
Case Report | DOI: https://doi.org/10.31579/2692-9759/059
1 Division of Cardiology, University of New Mexico, Albuquerque NM and
2 Heart Institute, Geisinger Medical Center, Danville PA
*Corresponding Author: James Blankenship, Division of Cardiology, University of New Mexico, Albuquerque NM.
Citation: : Carmel Moazez, Carlos V. Sosa, Lucas C-Lutrick, Tanawan Riangwiwat, James Blankenship (2022) Axillary and Brachial Artery Thrombosis after Left Radial Access for Coronary Angiography. Cardiology Research and Reports. 4(4); DOI: 10.31579/2692-9759/059
Copyright: : © 2022 James Blankenship, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 March 2022 | Accepted: 01 April 2022 | Published: 20 April 2022
Keywords: thrombosis; electrocardiography; hydrophilic
One case of brachial artery occlusion and no cases of axillary artery occlusions have been reported in the literature. Here we describe a case of a 50 years old female who presented for diagnostic coronary angiogram after having a positive stress test who developed a brachial, axillary and radial artery thrombosis after left transradial access.
Summary: Radial artery occlusion is one of the most commonly reported complications of transradial access. One case of brachial artery occlusion and no cases of axillary artery occlusions have been reported in the literature. Here we describe a case of a 50 years old female who presented for diagnostic coronary angiogram after having a positive stress test who developed a brachial, axillary and radial artery thrombosis after left transradial access.
Background
In the last decade, more operators have transitioned to a radial access approach as opposed to femoral access for coronary angiography due to lower bleeding rates, less vascular complications, earlier ambulation and comfort for the patient [1,2]. Radial artery thrombosis occurs in 5-10% of patients undergoing radial access for coronary angiography but its incidence may be underestimated due to the lack of patient symptoms [3]. While radial artery occlusion is fairly common, thrombosis of more proximal arteries after radial access is rare. We present what we believe is the first reported case of axillary thrombosis complicating transradial diagnostic cardiac catheterization.
A 50-year-old female with prior right wrist arthroscopy and residual impairment of supination of the right arm presented with resting chest pain. Electrocardiography was normal. She had no history of peripheral arterial disease or any predisposing condition to thromboembolic events. Exercise stress echocardiography produced exercise-induced chest pain and showed exercise-induced wall motion abnormalities suggesting ischemia in the mid anterior wall.
Investigations
Coronary angiogram was performed using left radial access because of her prior right wrist surgery. The modified Seldinger technique with a 21g needle was used to access the left radial artery and a 6 French 25 cm Glidesheath hydrophilic coated sheath (Terumo, Elkton, MD) was placed without difficulty. Heparin 5000u IV (equivalent to 62 IU/kg) was given. Judkins Left 3.5 and right 4 5 French catheters were used to engage the coronary arteries, all of which were angiographically normal. Procedure time was 32 minutes and fluoroscopy time was 6.5 minutes. No radial artery spasm was noted throughout the procedure. Post procedure patent hemostasis was achieved using the TR band.
The differential diagnosis included coronary artery disease, false positive stress test, prinzmetal’s angina, non-cardiac chest pain such as stress or anxiety induced, costochondritis, GERD.
Treatment
Within an hour post coronary angiography, she developed left arm pain not relieved with Tylenol and ibuprofen. Examination showed the hand was warm and well-perfused and the radial pulse was intact. She was admitted overnight for observation and pain control. At discharge the next day she had mild swelling and tenderness to palpation proximal to radial access site with no hematoma. The arm was noted to be warm and well-perfused, but pulses were not recorded and duplex ultrasound was not performed.
