
Research Article | DOI: https://doi.org/10.31579/2641-0419/289
1 Division of Cardiology, Parma University Hospital, Parma, Italy.
2 Division of Cardiology, IRCCS Arcispedale Santa Maria Nuova, Reggio Emilia, Italy.
3 Division of Cardiology, University of Parma, Parma University Hospital, Parma, Italy.
4 Cardiac Surgery Intensive Care Unit, Parma University Hospital, Parma, Italy.
5 Clinic of Radiology, Medical faculty, University of Muenster, Germany
6 Department of Medicine and Surgery, University of Parma, Italy.
7 Division of Cardio surgery, University of Parma, Parma University Hospital, Parma, Italy.
*these authors equally contributed to this work as first author.
*Corresponding Author: Emilia Solinas, MD, PhD, Division of Cardiology, Parma University Hospital, via Antonio Gramsci 14, 43126, Parma Italy.
Citation: Rossella Giacalone, Marco Ferretti, Filippo Luca Gurgoglione, Antonella Vezzani, Bettina Pfleiderer. et all (2022). Assessment of the Role of NonTraditional Risk Factors on Spontaneous Coronary Artery Dissections. J. Clinical Cardiology and Cardiovascular Interventions, 5(8); DOI:10.31579/2641-0419/289
Copyright: © 2022 Emilia Solinas, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 July 2022 | Accepted: 29 July 2022 | Published: 05 August 2022
Keywords: spontaneous coronary artery dissection; non traditional risk factors; gender; diagnostic tool; primary prevention; outcomes studies
Abstract
Background: Spontaneous coronary dissection (SCAD) and non-traditional risk factors (NT-RF) have assumed increasing interest.
Aim: To assess NT-RF in the Parma SCAD registry population.
Methods: 62 patients with SCAD, enrolled between January 2013 through November 2021, were divided in two groups: NT-RF (n=51) and T-RF (n = 11). Clinical, echocardiographic and angiographic features were compared between the two study populations; finally, the occurrence of major adverse cardiovascular events was assessed at follow-up.
Results: At least one NT-RF among sex related, sex prevalent and gender specific risk factors was present in 82% of patients, while TRF for atherosclerotic disease were less common with hypertension being the most prevalent (40.3%) and diabetes the most seldom (3.2%).
Patients with NT-RF were significantly younger (p=0.027) and mostly female compared to those without NT-RF (p=0.004). Type 2 (second Yip/Saw classification) dissection was the prevailing phenotype (54.8%) with a higher prevalence in the NT-RF group (63%, p=0.035).
Major Adverse Cardiovascular Events (MACEs) occurred in 17.7% in all patients at a median follow-up of 23 months. When comparing the incidence of cardiovascular events in the 2 study groups, we did not find any significant differences (p=0.4) between groups.
Conclusion: SCAD occurs more often in younger women without the traditional RF. Risk estimation does not include these factors and tailored prediction models are lacking. Clinicians and researchers should establish targeted interventions for primary prevention, early diagnosis and secondary prevention in younger women.
Spontaneous coronary artery dissection (SCAD) is a typical disease in younger female patients (mean age 35 to 40 years) and it is the most common reason for myocardial infarction in pregnant and postpartum women. [1-3] Patients seem often to lack the traditional typical risk factors for coronary heart disease: a strong correlation of occurrence with SCAD was observed only with hypertension. [4,5]
Lately, non-traditional risk factors (NT-RF) and their role in cardiovascular diseases in women are gaining increasing interest, but only few data are available so far in SCAD.[5-7] NT-RF refer to a mix of sex-associated and under-recognised gender factors affecting cardiovascular risk in women, in addition to the well-known “traditional risk factors” including hypertension, dyslipidemia, smoking, diabetes and a family history of cardiac disease [8] Sex-associated risk factors are linked to the biological aspects of being male or female and genetical differences between the female and male sex, while gender is a social construct which refers to the characteristics of women, men, girls and boys that are socially constructed and influenced by an individual’s environment including gender identity according to the World Health Organization -WHO definition (https://www.who.int/health-topics/gender#tab=tab_1)
NT-RF can be divided into three main categories: Sex-specific (SS-NT-FR), Sex-predominant (SP-NT-RF) and Gender-related NT-risk factors (GR-NT-RF) (Figure 1), according to The Lancet women and cardiovascular disease Commission [8].
