
Research Article | DOI: https://doi.org/10.31579/2641-0419/439
1Division of Vascular and Transplant Surgery, Department of Surgery, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Biomedicine and Health Science, The Catholic University of Korea, Seoul, Korea
3Department of Surgery, Kangdong Sacred Heart Hospital, Seoul, Korea
4Division of Vascular and Transplant Surgery, Department of Surgery, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Gyeonggi-do, Korea
5Department of Statistics and Actuarial Science, Soongsil University, Seoul, Korea
*Corresponding Author: Jeong-Kye Hwan, Division of Vascular and Transplant Surgery, Department of Surgery, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Citation: Jeong K. Hwang, Hyung J.Cho, Ju H. Yoo, Mi H. Kim, Kyung J. Ko, Kang W. Jun, et al, (2025), Association between End-Stage Renal Disease and Abdominal Aortic Aneurysm: A Nationwide Population-Based Cohort Study, J Clinical Cardiology and Cardiovascular Interventions, 8(1); DOI: 10.31579/2641-0419/439
Copyright: © 2025, Jeong-Kye Hwan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 January 2025 | Accepted: 15 January 2025 | Published: 29 January 2025
Keywords: aortic aneurysm; abdominal; end-stage kidney disease; association
Background
Abdominal aortic aneurysm (AAA) and end-stage renal disease (ESRD), defined by need for chronic renal replacement therapy, have similar epidemiological profiles and pathogenic mechanisms. However, studies testing for a connection between these two illnesses are rare. In this research, we tested the hypothesis that there is an association between AAA and ESRD.
Materials and Methods
Data from 2009 to 2015 were extracted from the Korean National Health Insurance Service database for this investigation. The study encompassed 16,671 individuals who had received a new AAA diagnosis. To form a control group, 50,013 participants without the diseases were selected using propensity score matching based on age and sex. The primary endpoint of this study was newly diagnosed ESRD.
Results
The hazard ratio (HR) of ESRD incidence in the AAA group was 2.5 (95% CI 2.0-3.2); in addition, when the AAA group was divided into surgical and non-surgical groups, the HR of the non-surgical group was 2.0 (95% CI 1.5-2.6). When AAA, chronic kidney disease (CKD), and proteinuria co-occurred, the HR of ESRD incidence increased to 128.7 compared to the cases without AAA. There were interactions of diabetes mellitus (DM), CKD, and proteinuria with incidence of ESRD (p < 0.05). In the absence of these comorbidities, the HR for ESRD was higher in the presence of AAA [1.6 vs. 3.8 (DM), 2.3 vs. 3.4 (CKD), and 1.8 vs. 3.0 (proteinuria)].
Conclusions
Our findings revealed a significant correlation between AAA and ESRD even after adjusting for several health conditions. This discovery suggests the need for regular monitoring of AAA patients. This proactive approach can aid in promptly identifying signs of ESRD and addressing modifiable risk factors at an early stage through timely interventions.
Chronic kidney disease (CKD) is defined as an abnormality of kidney function, present for > 3 months, with negative effects on health. Glomerular filtration rate (GFR) is often used as an indicator of renal function. CKD is the diagnosis when the GFR is < 60>
An abdominal aortic aneurysm (AAA) refers to a persistent dilatation of the abdominal aorta that surpasses the standard diameter by 50% or more than 3 cm. In Western populations, the average yearly occurrence of new AAA diagnoses is 0.4-0.67%.4 The current guidelines recommend considering surgical intervention for symptomatic and large asymptomatic fusiform AAAs. In this context, large is defined as a maximum diameter ≥ 55 mm in men and ≥ 50 mm in women.5 However, most asymptomatic AAAs are discovered through screening or incidentally during the diagnosis of other conditions.6 When discovered through screening, the majority of AAA are 4.5 cm or less.7
Oliver-Williams et al.8 determined an AAA mean growth rate of 0.26 (0.25-0.28) cm/year in the first five years in men, with an initial AAA of 3.0-5.4 cm that increased to 0.80 (0.73-0.86) cm/year after 15-19 years. Therefore, even if patients are under surveillance, the condition may progress to a stage that requires surgical treatment. The odds ratio of mortality for patients receiving chronic renal replacement therapy was 4.0 when undergoing vascular surgery compared to that of patients with normal renal function.9 This trend was also present with endovascular treatment.10,11 Therefore, it is important to identify an association between AAA and ESRD to prevent ESRD.
