
Case Report | DOI: https://doi.org/10.31579/2578-8868/223
1 Department of Neurology, Binzhou Medical University Hospital.
*Corresponding Author: Ruli Ge or Jinbo Chen or Hongcai Wang, PhD, Department of Neurology, Binzhou Medical University Hospital, No. 661, the 2nd Yellow River Road, Binzhou City, 256603, Shandong Province, China.
Citation: Qingqing Zhang, Mengdi Wang, Wenxiang Xu, Zhenghao Shi, He Ma, et all (2022). Atypical Septic Cerebral Embolism in the Fatal Infective Endocarditis. J. Neuroscience and Neurological Surgery. 11(4); DOI:10.31579/2578-8868/223
Copyright: © 2022 Ruli Ge or Jinbo Chen or Hongcai Wang, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 04 January 2022 | Accepted: 26 January 2022 | Published: 01 February 2022
Keywords: infective endocarditis (ie); streptococcus agalactiae (gbs); cerebral embolism; heart failure
Streptococcus agalactiae (GBS) is an unusual cause of infectious endocarditis. At present, evidence suggest that the increasing impact invasive GBS disease occurs on adults. A 51-year old man, had a history of cirrhosis, fundus, esophageal varices, upper gastrointestinal bleeding for 11 years, with spleen resection, fundus and esophageal varices ligation. First clinical feature as right wrist and finger movement dysfunction with low-grade fever was described. Cerebral embolism induced by severe infectious endocarditis was confirmed by MRI+DWI in the early stage. The cardiac color Doppler showed the development of aortic valve vegetation (10 mm x 10 mm), which moved into the aortic sinus in systolic phase and the left ventricular outflow tract, severely affecting hemodynamics. ST-segment depression in the ECG and the elevated serum troponin were indicated. Bacterial isolates from blood cultures revealed that Streptococcus agalactiae (Group B Streptococcus) infection. Despite the infection control and supportive treatment, the patient's condition continued to deteriorate, characterized by intermittent fever, chest pain, sitting breath and coughing up pink and foam sputum. Acute left heart failure was confirmed by echocardiography. The cardiac surgery was complicated and have high risk. The patient eventually died of myocardial infarction and heart failure. Infectious endocarditis should be considered in patients without native valve disease who have cerebral infarction involving anterior and posterior circulation of cerebral artery and prolonged fever. Considering the severity of GBS infection, early recognition and prompt treatment was cardinal importance for the forward prognosis of infectious endocarditis.
Infective endocarditis (IE) is rare but potentially lethal disease, with an incidence of approximately 3 to 9 per 100 000 persons per year in developed countries [1]. Furthermore, left-sided infective endocarditis caused by Streptococcus agalactiae (group B streptococci, GBS) have low probability of occurrence [2]. The most prevalent underlying diseases associated with GBS infection are intravenous drug addiction and valve heart disease. In this paper, we report a rare case of low immunity with irrhosis, fundus, esophageal varices, upper gastrointestinal bleeding acquired Streptococcus agalactiae infection and presented with brain infarction as well as myocardial infarction and heart failure.
A 51-year old man, had a history of cirrhosis, esophageal varices, upper gastrointestinal bleeding for 11 years, with spleen resection, fundus and esophageal varices ligation. He has a history of 30 years of smoking. No family history, no dental visits, no history of use of steroids or immunosuppressive drugs and was not an intravenous drug user.
In the beginning, the patient with high fever 39.0 °C was recognized as influenza virus in community hospital and treated with antivirus medicine. The impaired physical mobility was mild and he did not seek medical attention. He was received antivirus and antibiotics treatment for high fever. After 6 days treatment, the high fever was controlled. But deterioration of right wrist and finger dysfunction leads him to seek medical care. Sustained worsening of the patient's condition indicated that intermittent fever, chest pain, orthopnea and coughing up pink-tinged, foamy sputum. Considering the coronary artery was blocked by the aortic vegetation. Due to the severe complication of heart, the risk of surgery is extremely high. The patient eventually died of severe acute cerebral infarction, myocardial infarction and heart failure.