Sex-specific risk factors include risk factors associated with biological and genetical differences between the female sex and male sex with endogenous and exogenous reproductive hormone levels playing an important role. [9]
SCAD is the most common cause of pregnancy associated myocardial but still poorly characterized (P-SCAD). Compared with other women of childbearing age in the U.S. population, patients with P-SCAD were more frequently treated for infertility, multiparous and had a diagnosis of pre-eclampsia. Moreover, compared with non-pregnancy associated NP-SCAD, patients with P-SCAD had a more severe clinical presentation, were more likely to experience SCAD affecting the left main or multiple vessels and had a lower mean left ventricular ejection fraction (LVEF) at SCAD diagnosis. [10-11]
SCAD following use of oral contraceptives and pseudo-menopause therapies has also been well described. [12]
Sex-predominant risk factors include several not sex-associated diseases which disproportionally affect women more often in comparison to men like Inflammatory and Autoimmune diseases, connective tissue disease, Thyroid disorders and migraine. [8]
Although coronary atherosclerotic disease is the main cause of acute coronary syndrome (ACS) in patients with Systemic Lupus Erythematous (SLE), SCAD is probably a more common cause of ACS than reported in the literature. [13]
Approximately 5% of patients with SCAD have heritable connective-tissue disorders such as Marfan, Ehlers-Danlos and Loeys-Dietz syndromes. [14,16]
Thyroid hormones affect the metabolism of all cells and tissues in the body. In a series of 73 patients with SCAD, 26% were affected by hypothyroidism. SCAD patients with hypothyroidism had a higher frequency of distal vessel involvement and tended to show a more diffuse involvement, have a greater tendency for relapse, and lower spontaneous resolution during follow-up. [17]
The finding that migraine is more common in SCAD patients compared to atherosclerosis-related ACS has been reported by Krittanawong et al. with lifetime prevalence estimated at 40%. [7]
Gender-related risk factors encompass several under-recognised psycho-social factors which can be related to gender and culture and to their interaction in a woman’s social and physical environment (Figure 1) [8].
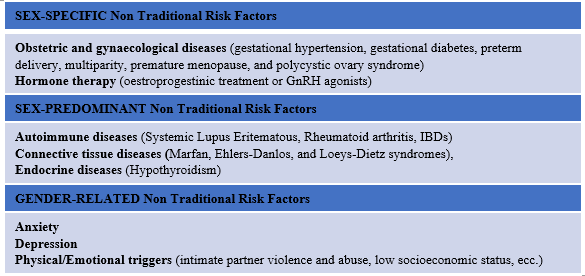
* We created this figure for this article; it is not based on any previously published image. Copyright will belong to Journal of Clinical Cardiology and Cardiovascular Intervention, but substantial rights for future use are granted back to the author.
Figure 1: Classification of non-traditional risk factors
Evolving evidence indicates that SCAD is more frequently preceded by an emotional crisis in women (40–56% of cases), whereas heavy physical exertion (18–24%) more often precedes the event in males. [4,6] Moreover, findings indicated high levels of perceived stress and fatigue in women after SCAD. [18]
Depression and anxiety are associated with increased risk of cardiovascular disease morbidity and mortality and depression is an independent and long-term risk factor for both obstructive and non-obstructive coronary artery disease in women. [19,20]
The objective of this study was to assess the role of non-traditional risk
factors in the “Parma SCAD registry” and their correlation with baseline characteristic of SCAD population and major cardiovascular adverse outcomes (MACEs).