This research tested the hypothesis that a correlation exists between AAA and ESRD. We used data from the Korean National Health Insurance Service (NHIS) database that spanned seven years.
This study is a parallel study to “Risk of various cancers in adults with abdominal aortic aneurysm” and “The risk of dementia in adults with abdominal aortic aneurysm” by Cho et al.12,13 We used similar study protocols, patient group selection methods, and statistical methods.
Data source
The NHIS serves as the sole public medical insurance system in South Korea, providing coverage to approximately 97% of the country's 50 million citizens. The remaining 3% receive coverage through Medical Aid.14 As part of its services, the NHIS offers a health examination program every two years for all insured individuals aged 40 and above and for employee subscribers aged 20 and older. Additionally, the NHIS maintains an extensive dataset of medical records in Korea. These records include patient demographics, medical treatments, procedures, and disease diagnoses following the 10th edition of the International Classification of Diseases (ICD-10). For this study, data from the NHIS database spanning the years 2009 to 2015 were collected.
Study population
Between January 2009 and December 2015, a total of 45,767 individuals was diagnosed with AAA using the appropriate ICD-10 code. Cases of AAA were determined by identifying individuals with multiple instances of AAA diagnosis codes I71.3-I71.6, I71.8, and I71.9 within the previous year at outpatient departments, those who had experienced repeated hospitalizations with these codes, or individuals who had undergone aneurysm repair such as open surgical aneurysmal repair (OSAR) or endovascular aneurysmal repair (EVAR). These surgical repair procedures are indicated by ICD-10 codes of O0223, O0224, O0234, M6611, or M6612. Exclusions were applied to patients who had not undergone a health examination within two years before the diagnosis of AAA (n = 26,123), those aged under 20 years (n = 195), or those with incomplete data (n = 219). Although we intended to exclude patients who had been diagnosed with ESRD prior to their AAA diagnosis, no such cases were found. From the remaining patients, a subset of individuals with greater than one year between the diagnosis of AAA and ESRD was chosen. Therefore, the analysis included 16,671 AAA patients who were matched with 50,013 controls (1:3 ratio) using propensity score matching based on age and sex (Figure 1). The observation period concluded in December 2019. The primary objective of this study was to identify newly diagnosed cases of ESRD. This study was conducted with approval from the Institutional Review Board of The Catholic University of Korea, Eunpyeong St. Mary’s Hospital, Seoul, Korea (PC24ZASI0037).
Figure 1: Enrollment flow chart
AAA: abdominal aortic aneurysm, ESRD: end-stage renal disease
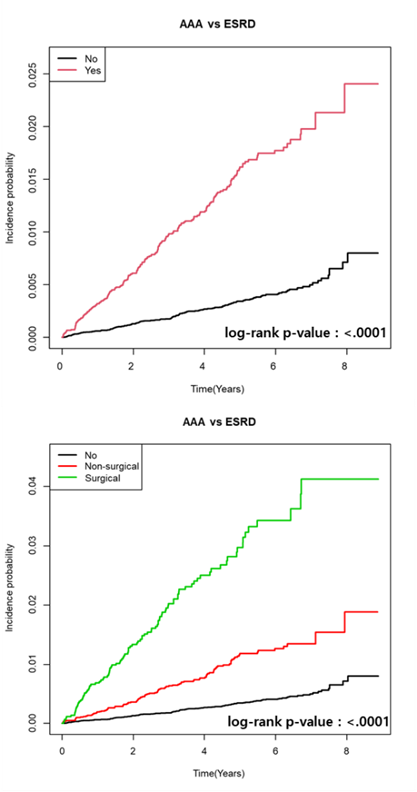
Figure 2: Kaplan–Meier plot for incidence of ESRD in patients with AAA.