Admission examination indicated that the patient’s temperature was 38.3 °C, blood pressure was 120/55 mmHg, heart rate was 78 beats per minutes, respiratory rate was 22 breaths per minute, and oxygen saturation was 98% on room air. No obvious bleeding spots or erythema were seen on his skin. The patient had no disturbance of consciousness and meningitis. The state of mind is clear with clumsy speech. The muscle strength of right finger grade 0 and wrist grade 1. The remainder of the neurological exam were normal including normal muscular tension, bilateral Babinski sign (-). Cardiac auscultation indicated that low heart tone and grade 4/6 diastolic murmur of aortic valve.
Blood test: AST 29.3U/L(normal: 29~35 U/L), albumin28.7 g/L(normal: 3~50 g/L), alkaline phosphatase 116.0 U/L(normal: man45~125 U/L), g-glutamyltranspeptidase 73.4 U/L(normal: 3~50 U/L), lactate dehydrogenase 275.4 U/L(normal: 135.0~215.0 U/L), a-hydroxybutyrate dehydrogenase 213.5 U/L(normal:90~182 U/L), LDL 2.71 mmol/L(normal: 2.07~3.37 mmol/L), tumor marker: NSE 16.89ng/ml (normal:<12>
Two days later, AST 51.3 U/L, albumin 29.0 g/L, white blood cell 21.86x10^9/L, neutrophilic granulocyte 19.77x10^9/L, BNP 1374.8 pg/ml, troponin I 2.66 ng/ml.
Bacteria isolation and blood culture: Streptococcus agalactiae (Group B Streptococcus) (GBS) were positive. The procedures were repeated 2 times.
The MRI of the brain showed the increased signal intensity on Diffusion-weighted imaging (DWI) in the left frontal lobe and bilateral cerebellar hemispheres, implying acute lacunar infarction, multiple intracranial arteriosclerosis, and local stenosis of the right cerebral anterior artery A1 segment (Figure.1).

The ultrasonography of carotid artery revealed an increase in blood flow resistance of the left vertebral artery. Cardiac color Doppler showed a moderately strong echo of the aortic valve 10 mm x 10 mm (aortic valve vegetation). The aortic valve vegetation moved into the aortic sinus in systolic phase, and into the left ventricular outflow tract, severely affecting hemodynamics (Figure. 2).
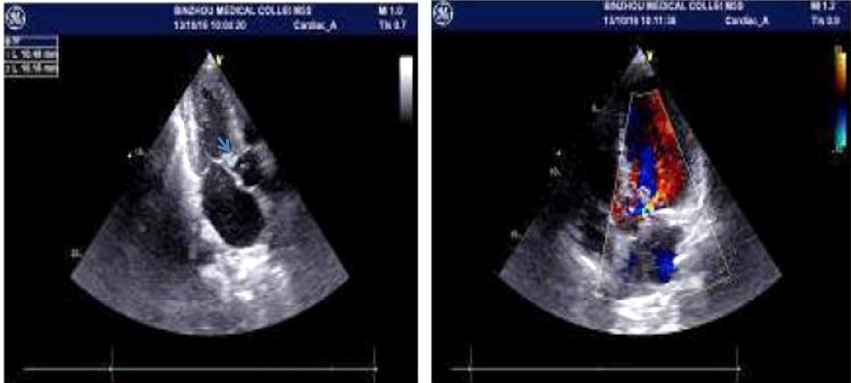
The heart color ultrasound was further confirmed that acute left heart failure occurred. The ECG indicates that the ST segment is significantly depressed, and the serum troponin are elevated.
