
Research Article | DOI: https://doi.org/10.31579/2768-0487/134
1 Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
2 Obstetrics Gynecological Nursing, Faculty of Nursing Benha University.
*Corresponding Author: Hanan Elzeblawy Hassan., Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Citation: Abdelazim Mohamed SS, Elham A. Ramadan, Hanan E. Hassan, Hassan Omran AA, (2024), Assessment of the Severity of Urinary Incontinence Among Elderly Women, Journal of Clinical and Laboratory Research, 7(5); DOI:10.31579/2768-0487/134
Copyright: © 2024, Hanan Elzeblawy Hassan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 March 2024 | Accepted: 25 April 2024 | Published: 30 April 2024
Keywords: elderly women; urinary incontinence
Background: The International Continence Society (ICS) defines urinary incontinence (UI) as the complaint of any involuntary leakage of urine. It is a distressing and debilitating condition that is becoming more prevalent as our population ages. Pathophysiology of urinary incontinence during menopause the ovaries stop producing considerable quantities of estrogen; hence the symptoms and problems associated with estrogen deficiency occur gradually. Among the changes is reduction in the integrity of the pelvic floor, changes in the rate of different types of collagens and the preferential atrophy of type II muscle fibers, atrophy of urinary-genital tract which may be associated with problems such as urinary urgency, urinary frequency, nocturia, stress incontinence, urge incontinence, burning upon urination and an increased prevalence of urinary tract infections.
Aim of the study: The study aimed to assess severity of urinary incontinence among elderly women.
Design: A descriptive study design was utilized in this study.
Sample: A purposive sample of 100 women diagnosed with stress urinary incontinence.
Setting: gynecological and urological outpatient clinics Beni-Suef university hospital.
Tools: (1) A structured interviewing questionnaire sheet was developed by the researcher in the Arabic language. It was containing of two parts; (1) personal characteristics data of the study women such, (2) urinary incontinence history; (2) The International Consultation on Incontinence Modular Questionnaire ICIQ-SF.
Results: The mean weight of the studied sample was 82.680±11.8815, mean height was 160.420±2.8610, and mean of BMI was 32.1224±4.47973. It indicates that 42% of the study sample their frequency of urination was every 3-6 hours, 75% of them had a completely empty bladder after voiding, 37% did not used sanitary towel for urine leakage.
Conclusion: Based on the results of the study; It can be concluded that most of elderly women suffer from sever urinary incontinence.
Recommendations: Replication of the present study under different circumstances (sampling and setting) is recommended to validate its results.
Urinary incontinence (UI) is defined by the International Continence Society (ICS) as any involuntary urine leakage. As our population ages, this disturbing and crippling disorder is becoming more common. It has substantial negative effects on quality of life, both psychologically and physically, and it has serious economic repercussions [1-4]. The pathophysiology of urine incontinence involves the ovaries ceasing to produce significant amounts of estrogen throughout menopause, which causes the symptoms and issues related to estrogen insufficiency to gradually manifest.. Reduced pelvic floor integrity, variations in the rate of various collagen types, preferential atrophy of type II muscle fibers, and atrophy of the urinary-genital tract are a few of the changes. These may be linked to issues like nocturia, stress and urge incontinence, burning when urinating, urinary urgency, and a higher incidence of urinary tract infections. Dyspareunia is sometimes caused by a weak vaginal mucosa [5-8]. Idiopathic etiologic factors of urge urinary incontinence include myogenic, neurogenic, and urethrogenic manifestations. Anatomical considerations are important, including pelvic masses, urethral diverticulum, bladder outlet obstruction, and pregnancy. Bladder inflammation, urinary tract infections, urinary stones, bladder cancer, or benign urothelial growths could cause Urge Urinary Incontinence. Behavioral factors like excess fluid and caffeine intake, habitual increased voiding frequency, and obsessive anxiety about urinary problems have a significant effect. Chronic medical conditions like diabetes, multiple sclerosis, Parkinson’s disease, brain tumors, other neurological diseases, and spinal cord injury also contribute to Urge Urinary Incontinence [9-12].
Diagnostic evaluation of urinary incontinence can be obtained by several points as:
(1) History taking: In establishing the history, the opportunity should be taken not only to describe symptoms, but also their progression, impact on lifestyle and possible risk factors. Multiple symptoms are commonly reported and during the history it is important to define the most troublesome symptoms and the patient’s expectations from treatment [13].