AAA: abdominal aortic aneurysm, ESRD: end-stage renal disease
The upper graph illustrates the incidence of ESRD between the AAA group and the control group. The lower graph shows the incidence of ESRD divided among the control group, the group that underwent surgery for AAA, and the group that received non-surgical treatment.
Definitions of ESRD and other covariates
ESRD patients were identified using rare incurable disease codes of V001 (hemodialysis), V003 (peritoneal dialysis), and V005 (kidney transplantation). For CKD, the criterion was the scientifically appropriate estimated GFR measured during routine health examinations. The estimated GFR is calculated using the Modification of Diet in Renal Disease (MDRD) equation; the threshold was defined as less than 60.
Smoking status was categorized as non-smoker, ex-smoker, or current smoker. Alcohol consumption status was categorized as non-drinker, mild-to-moderate drinker (average consumption < 30>
Statistical analysis
For comparing baseline characteristics, Student’s t-tests were employed for continuous variables, and chi-square or Fisher’s exact tests were used for categorical variables. The incidence rates of ESRD are presented per 1,000 person-years. Multivariate Cox proportional hazard regression analyses were performed to evaluate the association between ESRD and AAA.
The hazard ratio (HR) was not adjusted in model 1. Model 2 was adjusted for age; sex; income level; and presence of diabetes, hypertension, and dyslipidemia. In model 3, additional variables of smoking status, alcohol consumption, exercise habits, and BMI were incorporated and adjusted.
Model 4 additionally adjusted for a history of CVD and the presence of CKD. Statistical significance was set at p < 0>
Baseline characteristic
Dyslipidemia and hypertension are recognized as key risk factors for AAA, and these conditions were more commonly observed in the AAA group. Additionally, the AAA group exhibited a higher proportion of smokers and those with elevated BMI and greater waist circumference. Physical activity was notably lower among members of the AAA group, and their alcohol consumption was relatively lower. The proportion of low-income participants in this group was relatively lower. Within the AAA group, there was a greater incidence of patients with DM and individuals with a history of CVD. Significantly more patients with CKD were observed in the AAA group; this corresponded to a reduced eGFR (Table 1)
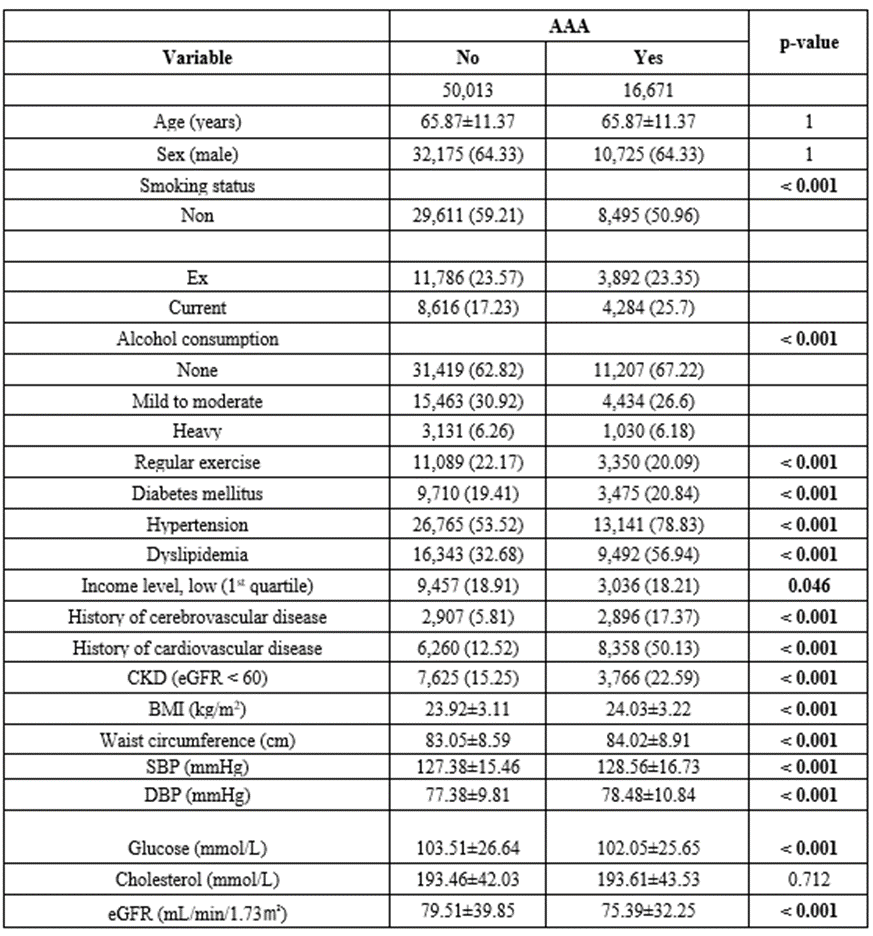
Table 1: Clinical characteristics of control and abdominal aortic aneurysm (AAA) patients.
