
Research Article | DOI: https://doi.org/10.31579/2578-8868/200
1Department of Neurology, Shengli Oilfiled Central Hospital, 31 Jinan Road, Dongying, Shandong, China. 257000.
2Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, 110 W. South 4th Ring Road, Fengtai, Beijing, China. 100070.
*Corresponding Author: Shimeng Liu, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, 110 W. South 4th Ring Road, Fengtai, Beijing, China. 100070.
Citation: Tianping Tang., Ligong Zhang., Xingquan Zhao., Shimeng Liu. (2021) Associations between Intensive Lipid-lowering Therapy and Outcomes of Intracerebral Hemorrhage. J. Neuroscience and Neurological Surgery. 9(3); DOI:10.31579/2578-8868/200
Copyright: © 2021 Shimeng Liu, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 22 July 2021 | Accepted: 29 July 2021 | Published: 05 August 2021
Keywords: intensive lipid lowering therapy; intracerebral hemorrhage; low-density cholesterol lipoprotein; outcomes
Background: The intensive lipid-lowering therapy (ILLT), targeting an low-density lipoprotein cholesterol (LDL-C) < 1.80 mmol/L, was a crucial strategy for the secondary prevention of cerebrovascular diseases. But the associations between ILLT and the outcomes after intracerebral hemorrhage (ICH) were unclear.
Materials and Methods: Data of the consecutive patients with acute ICH and past medical histories of ischemic stroke from 2017 to 2019 at an academic stroke center in China were analyzed. The study patients were classified according to their baseline LDL-C levels: < 1.80 mmol/Lvs. ≥ 1.80 mmol/L. The outcomes of ICH were compared between the two groups. Multivariate linear mixed effect model with repeated measures adjusting for ICH scores were used to determine the associations between LDL-C levels and the change in NIHSS scores; baseline ICH scores were adjusted in the multi-variable models
Results: A total of 197 patients were included in the study, 31 of them had LDL-C < 1.80 mmol/L and 166 had LDL-C ≥ 1.80 mmol/L. We did not test any significant differences regarding the demographic characteristics or vascular risk factors. Medians of the baseline National Institutes of Health Stroke Scale (NIHSS) scores (8 vs. 9, P = 0.79) and ICH scores (1 vs.1, P = 0.26) were similar. But the patients with LDL-C < 1.80 mmol/L had higher risks of secondary intraventricular hemorrhage (13% vs. 4%, P = 0.03). Outcomes of the hemorrhagic stroke at discharge were similar, except the patients with LDL-C ≥ 1.80 mmol/L had significant improvements in their NIHSS scores at discharge (estimated change in means: -2.4, 95% CI: [-4.3, -0.5]), while patients with LDL-C < 1.80 mmol/L did not (estimated change in means: -1.4, 95% CI: [-5.9, 3.0]).
Conclusion: ILLT achieved LDL-C < 1.80 mmol/L was associated with limited improvements in the neurological deficits in the patients with ICH.
Serum low-density lipoprotein cholesterol (LDL-C) was identified as an independent risk factor of ischemic stroke.[1] The use of the 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor (statin) class of drugs, reduces serum LDL-C by 55% to 60% at the maximal doses. Our prior study found achieving LDL-C < 1>
Spontaneous, nontraumatic ICH is a significant cause of morbidity and mortality, ranking the second subtype of stroke.[3, 4] The mortality rate of ICH was reported to be 40% at 1 month and 54% at 1 year, only 12-39% of the survivors achieved long-term functional independence.[4] Risk factors of ICH included advanced age, hypertension, current smoking, excessive alcohol consumption, hypocholesterolemia.[4] Blood pressure managements, intensive care, glucose managements, surgery intervention was the standard managements of ICH.[3]
When balancing the benefits of ILLT for the prevention of ischemic stroke and the increased risks of ICH, the current evidence was controversial. In a cumulative meta-analysis of lipid-lowering trials reported the events of ICH, 9.17 (95% confidence interval [CI]:[5.78, 12.66]) fewer ischemic strokes and 0.41 (95% CI: [0.05, 0.86] more ICH per 1000 person-years were estimated.[5] Based on the French population cohort in the Treat Stroke to Target trial (n = 1073) , after an ischemic stroke of documented atherosclerotic origin, lipid-lowering therapy targeting an LDL-C < 1 xss=removed xss=removed>
Evidence from the studies to investigate the associations between the serum LDL-C concentrations and the prognosis of ICH was even less. In a retrospective study of the patients with acute ICH (n = 672), higher admission LDL-C concentrations were independently associated with decreased risks of hematoma expansion (OR: 0.88, 95% CI: [0.77, 0.99]; P = 0.048) and lower likelihood of in-hospital death (OR increased by 0.68 per 0.3 mmol/L decreased in LDL-C, 95% CI: [0.57, 0.80]; P < 0 xss=removed xss=removed>
Due the current limited studies, we carried the retrospective cohort study to explore the associations between the ILLT in the secondary stroke prevention settings and the outcomes of ICH.
We retrospectively analyzed the data of the consecutive patients with acute ICH at a comprehensive stroke center in China from 2017 to 2019. The inclusion criteria were: (1) ≥ 18 years old; (2) with the admission diagnosis of spontaneous ICH; (3) symptoms onset within 7 days; (4) with the past medical histories of ischemic stroke.[11] We excluded the patients with the etiology of vascular malformations.[11] Diagnosis and stroke subtypes were determined based on clinical features, brain imaging and angiography.[11] The study was approved by the institutional review board (IRB).
