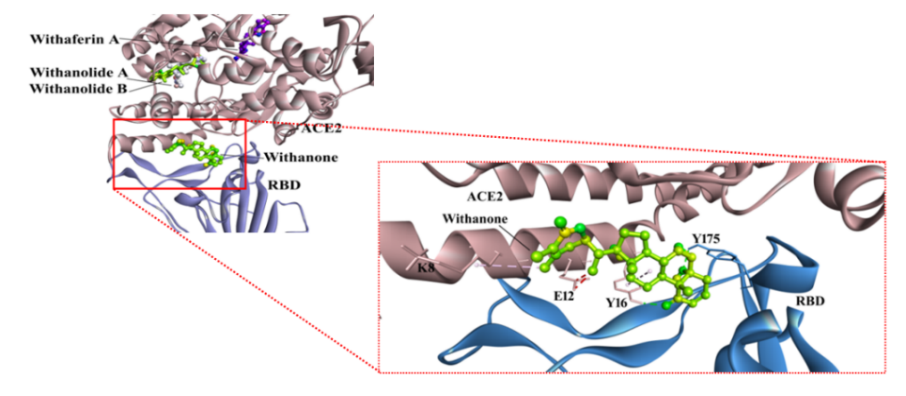
Withanolides present in roots and leaves of W. somniferaare docked against ACE2-RBD complex. The phytocompound which bound to the interface was forced to targeted/focused docking.Thephytocompoundsare bound at the ACE2-RBD complex tightly. Of these compounds, only the Withanone bound at the interface of the receptor and RBD fig: [3] Therefore, Withanone was analyzed further to study its role in weakening the interactions between the ACE2 receptor and RBD. In this process of targeted docking of the Withanone, it was found to be well-bound at the ACE2-RBD interface by two H-bonds (Tyr16 of ACE2 and Tyr175 of RBD to Withanone), alkyl and van der Waals interactions fig: [3]. The Tyrosine’s were then mutated by alanine, and re-docked with Withanone [2, 7].
Molecular dynamics MD simulation interaction analysis:
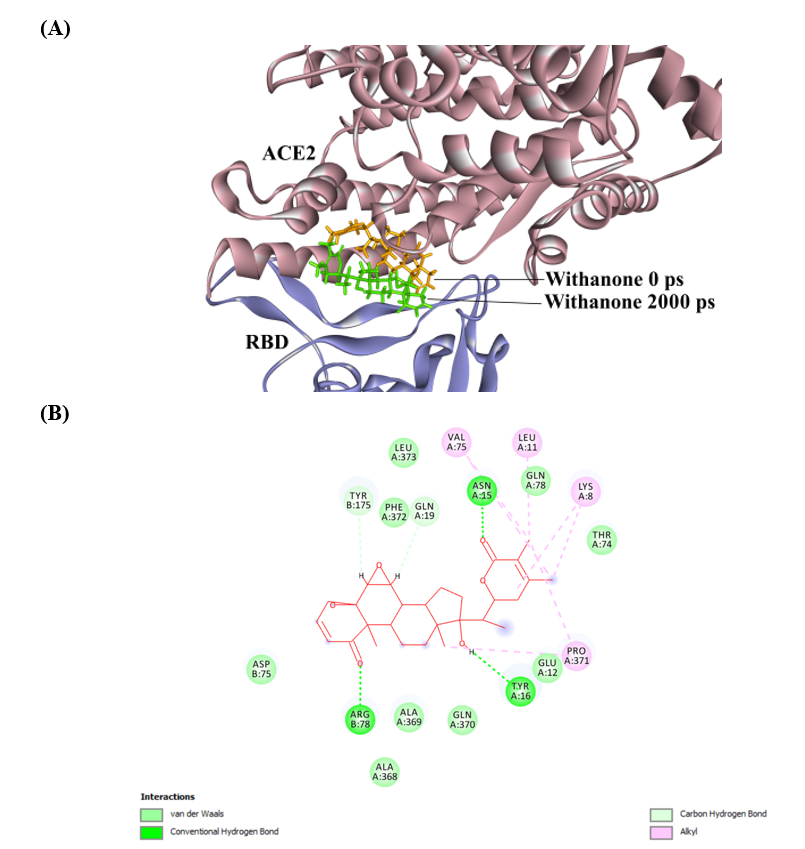
The RMSD of simulated molecule (Withanone) was 5.08 Å compared to starting position. At the end of simulation, it moved slightly towards the binding interface center fig: [4A]. On analyzing, the ligand interaction, it was found that ACE2 Y16 H-bonding to Withanone was preserved in the simulated coordinates, whereas RBD Y175 forms Carbon H-bond to Withanone. Additionally, there is formation of three more H-bonds (ACE2 N15, ACE2 Q19 and RBD R78 to Withanone) in the simulated ligand-ACE2-RBD complex fig: [4A] [3].