ESRD risk according to AAA
In a study population of 66,684 participants, 379 (0.56%) developed ESRD. Compared to the control group, the AAA group had a higher risk of ESRD in the unadjusted model, with HR 4.33 (95% CI 3.53-5.31), and also in the fully-adjusted model with HR 2.51 (95% CI 2.0-3.16). In the AAA group, when divided into surgical and non-surgical subgroups, the surgical subgroup had a significantly higher HR (Table 2-1). These results were easily confirmed through the Kaplan-Meier plot, in which the AAA group showed significantly higher incidence probability of ESRD than the control group (Figure 2). This difference was significant as the p-value was less than 0.05 (p-value <0>
Additionally, a more detailed subgroup analysis was conducted based on the presence of proteinuria and CKD. In the unadjusted model, the HRs for ESRD onset were 4.79 (95% CI: 1.69-13.54) for those with proteinuria only, 11.81 (95% CI: 7.72-18.08) for those with CKD only, and 180.39 (95% CI: 118.36-274.91) for those with both conditions. In the fully-adjusted model, these HRs were 3.15 (95% CI: 1.11-8.93), 86 (95% CI: 5.57-13.26), and 86.64 (95% CI: 55.82-134.5), respectively. Moreover, when AAA was present with these conditions, the incidence of ESRD increased dramatically; the fully adjusted model had an HR of 128.66 (95% CI: 81.58-202.9) (Table 2-2).
Interactions with AAA on occurrence of ESRD
In studying the onset of ESRD, we identified variables that interact synergistically with AAA. Among various factors, only the presence of diabetes mellitus (DM), chronic kidney disease (CKD), and proteinuria showed significant interactions, all of which were negative. This implies that the combined effect of AAA with any of these conditions on the risk of developing ESRD is less than would be expected from their individual impacts [1.64 vs. 3.76 (DM), 2.26 vs. 3.39 (CKD), 1.78 vs. 3.01 (proteinuria)] (Table 3) (p-vaule : <0>
| AAA | N | Event | Duration | Rate | Model 1 | Model 2 | Model 3 | Model 4 |
| No | 50,013 | 166 | 235,023.07 | 0.70631 | 1 | 1 | 1 | 1 |
| Yes | 16,671 | 213 | 69,842.43 | 3.04972 | 4.33(3.53,5.31) | 3.26(2.63,4.01) | 3.13(2.53,3.87) | 2.51(2.0,3.16) |
| AAA group divided into surgical and non-surgical groups (Reference : control group) | ||||||||
| No | 50,013 | 166 | 235,023.07 | 0.70631 | 1 | 1 | 1 | 1 |
| Non-surgical | 12,250 | 112 | 53,443.82 | 2.09566 | 2.98(2.34,3.78) | 2.51(1.96,3.21) | 2.45(1.91,3.13) | 2.01(1.55,2.61) |
| Surgical | 4,421 | 101 | 16,398.62 | 6.15906 | 8.79(6.86,11.27) | 4.97(3.83,6.44) | 4.77(3.66,6.21) | 3.65(2.77,4.82) |
| AAA group divided into surgical and non-surgical groups (Reference : non-surgical group) | ||||||||
| No | 50,013 | 166 | 235,023.07 | 0.70631 | 0.34(0.26,0.43) | 0.4(0.31,0.51) | 0.41(0.32,0.52) | 0.50(0.38,0.65) |
| Non-surgical | 12,250 | 112 | 53,443.82 | 2.09566 | 1 | 1 | 1 | 1 |
| Surgical | 4,421 | 101 | 16,398.62 | 6.15906 | 2.95(2.26,3.87) | 2.0(1.51,2.60) | 1.95(1.48,2.57) | 1.82(1.38,2.4) |
Table 2-1. Hazard ratio of AAA for incidence of ESRD.