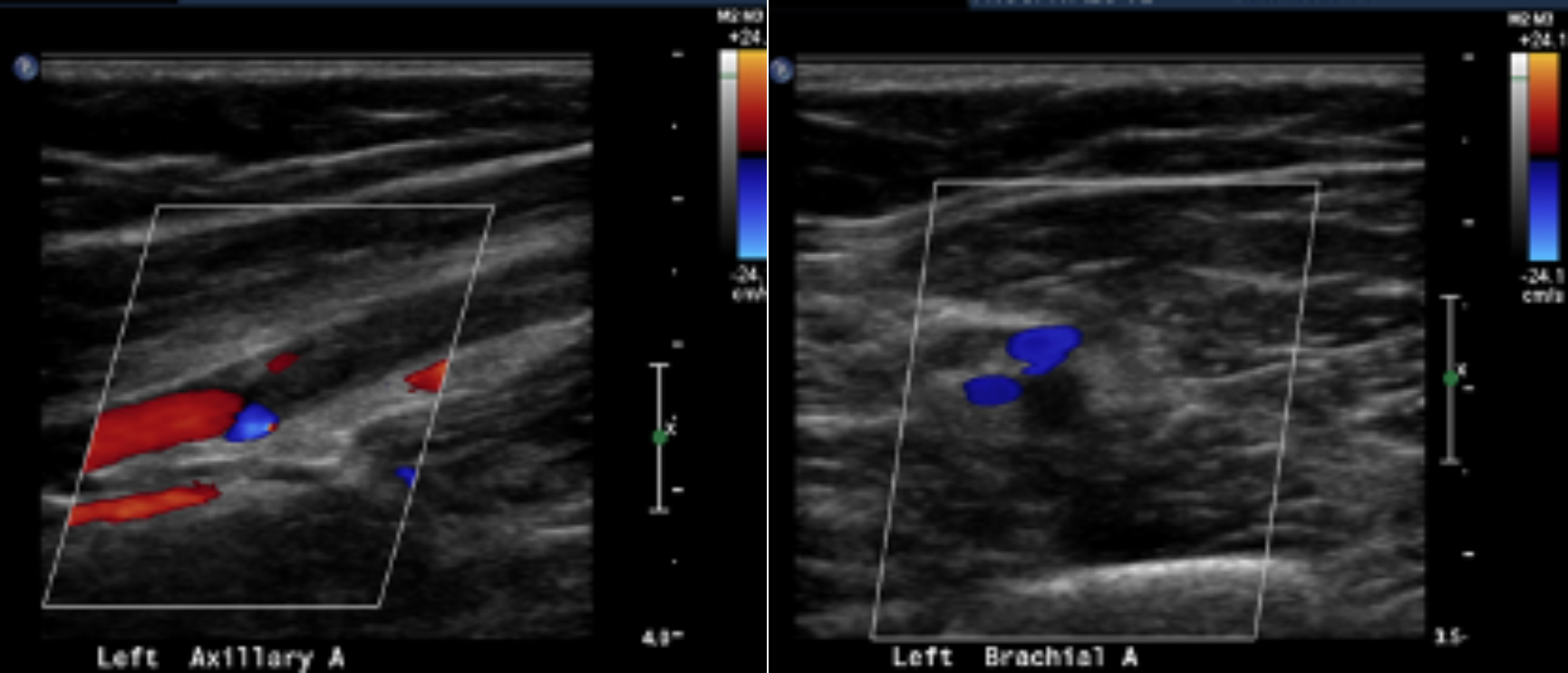
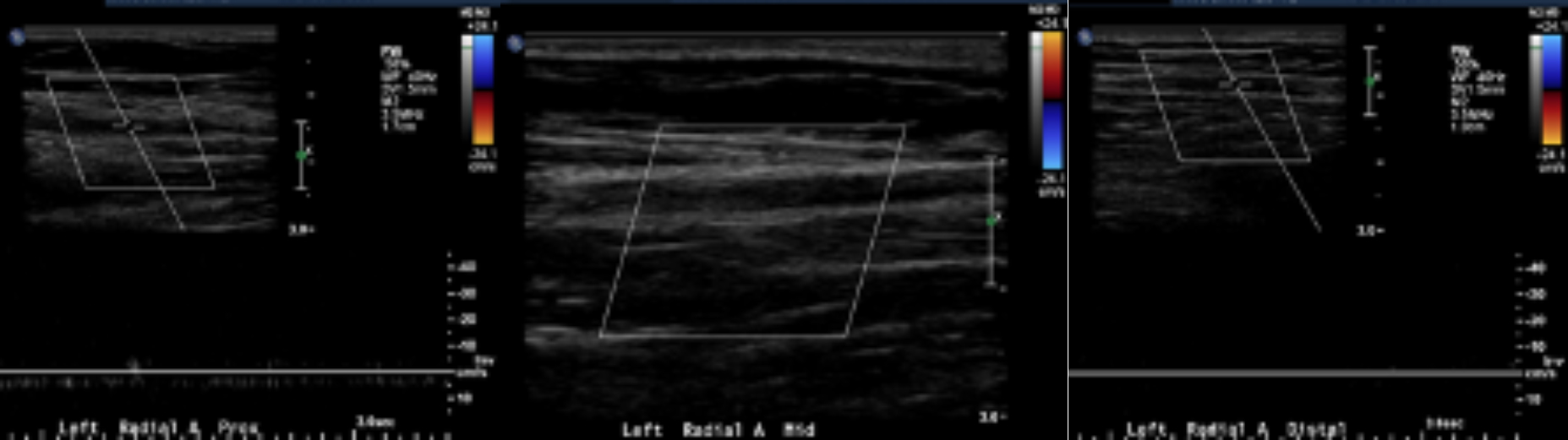
Four days after discharge, she returned with left arm pain and her hand was cold to touch. An upper extremity arterial duplex ultrasound showed thrombosed axillary, brachial, radial arteries with patent ulnar and subclavian arteries (Figures 1,2). Computed tomographic angiography of the chest and upper extremity showed long segment left brachial artery and radial artery occlusions. There was preserved flow to the hand through the ulnar artery and collaterals. She was started on intravenous heparin and on the next day, she underwent successful left axillary, brachial, and radial artery surgical thrombectomy. She was discharged home on warfarin with target INR of 2-3 and aspirin 81mg daily. At that time, she had palpable brachial, radial and ulnar pulses and intact sensation.
At a clinic visit 1 week later, the left hand was noted to be warm and well-perfused with good ulnar and brachial pulses. Upper extremity arterial duplex ultrasound showed thrombosed mid-distal radial artery with other arteries patent. Upper extremity arterial duplex ultrasound at 1- and 3-months post-procedure showed left mid-distal radial artery occlusion and widely patent left subclavian, axillar, brachial and ulnar arteries. Warfarin was discontinued 6 weeks after surgery and she was maintained on aspirin. Three months after the surgery she had some tenderness to palpation of her upper arm and forearm with palpable brachial and ulnar pulses and non-palpable radial pulse. Residual diffuse arm discomfort was attributed by the vascular surgeon to ischemic nerve damage.
Discussion
To our knowledge this is the first reported case of axillary thrombosis after transradial access. Only 1 case of brachial thrombosis after radial access has been reported [3].
Radial artery occlusion is usually caused by thrombus formation from intimal injury. Risk factors for radial artery occlusion include prolonged cannulation times, repeated cannulations, larger introducer sheath size, decreased ratio of arterial diameter to sheath, lower heparin doses, radial artery spasm, and prolonged occlusive hemostasis [3].
Our patient was relatively healthy and had no predisposing factors for arterial thrombosis other than relatively smaller arteries in women compared to men. Left radial access by itself is not associated with a higher incidence of complications [5]. Factors that may have contributed to thrombosis of the radial, brachial and axillary arteries in this patient include [1] use of a 6 French sheath in a female since females have smaller arteries, and smaller arteries with an artery:sheath ratio of < 1>
Radial artery occlusion, when detected immediately after the procedure, can be treated with ulnar artery compression to force flow back into the radial artery [10]. Low molecular weight heparin for 4 weeks increases artery patency up to 86
The authors have no disclosures or conflicts of interest relevant to this paper.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