We reviewed 62 patients enrolled in the “Parma SCAD registry” between January 2013 through November 2021, with complete medical records and surveys. Inclusion criteria were age ≥ 18 years and angiographic diagnosis of SCAD according to the Saw angiographic classification (Figure 2), made by experienced interventional cardiologists. [21] The Thrombolysis In Myocardial Infarction (TIMI) flow grade classification was used to better characterize the SCAD lesions. [22] All angiograms were reviewed by another experienced interventional cardiologist to confirm the diagnosis.
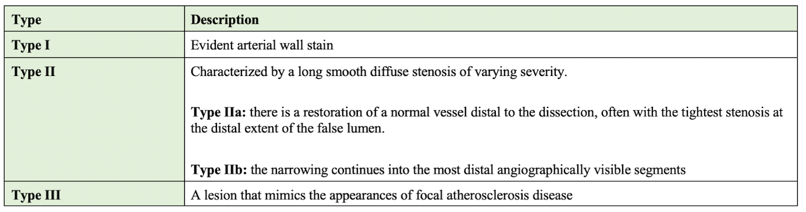
* We created this figure for this article; it is not based on any previously published image. Copyright will belong to Journal of Clinical Cardiology and Cardiovascular Intervention, but substantial rights for future use are granted back to the author.
Figure 2: Yip-Saw Classification
Patient prior medical history (including past medical and reproductive history, hormonal therapy, clinical, mental health and other psychological characteristics and current medical status and therapy), clinical presentation, coronary angiography and other imaging techniques (including screening of extra-coronary arteriopathy when available), interventional procedures (percutaneous coronary interventions or coronary artery bypass grafting, PCI or CABG) and in-hospital outcomes of the index event were registered in the database.
During the last few years of the study (2018-2021), in accordance with international expert consensus, we started to routinely screen our SCAD population for fibromuscular dysplasia (FMD) with computed tomography angiography (CTA) or Magnetic Resonance Angiography (MRA), which were interpreted by dedicated vascular radiologists. [5]
We defined as traditional risk factors (TRF) the well-established factors for SCAD including hypertension, dyslipidemia, smoking, obesity, family history of CAD and diabetes, in contrast to non-traditional risk factors (NT-RF), which are usually not considered when assessing risk profiles for cardiovascular diseases and SCAD, and we further divided them in three groups, according to the description in The Lancet women and cardiovascular disease Commission [8] :
Diagnosis of depression was based on a previously diagnosed condition characterized by feelings of tension/worried thoughts for anxiety and a persistent feeling of sadness and loss of interest interfering with daily activities for depression, for which the patient took specific medications after the diagnosis and specialistic prescription. [24]
The rate of major adverse cardiovascular and cerebrovascular events (MACEs) was used to assess the prognosis of patients with SCAD. MACEs were defined as the composite of all-cause death, myocardial infarction (MI) according to the fourth universal definition, including propagation of initial SCAD lesion and recurrent SCAD (defined as the development of de novo dissection with new MI unrelated to the extension of original SCAD lesion, need for target vessel revascularization (TVR), acute ischemic stroke and transient ischemic attack according the major recent definition. [25,26]
The outcomes were assessed during hospitalization, thirty days after discharge and at the end of follow-up. Outcomes of patients were obtained through clinical visits, telephone interviews or medical record in case of readmission reported in our registry. Duration of follow-up was determined by last clinical visit or study correspondence.
The registry was conducted in accordance with the Declaration of Helsinki and approved by local ethics committee. All-comers patients have written informed consent for participation in the “Parma SCAD registry”. A waiver of consent was given for patients who had died or could not be contacted.
Statistical data analyses
Following data collection, we have identified two groups of patients: the first group, represented by patients with non-traditional risk factors (NT-RF; as previously described), and a second group, less numerous, with only traditional risk factors (T-RF). The clinical/anatomical characteristics and outcomes were performed by comparing the two groups of patients.