AAA: abdominal aortic aneurysm, ESRD: end-stage renal disease
Rate: incidence rate per 1,000 person-years
Model 1: non-adjusted. Model 2: adjusts for basic demographics and health conditions, including age; sex; income level; and the presence of diabetes, hypertension, and dyslipidemia. Model 3: includes all factors from Model 2 and further adjusts for lifestyle factors of smoking status, alcohol consumption, exercise status, and body mass index (BMI). Model 4: builds on Model 3, adding adjustments for a history of cardiovascular disease (CVD) and the presence of chronic kidney disease (CKD).
| CKD | UPRO | AAA | N | Event | Model 1 | Model 2 | Model 3 | Model 4 |
| No | No | No | 41,308 | 32 | 1(Ref.) | 1(Ref.) | 1(Ref.) | 1(Ref.) |
| No | Yes | No | 1,080 | 4 | 4.79(1.69,13.54) | 3.15(1.1,8.83) | 3.14(1.11,8.9) | 3.15(1.11,8.93) |
| Yes | No | No | 7,059 | 63 | 11.81(7.72,18.08) | 8.74(5.67,13.48) | 8.65(5.61,13.33) | 8.6(5.57,13.26) |
| Yes | Yes | No | 566 | 67 | 180.39(118.36,274.91) | 89.79(57.94,139.14) | 86.15(55.51,133.70) | 86.64(55.82,134.5) |
| No | No | Yes | 12,391 | 44 | 5.04(3.2,7.95) | 3.9(2.46,6.19) | 3.80(2.39,6.05) | 3.48(2.18,5.57) |
| No | Yes | Yes | 514 | 12 | 33.86(17.44,65.75) | 19.56(10.0,38.28) | 19.17(9.77,37.61) | 17.6(8.93,34.7) |
| Yes | No | Yes | 3,369 | 95 | 45.89(30.73,68.51) | 28.99(19.17,43.85) | 27.89(18.41,42.26) | 25.49(16.68,38.96) |
| Yes | Yes | Yes | 397 | 62 | 288.95(188.49,442.97) | 146.16(93.78,227.78) | 139.87(89.52,218.54) | 128.66(81.58,202.9) |
Table 2-2. Hazard ratio of AAA for incidence of ESRD. (Further analysis)
AAA: abdominal aortic aneurysm, ESRD: end-stage renal disease, CKD: chronic kidney disease, UPRO: urine protein (≥ 1+ dipstick proteinuria)
Model 1: non-adjusted. Model 2: adjusts for basic demographics and health conditions, including age; sex; income level; and the presence of diabetes, hypertension, and dyslipidemia. Model 3: includes all factors from Model 2 and further adjusts for lifestyle factors of smoking status, alcohol consumption, exercise status, and body mass index (BMI). Model 4: builds on Model 3, adding adjustments for a history of cardiovascular disease (CVD) and the presence of chronic kidney disease (CKD).
Most research on the relationship between AAA and renal function has focused on the relationships between treatments for AAA and renal function. For example, OSAR and EVAR were both associated with acute kidney injury (AKI); and the incidence of AKI was higher in the OSAR group.15,16 Factors affecting this relationship included preoperative hemoglobin level and eGFR, operation duration, history of cardiovascular disease, and amount of bleeding and transfusion.17 However, unlike AKI, there was no significant difference in the incidence of postoperative CKD between OSAR and EVAR from one to five years after surgery.18–21 Age > 70 years, renal artery stenosis (RAS) ≥ 70%, peri-procedural AKI, graft complications, larger neck diameter, and angio-CT followed by stent-graft implantation over a short time interval were independent risk factors for CKD.18,21–23 In this study, the HR of ESRD was significantly higher in the surgical group compared with the non-surgical group [HR: 1.82 (95% CI 1.38-2.4)].