(2) Urological history: Lower urinary tract symptoms (LUTS) are categorized by the International Continence Society (ICS) into three categories: storage, voiding, and post-micturition symptoms. While an accurate urological history does not provide a conclusive diagnosis, it does serve as a useful guide for further testing and treatment [14].
(3) Gynecological history: It is important to establish the estrogen status as estrogen receptors are present within the lower urinary tract, and are shown to influence cell proliferation. Women with estrogen deficiency may complain of urgency and frequency and recurrent urinary tract infections may develop because of loss of urethral mucosal cooptation. In women of reproductive age, symptoms may vary with the menstrual cycle. It is equally important to consider aspects of obstetric, medical and surgical history, all of which may be of relevance to causes and management of incontinence [14].
(4) History of Drugs use: Many drugs affect the lower urinary tract, either as a result of their autonomic activity, or by indirect mechanisms; patients should be asked whether symptoms changed after they commenced or altered the dose of any of their medications. Diuretics cause increased urinary frequency; alpha adreno-receptor blockers are associated with stress urinary incontinence. Caffeine and nicotine ingestion will aggravate irritative bladder symptoms [13].
(5) A functional assessment that looks at the patient's mobility, mental state, and body mass index should be part of the physical examination. An examination of the abdomen should look for pelvic tumors, a palpable bladder, and pain at the costal vertebral angle. Vaginal atrophy and incontinence-associated dermatitis, or skin damage from contact to urine, may be found during the urogenital examination [15–17].
(6) It is recommended to perform a digital examination by palpating the pelvic floor to assess muscle tone, contraction technique, and strength. Although terminology related to pelvic floor function has been standardized, there is currently no normative value or standardized method for measurement or classification. When looking for signs of pelvic organ prolapse, other anomalies such pelvic masses and urethral diverticula—an out-pouching of the urethral mucosa that results in a cystic mass in the midline anterior wall—can also be seen [1].
(7) Lastly, a speculum examination can help evaluate each vaginal compartment and check for any urine leakage that occurs outside of the urethra, which could indicate a fistula. A rectal examination with sphincter squeeze and tone assessment should be performed in the event of any neurological complaints or bowel problems. Furthermore, a general neurological evaluation, which includes assessing the S2-S4 nerve distribution, should be prompted by gastrointestinal dysfunction [15].
(8) Urological tests, such as 3- to 7-day voiding diaries, are commonly employed as a dependable instrument that is sensitive to minute changes. Voiding diaries provide an objective measurement of mean voided volume, frequency, and frequency of urine incontinence. Urine diaries can be of three types: a micturition chart that logs the time of each void; a frequency–volume diary that logs the volume voided with the time; and a bladder diary that logs extra details about episodes of urine incontinence, pad use, fluid intake, fluid type, and urgency feeling. Furthermore, a 24-hour urine production record can be used to evaluate polyuria during the day and at night, which is especially helpful for elderly women who experience nocturia [18].
Significance of the study
Urinary incontinence is a major global health problem. The prevalence of UI increases with age, though the prevalence rate in women. The prevalence of urinary incontinence (UI) in Egypt is difficult to estimate due to several factors, including embarrassment, the belief that UI is a normal part of aging and childbirth, and the fact that most Egyptian women are reluctant to seek help for UI. Therefore, more research needs to be done to determine the precise prevalence of UI in Egypt. Urinary incontinence has a significant influence on physical, psychological, and social health and wellness, including sleep issues, low self-esteem, sadness, and psychological anguish, even though it's not a life-threatening condition.
Aim of the study
The study aimed to assess severity of urinary incontinence among elderly women
Research questions
What about severity of urinary incontinence among elderly women?
Subject and methods
Study design:
The study followed a descriptive study design.
Study Setting and Sampling:
The study was conducted at gynecological and urological outpatient clinics at Beni-Suef University Hospital. Total sample was 100 women.
Tools of data collection:
Tool I: With the help of supervisors, the researcher created a structured questionnaire sheet in Arabic based on a review of recent literature. It was divided into two sections:
The first part: Includes the study women's personal characteristics (age, height, weight, body mass index, or "BMI"), education level, occupation, place of residence, and marital status in the first section.
The second part: urinary incontinence history included duration of illness, frequency, amount of leakage of urine, timing (day and night), and predisposing factors as coughing, sneezing, laughing, using sanitary towels for urine leakage, frequency of change the towels.