Continuous variables were presented as mean ± standard deviation (SD). Categorical variables were presented as frequencies and percentages In case of skewed distribution, variables were summoned up as medians (interquartile range). Unpaired Student’s t-test if or Mann–Whitney U-test were used to compare continuous variables according to the presence of normal distribution or not and categorical variables were compared by Chi-Square test or Fisher exact test as appropriate. All tests were two-sided, and a p-value of <0>
Baseline clinical and anatomical characteristics of the overall population
Of the 62 patients identified as SCAD, 55 were Caucasian women (88.7%) with mean age at diagnosis of 53 years (IQR 47.7; 63) and non-pregnant body mass index of 24.2±4.2 kg/m2 .
Table 1 shows all clinical and anatomical characteristics of the study population.
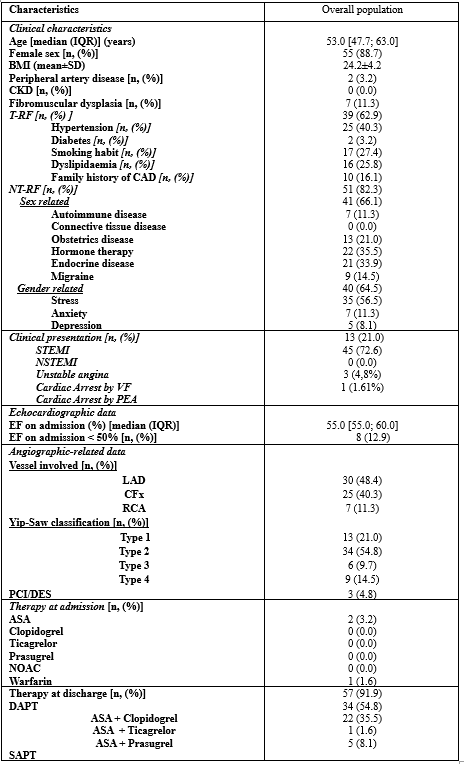
Legend to table: IQR: InterQuartile Range; CKD: Chronic Kidney Disease; T-RF: Traditional Risk Factors; CAD: Coronary Artery Disease; BMI: Body Mass Index; SD: Standard Deviation; NT: Non-Traditional Risk Factors; STEMI: ST-segment Elevation Myocardial Infarction; NSTEMI: NON-ST segment Elevation Myocardial Infarction; VF: ventricular fibrillation; PEA: pulseless electrical activity; NOAC: New Oral Anticoagulant; ASA: Cardioaspirin; EF: Ejection Fraction; LAD: Left Atrial Descending; CFx: Circumflex; RCA: Right Coronary Artery; PCI-DES: Percutaneous Coronary Intervention – Drug Eluting Stent; DAPT: Dual Anti-Platelet therapy; SAPT: Single Anti-Platelet therapy
Table 1: Clinical, echocardiographic and angiographic features of patients with spontaneous coronary artery dissection in our study sample of the Parma SCAD registry population (n = 62).
Traditional risk factors for atherosclerotic disease were less common: hypertension was the most prevalent (25 pts, 40.3%) in line with other series, 17 patients (27.4%) had a smoking habit, 16 patients had dyslipidemia (25.8%) and 10 patients reported about a family history of CAD. Only two patients had diabetes (3.2%).
In relation to non-traditional risk factors, 51 patients (82%) had at least one of them, and more than half of the total population had at least one sex-related risk factor (66%) or gender-related risk factor (64,5%).
Patients with SCAD reported more frequently sex-specific NT-RF as a prior history of a obstetric disorder (13 pts, 21%) such as pre-eclampsia, gestational diabetes mellitus and hypertension during pregnancy. A medical history of multiple abortions was the most common (6 pts, 9,7%) among the disorders in the obstetric setting. Two cases were identified as peripartum SCAD (P-SCAD).
