
case report | DOI: https://doi.org/10.31579/2692-9392/106
Department of Cardiology, Royal Free Hospital, Royal Free NHS Foundation Trust, London, UK.
*Corresponding Author: Adam Ioannou, Department of Cardiology, Royal Free Hospital, Royal Free NHS Foundation Trust, London, UK.
Citation: Adam Ioannou, (2022) Atrial Fibrillation with Ventricular Pre-Excitation: A Diagnosis That Must Not Be Missed. J. Archives of Medical Case Reports and Case Study, 5(4); DOI:10.31579/2692-9392/106
Copyright: © 2022 Adam Ioannou, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 January 2022 | Accepted: 30 March 2022 | Published: 08 April 2022
Keywords: wolff-parkinson-white; haemodynamic; atrial fibrillation
Wolff-Parkinson-White (WPW) syndrome is caused by an accessory pathway that communicates between the atria and ventricles known as the Bundle of Kent. The development of atrial fibrillation, can result in the atrial impulses all being conducted via the accessory pathway and result in a sinister, board complex, irregular tachycardia, with varying QRS morphology (known as pre-excited atrial fibrillation) Adenosine is a potent atrioventricular node blocker, which can be used in the treatment of supraventricular tachycardias, but also has diagnostic utility, particularly in differentiating between supraventricular tachycardia with aberrant conduction (which would often terminate) and a ventricular tachycardia (which would not respond to adenosine). However, the administration of adenosine in pre-excited atrial fibrillation can precipitate 1:1 atrial to ventricular conduction, which can degenerate into life-threatening ventricular arrythmias. This case describes a patient who presented with pre-excited atrial fibrillation and received intravenous adenosine that resulted in development of broad complex tachycardia with haemodynamic compromise. In patients with pre-exited atrial fibrillation, AV nodal blocking agents should be avoided and direct current cardioversion should be utilised.
Wolff-Parkinson-White (WPW) syndrome is caused by an accessory pathway that communicates between the atria and ventricles known as the Bundle of Kent. The development of atrial fibrillation, can result in the atrial impulses all being conducted via the accessory pathway and result in a sinister, board complex, irregular tachycardia, with varying QRS morphology (known as pre-excited atrial fibrillation).[1] This case describes a patient in whom this diagnosis was not initially recognised and the administration of intravenous adenosine precipitated a broad complex tachycardia with haemodynamic compromise.
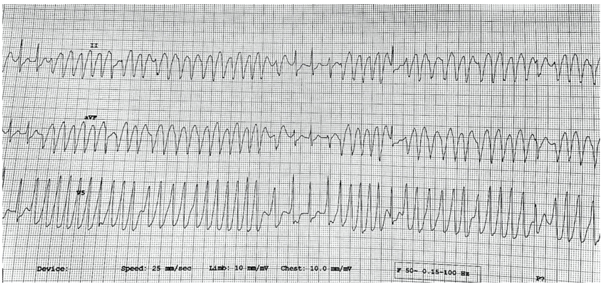
A young male who was previously fit and well presented to hospital due to palpitations. These began gradually and worsened over the preceding hour. On arrival he still had palpitations, but did not report any chest pain, shortness of breath or dizziness. He denied having any other medical conditions, any family history of cardiac disease or sudden unexplained death, and denied recreational drug use. Clinical examination was unremarkable apart from a resting tachycardia (167 bpm) and his blood pressure was normal (132/75 mmHg). The rhythm strip of his electrocardiogram (ECG) demonstrated an irregular broad complex tachycardia, with variable QRS morphology (Figure 1).
Following the initial assessment he was given 6mg of intravenous adenosine in order to differentiate whether this tachyarrhythmia was related to a supraventricular tachycardia with aberrant conduction or a ventricular tachycardia. On administration of the adenosine he became lightheaded, his heart rate rapidly increased to 220 bpm and his blood pressure decreased to 94/63 mmHg. The cardiac monitor showed a rapid regular broad complex tachycardia. He subsequently underwent immediate direct current (DC)
cardioversion with a single biphasic synchronised shock of 200J. This successfully cardioverted the patient into sinus rhythm. His resting 12-lead ECG demonstrated a short PR interval of 100 msec, narrow QRS complexes (111 msec) and a delta wave, which was most prominent in the inferior leads (Figure 2). In view of the ECG findings he was diagnosed with Wolff-Parkinson-White (WPW) syndrome.

His initial blood tests including a serum troponin revealed normal biochemistry and haematology. Transthoracic echocardiography demonstrated normal biventricular size and function and no valvular abnormalities.
He was admitted to the coronary care unit and the next day underwent an electrophysiology study followed by definitive treatment with an ablation of the accessory pathway. He made an uneventful recovery and was discharged 24-hours later.
PW is caused by an accessory pathway that communicates between the atria and ventricles known as the Bundle of Kent.[1] The accessory pathway does not share the rate limiting properties of the atrioventricular (AV) node and can conduct electrical activity at a much faster rate. If patients with WPW develop atrial fibrillation, the atrial impulses can all be conducted via the accessory pathway and result in a rapid heart rate with haemodynamic instability. Pharmacological agents that block the AV node (such as adenosine, beta-blockers and non-dihydropyridine calcium channel blockers) are contraindicated as they may exacerbate the syndrome by blocking the normal conduction pathway, and favouring 1:1 atrial to ventricular conduction via the accessory pathway.[2] This leads to a sinister, broad complex, irregular tachycardia which can degenerate into ventricular arrhythmias. Such patients should be treated in the acute setting with DC cardioversion and then have definitive treatment with an ablation of the accessory pathway.[3]
Intravenous adenosine is a potent AV node blocker with a short half-life, and has become the first line pharmacological agent in the treatment of supraventricular tachycardias. It often causes rapid termination of arrythmias that utilise the AV node. Adenosine can also be used as a diagnostic tool when the underlying arrhythmic mechanism is unclear. Atrial arrythmias, such as atrial flutter, do not terminate on the administration of adenosine but unmasking the atrial rhythm by temporarily blocking the AV node can be diagnostically beneficial.[4]
In patients presenting with a broad complex tachycardia, adenosine administration can be used to differentiate between a supraventricular tachycardia with aberrant conduction (which would often terminate) and a ventricular tachycardia (which would not respond to adenosine). This differentiation is extremely important as it has both short and long-term implications on subsequent patient investigations, treatment and prognosis. [5-8]
However, an important caveat to consider is that if the broad complex tachycardia is indeed a pre-excited atrial fibrillation, the administration of adenosine carries the risk of precipitating 1:1 atrial to ventricular conduction, which can degenerate into life-threatening ventricular arrythmias. Pre-excited atrial fibrillation often occurs in young otherwise healthy patients, and causes a rapid, board complex, irregular tachycardia, with variable QRS morphology. In the acute setting, AV nodal blocking agents should be avoided and DC cardioversion should be utilised.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