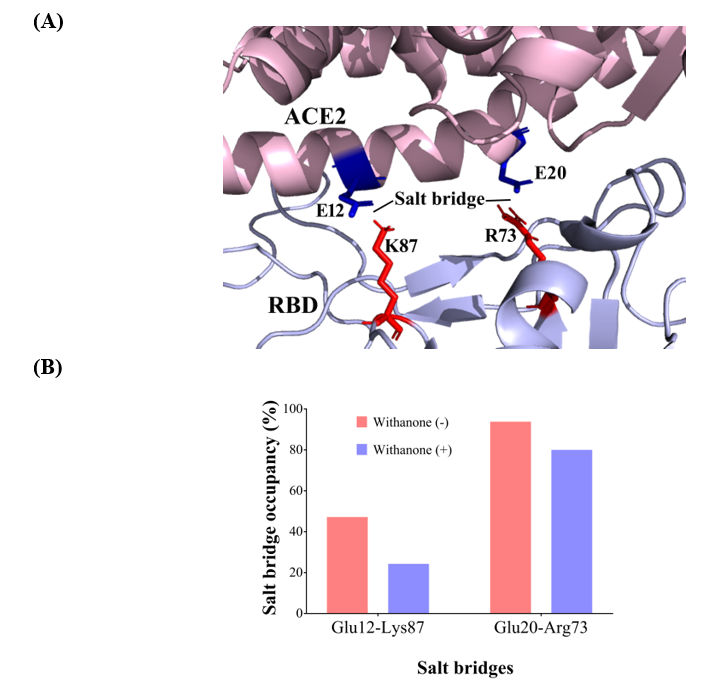
Salt bridge analysis:
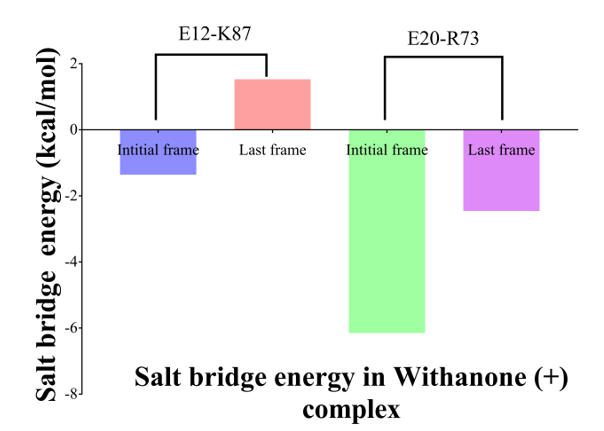
Two inter-chains (binding interface) were detected at salt bridge interactions, Glu12 OE2– Lys87 NZ (2.75 Å) (aa 404) and Glu20 OE2 – Arg73 NZ (2.67 Å) (aa 390). Val residue (aa 404) in SARS-CoV is substituted by Lys in COVID-19 S protein RBD, and Lys (aa390) is substituted by Arg Fig: [5]. These were also seen during the simulation. Percent occupancy of Glu12-Lys87 salt bridge was decreased to 24.3% in the simulation trajectories with the Withanone, from 47.2% present in the trajectories without the ligand. Likely, occupancy of Glu20-Arg73 salt bridge in the trajectories with the Withanone was 80%, while it was 93.8% in the trajectories without the ligand. Energetics of the two salt bridges (E12-K87 and E20-R73) was enumerated. It was -1.36 kcal/mol and 1.53 kcal/mol in the beginning and last frame for the salt bridge E12-K87, whereas it was estimated to be -6.15 kcal/mol and -2.46 kcal/mol for the salt bridge E20-R73 fig: [6].
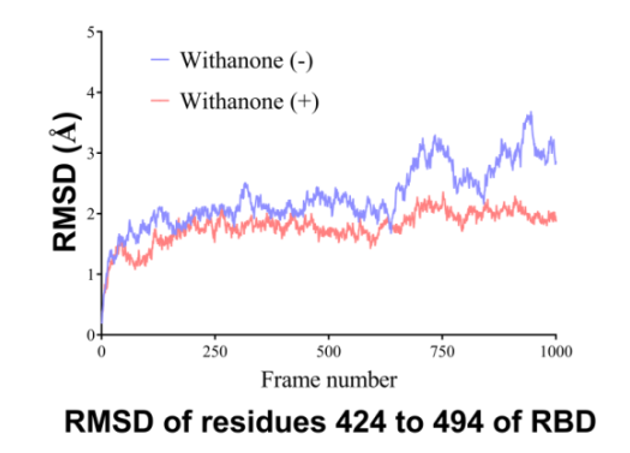
Flexibility analysis:
For local flexibility analysis, total RMSD of non-H atoms of the binding interface residues of RBD, RMSD of non-H atoms of aa 424 to 494 was determined fig: [7]. The data shows the local RMSD changes. RMSD was seen to be reduced in the simulation of Withanone plus case, in the region of aa 424 to 494 (binding interface residues in RBD).