Among the sex-predominant NT-RF, hormone therapy (22 pts, 35.5%) and endocrine diseases (21 pts, 33.9%) were the most common factors; thyroid disorders presented predominantly with hypothyroidism profile (19.3%), less often with hyperthyroidism (9.7%) or thyroid goitre with euthyroidism (4.9%).
Seven patients had a diagnosis of autoimmune disease: Polymyalgia rheumatica (PMR) was present in three cases, one had Lichen planus, one
had Ulcerative Colitis and one had Inflammatory Uveitis. In one case the diagnosis was of undifferentiated connective tissue disease. Migraine was not so frequent in our study population (9 pts, 14.5%).
Among gender-related NT-RF, a stressful condition, - emotional or physical - immediately preceding the period of the acute event was reported in more than half of patients (35 pts, 56,5%). Emotional distress and anxiety symptoms were present in 11%, whereas depression symptoms were found in 8% of the patients, in line with prior series.
When considering the SCAD clinical presentation, non-ST-segment elevation myocardial infarction was more frequent (43 pts, 72.6%) in comparison to ST-segment elevation (17 pts, 27.4%). Ventricular fibrillation was the first clinical presentation in three patients (4.9%) and cardiac arrest with pulseless electrical activity (PEA) in only one patient (1.6%). Mean left ventricular ejection fraction (LVEF) at SCAD diagnosis was 55% (IQR 55-60). Only 8 patients (12.9%) had a left ventricular dysfunction (LVEF < 50 p=0.010).>
Among patients who underwent a vascular exam by either computer tomography or magnetic resonance imaging, a total of 7 patients out of 23 (30.4%) were diagnosed with fibromuscular dysplasia (FMD). The majority of patients (60 pts) with SCAD were managed conservatively. Three patients had Drug eluting Stent (DES) implantation. No one needed CABG. All patients received dual antiplatelet therapy at discharge, mainly with the combination of ASA and clopidogrel (54%) or ASA and ticagrelor (35%) (Table 2).
Analysis of traditional and non-traditional risk factors
Patients who presented at least one of the non-traditional risk factors were allocated to the NT-RF SCAD group (n = 51), in the absence of these characteristics, patients were allocated to the T-RF SCAD group (n = 11) (Table 2). Patients in the NT-RF SCAD group compared with the T-RF SCAD group were younger (mean age 53 vs 66; p=0.027) and predominantly females (48 vs 7 pts, p=0.004).
Among T-RF, hypertension, diabetes, smoking and family history of CAD were comparable in both groups, except for dyslipidemia, which was significantly less frequent in patients with non-traditional risk factors (p=0.016). No difference in clinical presentation, incidence of FMD, peripheral arterial disease (PAD) and chronic kidney disease (CKD) was found between the two groups. In the majority of the NT-RF population was seen a Type 2 Yip/Saw angiographic phenotype (63%), with significantly higher prevalence than in the nT-RF (p=0.035). No differences in prescribed therapy at discharge were observed.
Follow up and clinical outcomes results
Clinical outcomes at a median follow-up of 23 months (interquartile range: 11;57) are shown in Table 3. MACE occurred in 17.7% of patients of the overall study population: two deaths (3,2%) and nine acute myocardial infarction (AMI). There were no in-hospital deaths. No one patient had stroke or TIA. Five patients (8%) had SCAD recurrence, mainly involving different coronary territories compared to the previous episode (4/5 events). When comparing the incidence of cardiovascular events in the 2 study groups there was no difference in the prevalence of MACES in both groups (NT-RF SCAD 19.6% - T-RF SCAD 9.1%; chi2 p=0.4); no differences in the individual components of the composite endpoint was also seen. At univariate Cox regression analysis, a history of previous SCAD (HR 11.580, CI 95% [3.091; 43.374], p < 0 p=0.555]>(Figure 4) .