The study patients were stratified according to their baseline serum LDL-C concentrations: <1>
The scores of National Institute of Health Stroke Scale (NIHSS) and Glasgow Coma Scale (GCS) were recorded in the emergent room to evaluate the baseline severity of the indexed events. [11] ICH scale was used to assess the severity of the ICH events. The modified Rankin Scales (mRS) were tested at discharge to evaluate the prognosis of the hemorrhagic events. An mRS score > 3 was defined as unfavorable outcomes. The ICH scale was ranged from 0 to 6, with higher scores indicating higher risks of ICH.[13]
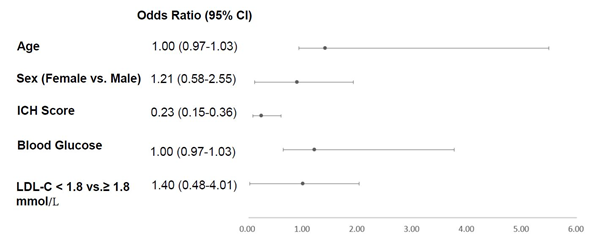
Data analysis first compared distributions of sex, age, vascular risk factors, medication history and results of blood work between the two groups (LDL-C: < 1>
Multivariate linear mixed effect models with repeated measures adjusting for ICH scores were used to determine the associations between LDL-C levels and the change in NIHSS scores; baseline ICH scores were adjusted in the multi-variable models
The SAS statistical package (version 9.4; SAS Institute, Cary, NC, USA) was used to perform data analysis.
Study patients
A total of 197 patients were included in the study. They were 131 men and 68 women. The median age of the study patients were 65 years. In the entire study cohort, 180 (91%) patients had mRS scores less than 3 ahead of the hemorrhagic events, and 161 (82%) had been taking statin (Table 1).
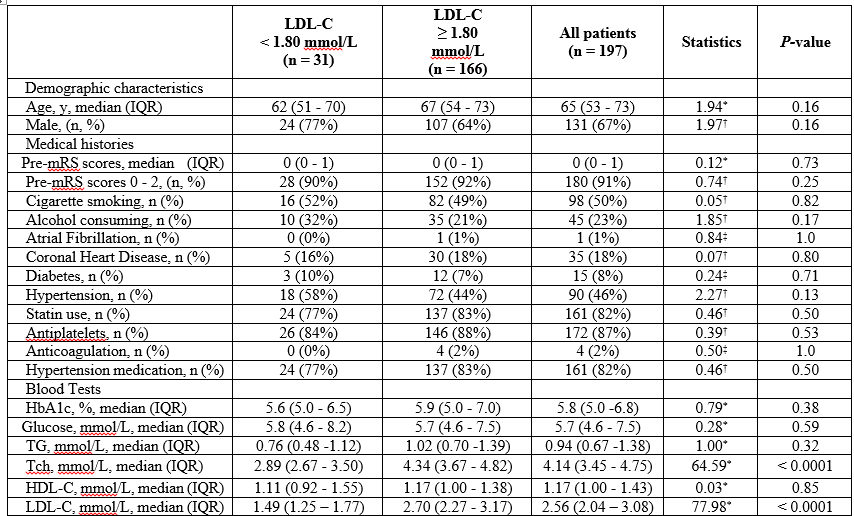
Thirty-one patients had serum LDL-C < 1 xss=removed>
The median of the baseline NIHSS scores in the entire study population was 9. We did not find any differences in the baseline NIHSS scores between the two groups (LDL-C < 1 xss=removed xss=removed xss=removed xss=removed xss=removed xss=removed>

Patients with LDL-C ≥ 1.80 mmol/L have significant improvements in their NIHSS scores at discharge than baseline (estimated change in means: -2.4, 95% CI: [-4.7, -0.1]), but the patients with LDL-C < 1 P=0.54), xss=removed>


ILLT, targeting an LDL-C < 1>
Our outcomes were supported by previous studies. A retrospective study, which analyzed a total of 732 patients with acute ischemic stroke within 72 hours of symptoms onset, indicated that with each 1 mmol/L reduction in LDL-C levels, the risk of an unfavorable outcome (an mRS score of 3–6 points) was increased by 46.2% (OR = 0.538, 95% CI: [0.300, 0.964]; P = 0.037) in the patients with hemorrhagic transformation.[14] But the generality of the study [14] was limited, with the potential selection bias with the high hemorrhagic transformation rate (14.2%). The Helsinki ICH Study was a single-center observational registry of consecutive 964 ICH patients,[15] showing significantly lower LDL-C levels in patients who died at hospital than the survivors (1.9 vs. 2.4 mmol/L; P < 0> 2) (adjusted OR: 1.41) when compared with the patients with TC > 4.14 mmol/L.[16] The retrospective cohort study from another stroke center in China found the rates of unfavorable outcomes (mRS >2) was higher in the ICH patients with lower LDL-C mmol/L (LDL-C < 1> 2.59 mmol/L:57% vs 39% vs. 37%; P <0>
Other lipids was repoted to be associated with the incidence of ICH. Low plasma high-density lipoprotein cholesteral (HDL-C) (<1 trend = 0.024).>
There were many limitations within the current study. Firstly, the sample size was insufficient. In order to test the potential effects of the ILLT in the secondary prevention settings for ischemic stroke, we selected the patients with acute ICH as well as the medical histories of ischemic stroke as the study population. Secondly, the data was collected retrospectively from a single center, the knowledge achieved from the study was warranted to be testified by multiple centers. Thirdly, due to the limitations of the database, we did not adjust the blood pressure status at hospital, which may interfere the outcomes of the hemorrhagic events.
ILLT achieved LDL-C < 1>
Acknowledgements:
The study was supported by the National Natural Science Foundation of China [grant numbers 82001242].
Acknowledgements: none.
Declarations of interest: none
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
