
Research Article | DOI: https://doi.org/10.31579/2578-8965/238
1Department of Obstetrics and Gynaecology, Abia State University, Uturu, Nigeria
2Department of Obstetrics and Gynaecology, University of Port Harcourt Teaching Hospital, Rivers State, Nigeria
3Department of Medical Laboratory Science, Babcock University, Ilishan. Ogun State, Nigeria
4Department of Physiology, Abia State University, Uturu, Nigeria
5Department of Surgery, Abia State University, Uturu, Nigeria
6Department of Biochemistry, Lead City University, Ibadan, Oyo State, Nigeria
*Corresponding Author: Augustine I. Airaodion, Department of Biochemistry, Lead City University, Ibadan, Oyo State, Nigeria.
Citation: C. O. Onyemereze, F. C. Alumona, O. O. Adesina, K. K. Mba, A. I. Airaodion, et al, (2024), Assessment of Risk Factors Associated with Placenta Previa in a Tertiary Health Institution in Southeast Nigeria, J. Obstetrics Gynecology and Reproductive Sciences, 8(7) DOI:10.31579/2578-8965/238
Copyright: © 2024, Augustine I. Airaodion. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 September 2024 | Accepted: 01 October 2024 | Published: 08 October 2024
Keywords: Placenta previa; risk factors; pregnancy complications; cesarean section; multiple pregnancies; maternal health
Background: Placenta previa is a significant obstetric complication that can lead to adverse maternal and fetal outcomes. Understanding its risk factors is crucial for early diagnosis and management, particularly in healthcare settings in Nigeria.
Objective: To assess the risk factors associated with placenta previa among pregnant women in a tertiary health institution in Southeast Nigeria.
Materials and Methods: This prospective descriptive study was conducted over two years (January 2021 to December 2022) and included all pregnant women who delivered in the institution during this period. Data were collected using a structured, interviewer-administered questionnaire after obtaining informed consent from participants. Placenta previa was identified through abdominal ultrasonography, and all confirmed cases were managed according to the MacAfee regimen. Descriptive statistics and chi-square tests were used to analyze the data using SPSS version 26.
Results: Out of the 8,766 deliveries recorded in the hospital during the period of this study, 94 (1.07%) were diagnosed with placenta previa. Significant associations were found between placenta previa and factors such as advanced maternal age (≥40 years, p=0.041), history of complications during previous pregnancies (p=0.039), previous cesarean section (p=0.009), history of placenta previa (p<0.001), multiple pregnancies (p=0.001), bleeding during pregnancy (p<0.001), and uterine surgeries apart from cesarean sections (p=0.001). Smoking history was also a significant risk factor (p<0.001).
Conclusion: The study identified several risk factors for placenta previa, including advanced maternal age, previous cesarean section, history of placenta previa, multiple pregnancies, uterine surgeries, and smoking. These findings highlight the importance of targeted interventions and close monitoring of at-risk pregnant women to reduce complications.
Placenta previa, a significant obstetric complication, remains one of the leading causes of maternal morbidity and mortality worldwide. This condition is characterized by the placenta's abnormal implantation in the lower uterine segment, often resulting in painless vaginal bleeding in the second or third trimester of pregnancy [1]. It poses significant risks not only to the pregnant woman but also to the fetus, necessitating urgent medical intervention and often leading to preterm delivery or cesarean section [2].
The prevalence of placenta previa varies globally, with higher rates reported in developing countries due to differences in maternal healthcare access, socioeconomic factors, and varying degrees of awareness regarding prenatal care [3]. In Nigeria, particularly in the Southeast region, placenta previa remains a significant contributor to maternal and perinatal morbidity and mortality [4]. The region's unique demographic and cultural characteristics further compound the challenge of managing this condition effectively.
Several risk factors have been identified for placenta previa, including advanced maternal age, multiparity, history of cesarean delivery, and previous uterine surgeries, among others [5]. Advanced maternal age, particularly women over 35, has been linked to an increased risk due to degenerative changes in the uterine vasculature, which may affect placental implantation [6]. Multiparity has also been shown to be a significant risk factor, as repeated pregnancies can lead to uterine scarring and changes that predispose women to abnormal placental implantation [7].