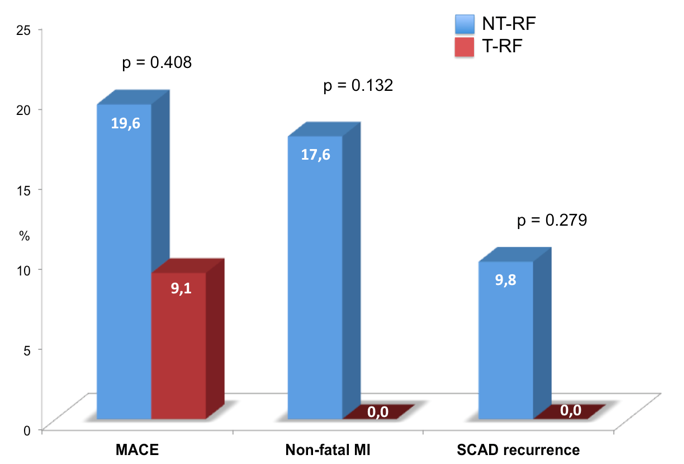
Figure legend:
NT-RF: non traditional risk factors; T-RF : traditional risk factors; MACE : major adverse cardiovascular events; MI : myocardial infarction
SCAD : spontaneous coronary artery dissection
* We created this figure for this article; it is not based on any previously published image. Copyright will belong to Journal of Clinical Cardiology and Cardiovascular Intervention, but substantial rights for future use are granted back to the author.
Figure 3: Histogram of MACEs with single endpoints
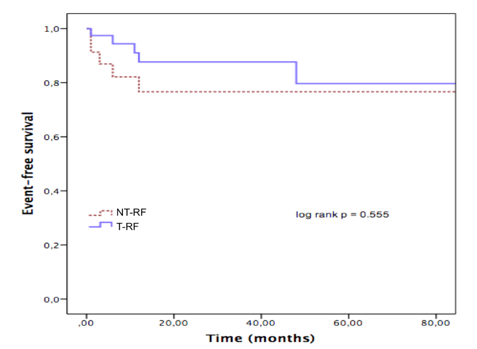
Figure legend: NT-RF: non traditional risk factors; T-RF traditional risk factors
* We created this figure for this article; it is not based on any previously published image. Copyright will belong to Journal of Clinical Cardiology and Cardiovascular Intervention, but substantial rights for future use are granted back to the author.
Figure 4: Event free survival in the two study groups : NT-RF non traditional risk factors and T-RF traditional risk factors
Presence of non-traditional risk factors
One main finding of our study is that NT-RF are common in the SCAD population, especially in younger female patients. Although coronary atherosclerotic disease remains the main cause of ACS, SCAD is more prevalent than previously reported in the literature, especially in young and middle-aged women. Early detection is important, not only because the therapeutic approach is generally less-invasive and may differ from the usual treatment of atherosclerotic ACS, but also because the malignant form that can sometimes underlie SCAD involves cardiac arrest.
The still present age and sex bias in the evaluation of chest pain suggests that younger patients (particularly female) may be referred for coronary disease evaluation much later as men or even being misdiagnosed as having non-cardiac symptoms. [27]
This may be related in part to the erroneous perception that coronary disease will not affect the young and otherwise healthy the more so in the absence of a “traditional risk profile”. In fact, SCAD needs to be suspected in every young woman presenting with ACS without traditional cardiovascular risk factors.
On the other hand, the relevance of SS-NT-RF in SCAD pathogenesis should be acknowledged, especially the role of female sexual hormones: young or middle-aged women who present with symptoms suggestive of ACS should be asked not only about pregnancy and their menstrual history, but also about therapies modulating female sexual hormones. To date, it is unknown whether the absolute levels and/or fluctuations in circulating estrogen and progesterone impact the process. [28]
As can be seen from the data derived from our registry, these young women who have been hospitalized for a SCAD frequently had a previous diagnosis of gynecological pathology or hormonal therapy in their medical history.
