
Case Report | DOI: https://doi.org/10.31579/2641-0419/268
1 Ohio State University Wexner Medical Center, Department of Internal Medicine.
2 Ohio State University Wexner Medical Center, Division of Gastroenterology, Hepatology & Nutrition.
3 Ohio State University Wexner Medical Center, Division of Vascular Interventional Radiology.
4 Ohio State University Wexner Medical Center, Division of Surgical Oncology.
5 Ohio State University Wexner Medical Center, Department of Cardiovascular Disease, Pulmonary Vascular Disease Program, Advanced Heart Failure & Transplant Program.
6 Ohio State University Wexner Medical Center, Division of Interventional Radiology.
7 Hio State University Wexner Medical Center, Division of Pulmonary, Critical Care and Sleep Medicine.
*Corresponding Author: Kevin Litzenberg, Ohio State University Wexner Medical Center, Department of Internal Medicine.
Citation: Kevin Litzenberg, Khalid Mumtaz, Gavisha Waidyaratne, Ahmad Anaizi, Mamdouh Khayat., et all (2022). Atypical Presentation of Isolated Gastric Variceal Bleeding Requiring Multidisciplinary Management. J. Clinical Cardiology and Cardiovascular Interventions, 5(6); DOI:10.31579/2641-0419/268
Copyright: © 2022 Kevin Litzenberg, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 April 2022 | Accepted: 30 May 2022 | Published: 06 June 2022
Keywords: gastric varices; non-cirrhotic portal hypertension; splenic injury
Variceal bleeding is the most lethal manifestation of portal hypertension, most commonly due to esophageal varices in the setting of liver cirrhosis. Isolated gastric varices (IGV) are a rare cause of upper gastrointestinal bleeding, often of pancreatic origin. In this case we present a complex patient with a history of remote splenic injury leading to portopulmonary hypertension and the development of refractory bleeding due to IGV. We discuss the extensive multidisciplinary approach taken to provide comprehensive care and to control bleeding, which included endoscopic (sclerotherapy), radiologic (balloon-occluded antegrade transvenous obliteration [BATO] and splenic artery embolization) and surgical interventions (splenectomy).
IGV are observed in up to 5% of patients with liver cirrhosis, and up to 10% of patients with non-cirrhotic portal hypertension (NCPH) [1,2]. If a branch of the portal venous system becomes obstructed, such varices can form in order to decompress the segment [2]. Although gastric varices are 50% less likely to bleed compared to oroesophageal varices, bleeding from gastric varices is more severe [1,3]. Studies have shown that gastric variceal bleeding have a significantly higher mean blood transfusion requirement [1]. Gastric variceal bleeds also portend a higher mortality risk than esophageal varices with some studies reporting mortality as high as 45% [1,4]. Management of initial bleeding of IGV presents a challenging problem since information about the etiology may not be available at the time of initial presentation. While cirrhosis is the most common cause of portal hypertension, there are numerous causes of NCPH which can be classified by the location of resistance to blood flow into prehepatic, hepatic, and post hepatic groups [5]. We present a rare case of refractory bleeding from IGV in a patient with NCPH due to remote splenic injury.
A 40-year-old woman with a history of remote splenic injury due to a motor vehicle accident during infancy was admitted with one episode of large hematemesis. On arrival, vital signs were unstable (blood pressure to 80/50 mmHg and tachycardia of 130/min) and initial hemoglobin was 11.7 g/dl. She was resuscitated with normal saline and started on intravenous pantoprazole. She was intubated and transferred to the intensive care unit for an urgent esophagogastroduodenoscopy (EGD), which demonstrated IGV with a large nipple sign and no active bleeding [Figure 1].

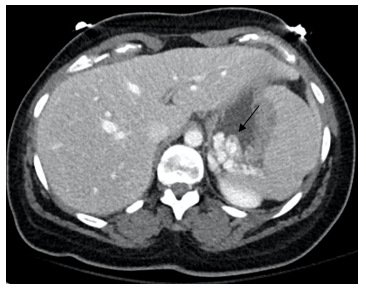
No endoscopic intervention was performed given the unknown etiology of IGV and inactive bleed. Abdominal CT scan revealed splenomegaly and confirmed prominent gastric varices without a discrete gastro-renal
shunt; there was no evidence of splenic vein stricture or thrombosis on imaging [Figure 2].
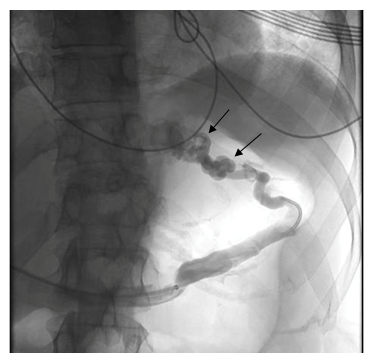
Transthoracic echocardiogram (TTE) showed moderate diastolic dysfunction and was suggestive of pulmonary hypertension with elevated right ventricular systolic pressure (RVSP). Percutaneous transhepatic obliteration of IGV with coil embolization was performed by Interventional Radiology [Figure 3]. On post-op day one, a repeat episode of hematemesis prompted follow-up EGD and sclerotherapy with N-Butyl Cyanoacrylate (NBC). She was discharged home four days later.