In this paper presented as a case of severe IE induced by GBS with neurological complications in a patient with an history of cirrhosis, esophageal varices, upper gastrointestinal bleeding. As more evidence suggest that endocarditis is a clinical definable and treatable disease [3]. Despite improvement in the prevention and therapeutic strategies, the fatality rate due to IE has not significantly reduced [3]. The most prevalent underlying diseases associated with IE is devices, congenital heart lesions, underlying native valve disease including rheumatic heart disease, calcific aortic stenosis and mitral valve prolapse. The risk for IE in patients with no previously seen structural changes in the heart is intravenous drug abuse, chronic hemodialysis and central venous access. Young patients tend to have chronic rheumatic heart disease or congenital heart disease and elderly patients are likely to have degenerative valve disease [4]. Although there is no artificial valve or heart disease for this case, the patient has low immunity such as diabetes and cirrhosis. The history of cirrhosis, fundus, esophageal varices, upper gastrointestinal bleeding revealed that the low immunity exist.
The patient's bacterial blood culture was positive for the second time as Streptococcus agalactiae. Left-sided infective endocarditis caused by Streptococcus agalactiae is rare and serious [2]. Streptococcus agalactiae frequently affects patients with debilitating diseases and was involved in native valves. It is charactered by a rapid clinical worsening and severe valve destruction, and high mortality has been reported [5-7]. The condition of patients worsened significantly due to the infection of Streptococcus agalactiae.
Streptococcus agalactiae often occurs in chronic diseases with immunosuppressive conditions, such as diabetes mellitus, alcoholism, pregnancy, intravenous drug abuse, and genitourinary disease [5]. Streptococcus agalactiae still have a high mortality rate, although the prognosis of infective endocarditis has improved significantly with the development of cardiac surgery [6]. Although GBS induced left-sided IE is much less frequent than Staphylococcus aureus left-sided IE, GBS infective endocarditis represented less than 3% of all IE cases throughout the years. GBS has similarly aggressive and onset as Staphylococcus aureus. Both present with acute fever, but GBS is not accompanied by skin lesions. It usually develops serious complications and a heart surgery is frequently required during the admission. Despite its easy medical treatment and the performance of early surgery, it has high mortality [2]. Thus, early recognition and treatment for GBS carried great weight.
There are four main factors that influence the prognosis of infective endocarditis: patient characteristics, presence or absence of cardiogenic or non-cardiac complications, infected microbes, and echocardiographic findings. Echocardiography is central to the diagnosis and helpful for the management of patients with IE. Echocardiographic evidence of an oscillating intracardiac mass or vegetation, an annular abscess, prosthetic valve partial dehiscence, and new valvular regurgitation are major criteria in the diagnosis of IE. Several echocardiographic features suggest patients at high risk for a complicated course or with a need for surgery. These features include large (>10 mm in diameter) vegetations, severe valvular insufficiency, abscess cavities or pseudoaneurysms, valvular perforation or dehiscence, and evidence of decompensated heart failure [8]. The greatest risk of embolic complications appears to occur with large (≥10 mm) vegetations on the anterior mitral leaflet [9]. Left-sided IE is always associated with stroke onset [9]. The aortic valve vegetation induced the cerebral embolism. As everyone known that embolism is one of the most severe complications of IE, and it is accepted as one of major determinants of prognosis increasing mortality. Embolism usually occurs in the first two weeks after the diagnosis of IE [11-12]. Surgical treatment is urgent to do because vegetation of >1 cm in left-sided IE is associated with higher mortality [13]. In this case, vegetation was >1 cm, the aortic valve vegetation moved into the aortic sinus in systolic phase, and into the left ventricular outflow tract, severely affecting hemodynamics.
The low resistance and tolerance to infection in patient prone to GBS infection with high mortality, suggesting a poor prognosis. Early surgery (during initial hospitalization and before completion of a full course of antibiotics) is indicated in patients with IE who present with mobile vegetations >10 mm and valve dysfunction resulting in symptoms or signs of heart failure. Because and high risk for surgery and the family members of the patients refused surgical treatment, the patient eventually died of severe acute cerebral infarction, myocardial infarction and heart failure [14].
This work was supported by grants from the National Natural Science Foundation of China (NSFC) (81601108), Natural Science Foundation of Shandong Province of China (ZR2016HQ14).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