Among GR-NT-RF in our study population, the frequency of patient-reported stressors prior to SCAD AMI was very high (64.5%), and more than twice as high as in other ACS cohorts. [18]
Migraine was uncommon in our study population, which is in contrast to a recent Mayo Clinic series of 586 SCAD patients of mostly women with a 40% lifetime and 27% 1-year prevalence of migraine. [29]
Those with migraines reported more anxiety, depression, chest pain, and concern for future SCAD events. [30] However, one must be careful before reporting causality for these associations due to the lack of objective data as to magnitude of the precipitant exposure and the effect of recall bias, especially because many SCAD studies utilize retrospective surveys.
In the scientific literature patients with SCAD are four times more likely to have coronary artery tortuosity and extracoronary vascular arteriopathies (EVAs) such as dilatation, tortuosity, aneurysm, dissection in comparison with matched controls; fibromuscular dysplasia (FMD) was found in > 60% when assessed systematically, highlighting the importance of screening of the entire population who received a diagnosis of SCAD. [31] In our study group we found an incidence of coronary artery fibromuscular dysplasia (FMD) in 30% of the screened cases (Table 2).
Lack of traditional risk factors
Another major finding was that traditional risk factors for atherosclerosis were not common, except for hypertension, in our registry (Table 1, Table 2). In two recent series with > 300 SCAD patients each, diabetes mellitus was present in only 0.9% to 4.6%, smoking in 0.6% to 10%, hypertension in 27% to 36%, and mean body mass index was 24 kg/m. [11,15]
This strong association with hypertension may partly be explained by the higher prevalence in the general population. Another reason that may explain this association is the increase in shear stress on the vessels imposed by high systolic arterial pressure and pulsatory pressure which seems likely to be the main pathophysiological mechanism by which SCAD occurs.
Of note some of psycho-social factors that disproportionally more often affect women, may act not only through a direct mechanism, but also indirectly be related to more patients being smokers, have hypertension and abdominal obesity.
In line with this, when comparing patients with prevalent NT risk profile with patients with T risk factors two different profiles could be observed: one group of patients with non-traditional risk factors (NT) and a second group, less numerous, without these characteristics (T). The NT-RF group included significantly more younger women (Table 2). This reflects the distribution of non-traditional risk factors in the general population, where for younger women autoimmune diseases, connective tissue diseases and gynecological diseases related to pregnancy predominate, the latter being the exclusive prerogative of the female sex only.
Of note, in the NT-RF group the prevalence of dyslipidemia was low and significantly lower in comparison with the T-RF group (Table 2). This clear difference could even explain a different pathogenesis of the disease: in the NT-RF group, the loss of vascular integrity and the increase in shear stress would prevail. In the group with T-RF, which have a higher prevalence of dyslipidemia, the cause may be more similar to the pathogenesis of atherosclerotic plaque or be related to it, but not visible with the current diagnostic methods available.
This hypothesis was further supported by the finding that the diffuse smooth stenosis pattern (type 2) was the most common angiographic manifestation of SCAD in our population and its prevalence was even higher in patients with NT-RF in comparison with T-RF population (Table 2). Moreover, the Angio-Type 2 second Yip/Saw, rather than other phenotypes, is more often correlated with the intrinsic frailty and vulnerability of the arterial wall and with the predisposition of the vasa vessels to disrupt in the context of the hormonal/autoimmune vascular changes occurring in the NT-RF population.