The Modular Questionnaire from the International Consultation on Incontinence is Tool II. ICIQ-SF: (conducted by the International Consultation on Urological Diseases (ICUD, 1998) and supported by the World Health Organization (WHO): Urinary incontinence frequency and severity are assessed using the self-reported ICIQ survey and screening tool. It had six total items overall, four of which asked for a rating of symptoms throughout the previous four weeks. The ICIQ-UI Short form is used to assess symptoms both before and after an intervention. Its score ranges from 0 to 21, with a higher score indicating greater intensity of symptoms.
Scoring system of the ICIQ-UI:
Tools of data collection were investigated for their content validity by three experts in the field of Obstetric and Gynecological Nursing from Faculty of Nursing and Benha University.
Administrative Design:
The director of Beni-Suef University Hospital received an official written consent letter from the dean of Benha University's college of nursing outlining the goal of the study and authorizing data collection.
Using IBM SPSS, a statistical tool for social sciences, the gathered data was updated, coded, tabulated, and input into a computer. Data were shown, and appropriate analysis was carried out in accordance with the kind of data found for each parameter.
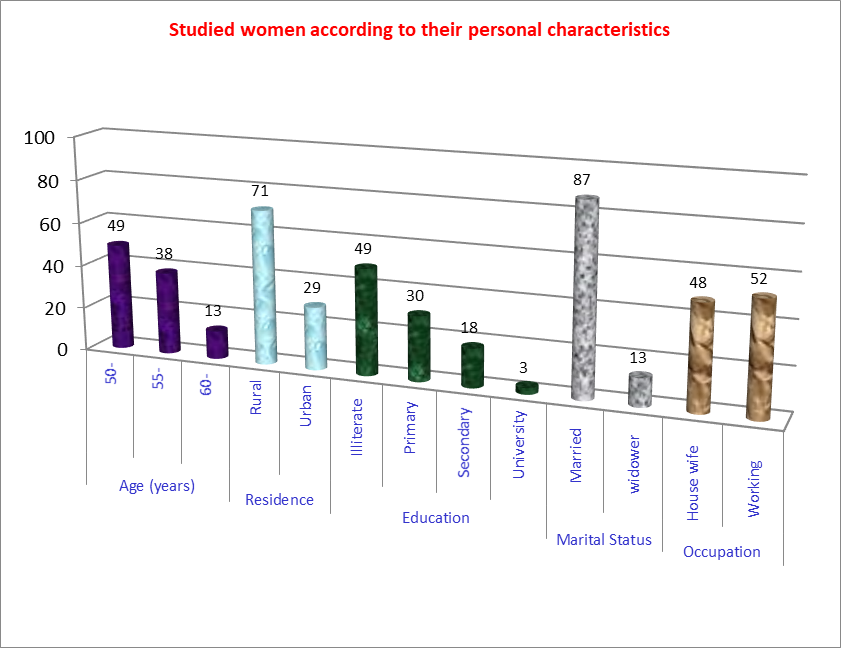
Figure 1: Distribution of studied sample according to personal characteristics (n=100).
Figure 1: Reveals that more than one-third (38%) of the studied sample were aged 55-60 years old, and 29% were from urban areas, also 49% of them were illiterates and 48% of them were housewives.
| Personal Characteristics | |
| Weight Mean ±SD | 82.680±11.8815 |
| Height Mean ±SD | 160.420±2.8610 |
| BMI Mean ±SD | 32.1224±4.47973 |
Table 1: Displays the distribution of studied sample according to body characteristics. It reveals that mean weight of the studied sample was 82.680±11.8815, mean height was 160.420±2.8610, and mean of BMI was 32.1224±4.47973.
