
Research Article | DOI: https://doi.org/10.31579/2690-8808/151
1 Department of Obstetrics and Gynaeology, Ahmad Sanni Yariman Bakura Specialist Hospital, Gusau, Zamfara State.
2 Department of Obstetrics and Gynaecology, Federal Medical Centre, Gusau, Zamfara State.
*Corresponding Author: Oyaromade A, Nurse. Department of Obstetrics and Gynaeology, Ahmad Sanni Yariman Bakura Specialist Hospital, Gusau, Zamfara State.
Citation: Oyaromade A, Fasanu O T, Usman M S, Isah M B, Ekele O I, Egwuete C O and, Mohammed B A (2023). Mate Selection by Gender Role Journal of Clinical Case Reports and Studies 4(1); DOI: 10.31579/2690-8808/151
Copyright: © 2023 Oyaromade A, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 November 2022 | Accepted: 28 December 2022 | Published: 06 January 2023
Keywords:
Rupture of the pregnant uterus refers to complete disruption of all uterine layers, including the serosa [1]. It is an Obstetric catastrophe associated with high maternal and perinatal morbidity and mortality [2]. It is a common complication in the developing countries due to poor obstetric care, low socioeconomic status, ignorance and adverse sociocultural practices, beliefs and aversion for Caesarean section [2].
We are reporting a case of spontaneous uterine rupture following a spontaneous vaginal delivery that was managed at the department of Obstetrics and Gynaecology, Ahmad Sanni Yariman Bakura Specialist Hospital, Gusau, Zamfara state, Nigeria.
Mrs A. A, a 25-year-old unbooked P4+0(2 alive) who had an unsupervised home delivery of a fresh male stillborn 9 days prior to presentation. She presented to the Obstetric emergency with lower abdominal pain of 9 days, fever, headache and diarrhoea of 8 days, no excessive vaginal bleeding. On examination, she was ill-looking, Temperature was 39.3°C, Pulse rate was 89bpm, BP- 120/90mmHg, there was generalized abdominal tenderness and she had normal lochia on vaginal examination. PCV was 32%. Ultrasound showed that pelvic organs were within normal limits but there was increased peritoneal fluid. She was admitted for puerperal sepsis and placed on parenteral antibiotics and analgesics.
1 day into admission, she was reviewed, she was still having abdominal pain and fever, on examination she was not pale, she had tinge of jaundice, pulse rate was 86bpm, BP- 120/90mmHg, abdomen was tender, uterus was difficult to palpate, percussion note was dull. The cervix was 6cm dilated. Ultrasound scan and PCV was to be repeated.
Day 2 into admission, she was still having fever, abdominal distention and pain. The repeat ultrasound scan showed a bulky uterus and a discontinuation in the lower part of the posterior wall of the uterus with massive peritoneal fluid, repeat PCV was 31%. On examination, she was not pale, had a tinge of jaundice, temperature was 38.0°C, pulse rate was 116bpm, BP- 110/80mmHg, there was generalized abdominal tenderness. On peritoneal tapping altered blood was obtained.
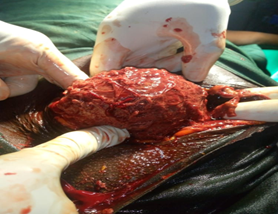
Figure 1
She subsequently had an emergency exploratory laparotomy with a midline sub-umbilical incision. Findings were massive haemoperitoneum of 2 litres, bulky uterus with left posterolateral rupture from the isthmus to the left cornu, gangrenous left fallopian tube and ovary, cheesy omental cake covering the uterus and the intra-abdominal organs. She had a total abdominal hysterectomy, left salpingo-oophorectomy and peritoneal toileting with a drain. She had 500mls of whole blood transfused intra-operatively. She was placed on antibiotics, IV fluids and analgesics. Drained was removed 2 days post op when it was no longer active. She did remarkably well and was discharged 1-week post op in good health condition.
Uterine rupture is an uncommon complication of pregnancy, it's prevalence varies from one region and country to another [3]. It is rare in developed countries, however, it is a menace to developing countries especially in Africa where studies put the range between 0.3-2.4% [3-8].
In the developing countries, majority of cases of uterine rupture occur following prolonged obstructed labour whereas in developed countries, it occurs more often with a history of previous uterine surgeries [4,9]. Other risk factors for uterine rupture are, injudicious uterotonic use[3], grand multiparity, macrosomia [10,11], abnormal placention [12,13], and drug abuse [14,15]. However, none of these was identified in the patient presented.
Though majority of cases of uterine ruptures are diagnosed in the intrapartum period, only a few cases are diagnosed in the postpartum period [16]. Also, most patients present with the typical features of sudden abdominal pain, vaginal bleeding, deranged maternal vital signs and fetal heart rate abnormality or death, but a few cases do not present this way [17]. In the case presented above, the patient presented 9 days after a spontaneous vaginal delivery, she had no vaginal bleeding nor any haemodynamic instability, this contributed to the delay in making the diagnosis of a uterine rupture.
Due to the rare occurrence and the atypical presentation of lower abdominal pain, fever, headache and diarrhoea, and findings of normal vital signs with no vaginal bleeding our primary diagnosis was puerperal sepsis. Ultrasound scan showing massive intraperitoneal fluid and a peritoneal tap yielding altered blood subsequently raised the diagnosis of a uterine rupture.
The pathogenesis of the rupture was not known, however with the practice of fundal pressure being very common in our environment [18], she might have sustained the uterine rupture in the second stage of labour on account of fundal pressure, this was probably the reason she subsequently progressed to a spontaneous vaginal delivery of a fresh still birth. A similar case was reported in Taiwan [19]. It is however unclear why she had neither vaginal bleeding nor haemodynamic instability despite massive haemoperitoneum later detected on emergency laparotomy.
Most cases of uterine rupture could be prevented with good antenatal care, birth preparedness and complication readiness, early recognition of obstructed labour, close monitoring of interventions known to have increased risk of uterine rupture [20]. Prompt diagnosis and treatment would prevent the accompanying morbidity and/or mortality.
In conclusion, uterine rupture is an uncommon complication of pregnancy with high maternal and perinatal morbidity and mortality. They may present with unusual signs and symptoms making it tough to diagnose with history and physical examinations only. However, there should be a high index of suspicion of uterine rupture in a pregnant woman or in the puerperium with severe generalized abdominal with or without vaginal bleeding.
None.
None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