Legend to table:
NT: Non-Traditional Risk Factors; IQR: Inter Quartile Range; CKD: Chronic Kidney Disease; T-RF: Traditional Risk Factors; CAD: Coronary Artery Disease; BMI: Body Mass Index; SD: Standard Deviation; STEMI: ST-segment Elevation Myocardial Infarction; NSTEMI: NON-ST segment Elevation Myocardial Infarction; NOAC: New Oral Anticoagulant; ASA: Cardioaspirin; EF: Ejection Fraction; LAD: Left Atrial Descending; CFx: Circumflex; RCA: Right Coronary Artery; PCI-DES: Percutaneous Coronary Intervention – Drug Eluting Stent; DAPT: Dual Anti-Platelet therapy; SAPT: Single Anti-Platelet therapy
Table 2: Clinical, echocardiographic and angiographic features in the total population and in the two groups: NT-RF = non-traditional risk factors, T-RF= traditional risk factors Significant results are marked in bold
Finally, we found that the NT-RF population had a trend towards a higher risk of recurrence (9,8% for NT-RF vs 0% for T-RF).
SCAD is a serious disease with an increased risk of recurrences
Although ACS is the predominant manifestation of SCAD, patients may also present with atypical symptoms and unstable angina which further complicates the diagnosis. In our series, no women presented to the emergency room with symptoms of unstable angina, and ACS NSTEMI was the most frequent clinical presentation in line with other studies. Of note, the highly malignant clinical presentation of SCAD with cardiac arrest occurred in 4 patients out of 62 (Tables 1-2), 3 with VF and in one case with PEA, in line with reports of other series in which approximately 13% of patients with SCAD presented with sudden death. [5,32]
Furthermore, although in-hospital death did not occur in our population, a considerable burden of MACE was recorded during the follow-up.
Five patients (8%) had SCAD recurrence (Table 3), predominantly affecting coronary territories different to that of the previous episodes.
Characteristics
| total population (n= 62) | NT-RF population (n = 51) | T-RF population (n = 11) | p value |
MACE [n, (%)] CV death Non-fatal MI Stroke/TIA SCAD recurrence [n, (%)] | 11 (17.7) 2 (3.2) 9 (14.5) 0 (0.0) 5 (8.1) | 10 (19.6) 1 (2.0) 9 (17.6) 0 (0.0) 5 (9.8) | 1 (9.1) 1 (9.1) 0 (0.0) 0 (0.0) 0 (0.0) | 0.408 0.225 0.132 - 0.279 |
Legend to table:
MACE: Major Adverse Cardiovascular Event; CV: Cardiovascular; MI: Myocardial Infarction; TIA: Transient Ischaemic Attack; SCAD: Spontaneous Coronary Artery Dissection
Table 3: Clinical outcomes in the total population and in the two groups
Our findings are in line with data from other studies, with recurrent MI occurring in 1.6% to 18% of patients, recurrent SCAD occurring in 4.7% to 22% of patients, heart failure in 2% to 3.9% and death ranging from 0% to 3.1% (0.3%). [32]
More than half of women have recurrent chest pain, even without detectable ischemia, and the rate of recurrence of SCAD has been reported to vary between 17% at 4 years and 30% at 10 years. [14]
Our data are also in line with this finding, corroborating that SCAD is a serious disease associated with a significantly increased risk of recurrences and long-term symptomatology.
The literature indicates that the development of a non-invasive coronary imaging modality or biomarker able to diagnose SCAD non-invasively would be a great advance in the care of patients with this condition and would avoid the need for invasive coronary angiography for diagnosis. [33]
The present study has several limitations. First, it was a mixed retrospective and prospective monocentric observational study and not a randomized study. Secondly, due to the small size of the population small effects may have been overlooked. Thus, our results does not allow definitive conclusions about the predominant risk profile and prognosis of SCAD patients to drawn. Still, the results are important to generate further hypotheses and should be confirmed in larger multicentric studies.
SCAD is an emerging cause of myocardial infarction in young women without the traditional cardiovascular risk profile, therefore risk assessment may be difficult due to the scarce validity of existing prediction models. Risk models incorporating NT-RF are needed and should be used widely. Being aware of the peculiar features of this disease could help clinicians and researchers to establish targeted interventions for cardiovascular primary prevention, early diagnosis and secondary prevention in young women.
no funding to declare.
none.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