One day after discharge on post-op day six, the patient again presented to our facility after another episode of hematemesis. After initial resuscitation, right heart catheterization confirmed pulmonary hypertension with a pulmonary artery (PA) systolic pressure of 67 mmHg (normal 15-25 mmHg), mean PA pressure of 41 mmHg (normal <24>
Ultimately, the patient underwent partial splenic artery embolization followed by total splenectomy as a definitive therapy. She tolerated splenectomy well. On post-surgical inspection, her spleen measured 19.4 cm (normal: 11 cm) in the greatest dimension and weighed 777 grams (normal is up to 150 grams). For her pulmonary hypertension she was started on epoprostenol infusion and then transitioned to oral riociguat and macitentan. Two months later, she was doing well with no further episodes of bleeding.
We present, to our knowledge, the first case of splenic injury resulting in bleeding IGV from NCPH, a case which was a diagnostic puzzle in which the patient experienced four life-threatening bleeding episodes before curative multidisciplinary management.
In recent years better understanding of the physiology of the portal venous system has improved management of bleeding IGV. Studies have demonstrated that almost half of IGV are secondary to abnormalities of the pancreas [6]. Classically, patients have imaging suggestive of splenomegaly and/or splenic vein thrombosis. Lin et al describe a patient with GV bleeding due to splenic vein occlusion arising from abdominal lymphadenopathy [7]. Similarly, mass effect from lymphomas, abscesses, or tumors of the pancreas, stomach, colon or kidney may cause splenic vein stenosis or thrombosis with resultant GV bleeding [2, 8]. Another case has described IGV resulting from abdominal tuberculosis [9].
Sclerotherapy of IGV with NBC is the optimal endoscopic intervention, supported by evidence-based guidelines, and routinely performed, though not approved for this purpose in the United States. Radiological interventions for managing IGV include TIPS, balloon-assisted antegrade or retrograde transvenous obliteration (BATO or BRTO), and partial splenic artery embolization [10]. For patients with IGV bleeds related to portal hypertension, TIPS directly reduces portal pressures, portending significant survival benefit [10]. BATO/BRTO is indicated for those in whom TIPS fails or is contraindicated. Transvenous obliteration of IGV entails systemic venous access with subsequent injection of a sclerosing agent and/or embolization of the culprit varix. Blood flow is diverted toward the portal circulation, and unlike a TIPS procedure, does not reduce portal pressures [10,11]. Alternative therapies for patients with IGV include partial splenic artery embolization or splenectomy to mitigate portal hypertension and its associated physiological effects. Partial splenic artery embolization is a safe and effective adjunctive consideration to address bleeding IGV, particularly in patients who cannot immediately undergo splenectomy or may not be good surgical candidates [9]. Surgical splenectomy can be pursued for more definitive therapy.
Our patient had large IGV, a normal pancreas, minimal hepatic fibrosis, a normal HVPG and pulmonary hypertension. Her marked splenomegaly from a remote splenic injury led to the development of presinusoidal portal hypertension followed by pulmonary hypertension and ultimately, refractory IGV bleeding. Portopulmonary hypertension is a well-established sequela of cirrhosis; however, it was recently described in patients with non-cirrhotic portal hypertension (NCPH) as in our case [12]. The underlying pathogenesis remains largely obscure. In patients with NCPH, vasoactive substances such as endothelins have been hypothesized to result in vascular remodeling, leading to increased pulmonary pressures. Decreased production of vasodilators, including nitric oxide and prostaglandins, will contribute to elevated pulmonary pressures as well. Another proposed mechanism is that established portosystemic shunts help to deliver these vasoactive substances directly into the pulmonary circulation, expediting pathologic changes. Portopulmonary hypertension leads to stress on the right ventricle, and prognosis is highly correlated with the degree of subsequent right ventricular dysfunction [12].
In order to serve our patient, the expertise of numerous disciplines was required. This unique case illustrates the challenges of managing gastric varices in a patient without cirrhosis caused by remote splenic injury and the need for a multidisciplinary approach to ensure the best outcome [13].
In conclusion, we present the unique case of a patient whose remote splenic injury led to the development of NCPH followed by pulmonary hypertension and refractory bleeding from IGV. While most IGV are caused by pancreatic abnormalities, there are multiple other etiologies including malignancy, abscess, and trauma leading to splenic vein stenosis or thrombosis. While sclerotherapy of IGV with NBC is considered optimal endoscopic therapy, there are variable options for refractory IGV including radiologic and surgical interventions. For such an unusual case of IGV without cirrhosis, we therefore recommend a multidisciplinary approach to patient care.
Our authors have no conflicts of interest to disclose.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