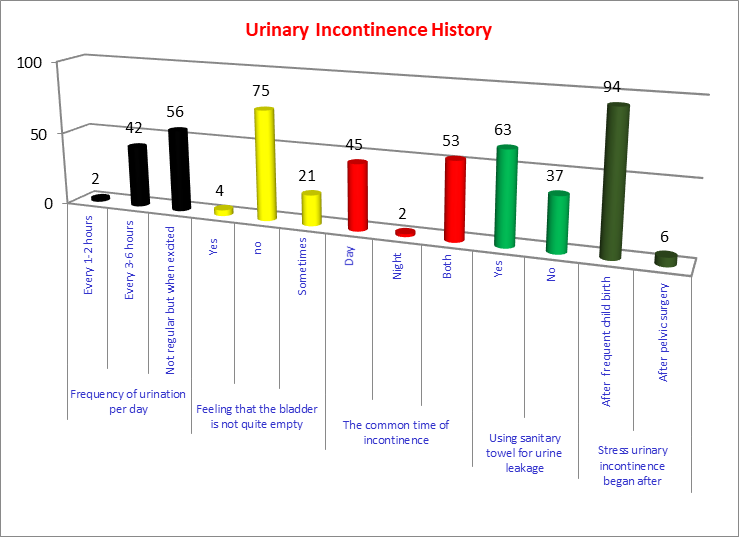
Figure 2: Distribution of studied sample according to urinary incontinence history (n=100).
Figure 2: Present the distribution of studied sample according to urinary incontinence history. It indicates that 42% of the study sample their frequency of urination was every 3-6 hours. Moreover, 75% of them had a completely empty bladder after voiding; 45% of them experienced stress urinary incontinence during day. It reveals from both figures that 37% of the studied sample did not used sanitary towel for urine leakage.
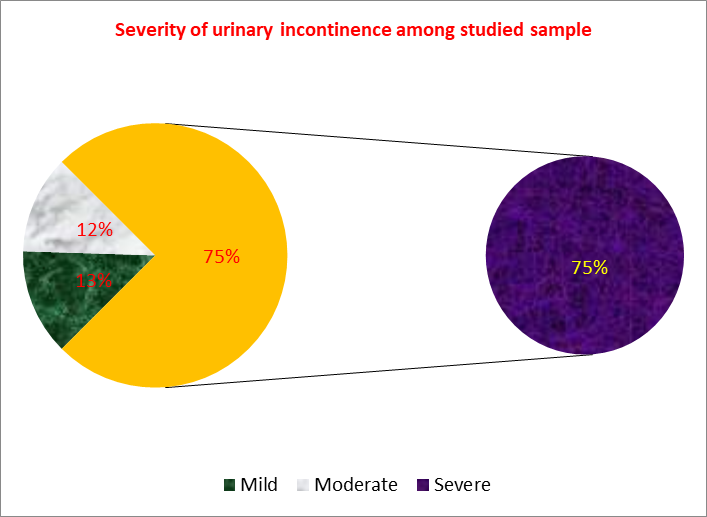
Figure 3: Distribution of studied sample according to the severity of urinary incontinence (n=100).
Figure 3: Demonstrated the distribution of studied sample according to the severity of urinary incontinence. It reveals that 75% of the studied sample has severed urinary incontinence.
Incontinence is one of the many health issues that older women face, particularly because of age-related changes in the lower urinary tract, physical limitations, and living conditions [19].Incontinence is one of the many health issues that older women face, particularly because of age-related changes in the lower urinary tract, physical limitations, and living conditions [19]. In relation to marital status, the current study showed that majority of the studied women were married, while slightly more than tens of them were widow. This finding were congruent with Mohamed, H et al (2018) who studied the Effect of pelvic floor muscle strengthening-kegel exercise on severity of stress urinary incontinence and quality of life among women and mentioned that majority of the control and the study groups were married [20]. Obesity is considered as a one of main etiological factor of urinary incontinence. The results of the present study revealed that the mean weight of the studied sample was 82.680±11.8815, mean height was 160.420±2.8610, and mean of BMI was 32.1224±4.47973. Genetic susceptibility or predisposition to having poor tissue strength can be considered a contributing factor. Stress urinary incontinence may be caused by individual behavioral characteristics such as smoking, obesity, alcohol use, excessive liquid intake, caffeine consumption, and strenuous activity. Stress urinary incontinence may be confounded by medical problems like age, estrogen insufficiency, and chronic obstructive pulmonary disease [1]. Many risk factors have role in the occurrence of UI as weak pelvic floor muscles supporting the proximal urethra, obesity, pregnancy and childbirth, menopause and old age, hysterectomy, constipation. Caffeine and alcohol consumption increase the risk of urinary urgency. Urinary tract infections can also temporarily induce UI, nerve damage can disrupt signals from the bladder to the brain, preventing patients from feeling the urge to urinate, and certain medications can also impair bladder control [21–22].
Based on the results of the study; It can be concluded that most of elderly women suffer from sever urinary incontinence.
Replication of the present study under different circumstances (sampling and setting) is recommended to validate its results.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