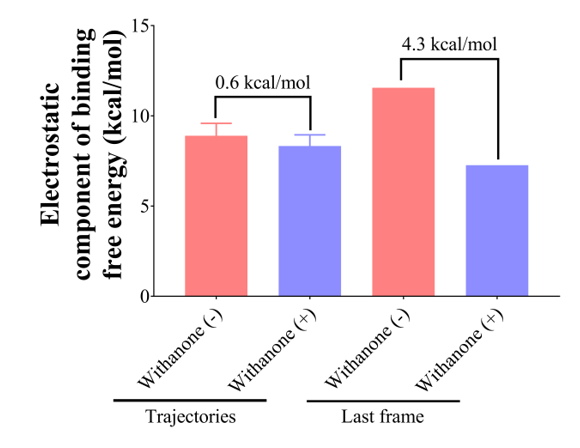
Ace2-rbd complex electrostatic component of binding energy calculation:
In MD simulation, a total 210 and 217 clusters were obtained upon clustering analysis of the trajectories with or without Withanone, respectively. The electrostatic component of ACE2-RBD complex were estimated on the last 100 ps representative trajectories of the cluster (11 trajectories, without the ligand; 10 trajectories, with the ligand) using Delphi, to assess the hypothesis that the proposed Phyto-compound weakens the interactions between ACE2 and RBD. The ΔΔGelof the complex with the ligand (7.27 kcal/mol) was decreased by 4.3 kcal/mol as compared to that without the ligand (11.55 kcal/mol), when estimated in the final trajectories, and it was observed to be decreased by 0.6 kcal/mol when estimated on the last 100 ps representative trajectories (8.89 and 8.33 kcal/mol in the trajectories without or with the ligand, respectively) fig: [8]. This indicates that the binding of Withanone at the interface of the ACE2 and RBD weakens their interactions [2].
We have both allopathic and ayurvedic system of medicines to treat covid but, the allopathic system of medicines not only treat the covid but they also bring many complications to the human system, which sometimes may lead to death of the patient. Ayurvedic system of medicine is not only old but it is also very effective with less side effects and has many alternative benefits too. This system is practiced from golden era and has always helped man-kind to get rid of many typical diseases. Indian medicine system is mainly dependant on herbal products and evidences based. Once they are found to be working for any disease, nothing wrong to use and experiment them as they are not showing any major side effects. In that way Ashwagandha is been tried for Covid19 also. At a certain point of time, we will be able to find out the actual cellular mechanism by taking up molecular level research. This is the case of Turmeric. It was used traditionally over 100 of years based on evidences. Now various research findings are coming on its medicinal properties and clinically it is proved to be effective. Every time it is not necessary to follow the allopathic system for finding out new chemical medicines. One who knows how to use ayurvedic medicines in a right way never gets disappointed. It is mainly due to lack of knowledge and own personal fears most of the people stopped referring ayurvedic medicines. People prefer allopathic medicines to obtain fast results. But here, they forget that every allopathic medicine has its own adverse drug reactions, which sometimes may lead to severe complications in the biological system. It is the time that mankind should start adapting Ayurveda to not only prevent the complications of disease, but also to bring balance to thevata, pitta, and kapha which are known as Tridoshaof the body.
S-protein-Spike protein; Covid-19-Corona virus 2019; ACE2- Angiotensin converting enzyme-2; RBD- Receptor binding domain; 2019-nCoV- Novel Coronavirus 2019; MD- Molecular dynamics; CCDCP-Chinese Center for Disease Control and Prevention; SARS-CoV, Severe Acute Respiratory Syndrome-Coronavirus; MERS-CoV- Middle East Respiratory Syndrome-Coronavirus; nAbs- Neutralizing antibodies; N-terminal- Amino terminal; C-terminal- Carboxy terminal; PBE- Poisson-Boltzmann equation; ADT4-Auto dock Tools 4; NAMD-Nanoscale molecular dynamics; VMD- Visual molecular dynamics; RMSD- Root mean square deviation; E20-R73- Glu20-Arg73; E12-K87- Glu12-Lys87; aa491- Amino acid 491; RBM- Receptor binding motif.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