However, the association between AAA and ESRD required more attention. In this regard, Barisione et al.24 provided clues for the increased CKD and cardiac damage risk profiles of AAA patients. The reason that this relationship is important is that the size of AAAs increases gradually. As shown by Olson et al.,25 26% of patients with a maximum transverse diameter of at least 4.25 cm exceeded sex-specific repair thresholds (5.5 cm for men and 5.0 cm for women) at two years. A significant number of patients under surveillance for AAA eventually required surgery. Therefore, an ESRD prevalence higher in AAA patients compared to a control group has significant clinical implications. First, the prognosis is better for those with an early CKD diagnosis who are provided appropriate treatment. This recognizes the potential for declining renal function in AAA patients, and active monitoring can help preserve kidney function in the long term. Second, since a significant number of patients under surveillance for AAA eventually undergoes surgery and ESRD has been reported as a major factor affecting outcomes in AAA surgery, focusing on preserving renal function in AAA patients can potentially improve the surgical and post-surgical outcomes.26
The results of the subgroup analysis showed that the presence of CKD increases the likelihood of developing ESRD, and this was also true for the proteinuria group. AAA patients with proteinuria require particular attention. Proactive surveillance is necessary for these patients. Of course, one reason for these findings may be that surveillance in the AAA group often involves the use of contrast agents for CT scans or that renal function can be impaired due to surgical interventions. However, this is not always the case since Table 2 demonstrates that, even in the non-surgical subgroup, the prevalence of ESRD was higher in the AAA group compared to the control group.
DM, CKD, and proteinuria are significantly associated with and are risk factors for ESRD.27 Indeed, ESRD incidence increases when these conditions coexist with AAA. However, the reason these factors exhibit a negative interaction effect may be that the impact these variables have on ESRD shares common mechanisms with AAA influence on the onset of ESRD. This overlap might result in a lower relative contribution of AAA.
The study has some limitations. First, the observational design of our study restricts our ability to infer a causal relationship. To mitigate this limitation as much as possible, we only enrolled patients who had a one-year time lag; and we utilized a Cox proportional hazards regression model to approximate as closely as possible the direct associations with the variables.
Additionally, even if we strive to accurately estimate the associations between variables, our definitions for ESRD and the AAA patient group may lack precision since they were identified using disease codes. Second, the mean eGFR values of the AAA group and the control group were significantly different, although the eGFR values were in the same category (G2; 60-89 mL/min/1.73m2). The values were 75.39 for the AAA group and 79.51 for the control group. This could have been a natural result because there were many CKD patients in the AAA group, but this difference may have created a bias. Third, in this study, because the incidence of ESRD was low, careful interpretation of the results is necessary. The small number of events may have affected the statistical power and reliability of the results, which may limit the generalizability of our findings. Therefore, larger-scale studies with a greater number of events are needed in the future. Fourth, since the study was conducted only on Koreans, the effect of race could not be analyzed.
Nevertheless, our study possesses several strengths. First, we established a connection between AAA and ESRD, a relationship not explored in previous research. Second, our research utilized a substantial national dataset coupled with an extensive follow-up duration. Third, we examined the effect of the coexistence of CKD and proteinuria on the relationship between AAA and ESRD and analyzed interactions among several variables.
Through this research, we identified a high incidence of ESRD among AAA patients, highlighting the necessity of meticulous renal function monitoring during the treatment or surveillance of this patient group. Moreover, the particular attention required by patients with existing CKD or proteinuria has been highlighted as these conditions significantly increase the prevalence of ESRD. Ultimately, our suggestions will not only help preserve renal function in patients, but also positively influence the outcomes of AAA treatment, especially after surgery
None of the authors have anything to disclose.
None declared.
This research was supported by a grant funded by The Catholic University of Korea, Eunpyeong St. Mary’s Hospital, Research Institute of Medical Science in program year 2023.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