Another crucial factor is the history of cesarean sections and uterine surgeries. Studies have demonstrated that the risk of placenta previa increases with each subsequent cesarean section due to the development of scar tissue, which may alter the normal placental implantation process [8]. This is particularly concerning in regions where cesarean delivery rates are rising, leading to an increased burden of placenta previa [9].
Lifestyle and environmental factors, such as smoking and exposure to secondhand smoke, have also been associated with placenta previa, with nicotine affecting placental development and function [10]. Additionally, multiple pregnancies, closely spaced pregnancies, and infertility treatments have been highlighted as contributing factors [11].
Despite the recognition of these risk factors, there is still limited data on the incidence and specific risk factors associated with placenta previa in Southeast Nigeria. Understanding these factors is critical for developing targeted preventive strategies and improving maternal and neonatal outcomes. The lack of comprehensive studies in this region underscores the need for research that focuses on identifying and assessing the risk factors specific to this population, as cultural, socioeconomic, and healthcare-related factors can significantly influence the incidence and management of placenta previa [12].
This study aims to fill the gap in knowledge by assessing the risk factors associated with placenta previa in a tertiary health institution in Southeast Nigeria. The findings will be instrumental in informing healthcare policies and developing intervention strategies to reduce the incidence and complications associated with placenta previa in the region.
This prospective descriptive study was carried out for two years, from January 2021 to December 2022. All pregnant women who delivered their children during the period of this study were enrolled in this study. Data were collected using a structured, interviewer-administered questionnaire. Participants were assured of the confidentiality of their responses, and data was anonymized to protect their identity. Informed consent was obtained from all participants, and they were informed of their right to withdraw from the study at any time without any consequences to their medical care.
Placenta praevia was identified via abdominal ultrasonography, revealing the placenta situated in the lower uterine section, with its lowest edge positioned beneath the dome of a distended urinary bladder. All preterm diagnoses of placenta previa were admitted and handled according to the MacAfee regimen (expectant management), with interventions implemented only at term or in the event of complications. Immediate delivery was performed in symptomatic instances endangering mother or foetal life, regardless of gestational age, as well as in cases presenting at term. In this hospital, Caesarean sections were routinely performed for all instances of placenta praevia, with the diagnosis confirmed intraoperatively. The collected data was analyzed using the Statistical Package for Social Sciences (SPSS) version 26. Descriptive statistics such as frequencies and percentages were used to summarise the demographic characteristics and obstetrics and gynaecology history. The proportion of women diagnosed with placenta previa was calculated for prevalence assessment. Chi-square tests were used to determine associations between categorical variables such as age, parity, etc. with the prevalence of placenta previa.
During the period of this study, a total of 8766 deliveries were recorded in this hospital. Most of them were aged 30-39 years (38.71%), with a significant number having attained secondary education (60.54%). Most respondents were married (99.14%), employed in the public sector (45.13%), and resided in urban areas (80.54%) (Table 1).
The majority had been pregnant 2-3 times (63.79%), with 36.38% having one delivery (parity). Previous pregnancy complications were reported by 8.16%, with premature birth being the most common complication (57.06%). Cesarean sections were reported by 34.33%, and a small proportion (0.44%) had a history of placenta previa, mostly diagnosed in the third trimester (71.79%) (Table 2). Regular antenatal care attendance was high (90.88%), with most participants satisfied with the information provided (42.43%). Only 11.34% reported challenges in accessing antenatal care (Table 3).
Only 1.07% of the women experienced placenta previa, indicating a relatively low occurrence (Figure 1). Most participants were non-smokers (96.55%), did not consume alcohol (93.82%), and did not have a history of hypertension (96.22%) (Figures 2-4). Significant associations were found with factors like age (p = 0.041), parity (p = 0.005), history of pregnancy complications (p = 0.039), cesarean section (p = 0.009), history of placenta previa (p = 0.000), multiple pregnancies (p = 0.001), bleeding during pregnancy (p = 0.000), uterine surgery (p = 0.001), smoking status (p = 0.000), and fibroid diagnosis (p = 0.011).
| Socio-Demographic Information | Frequency (n = 8766) | Percentage (%) |
| Age (in Years) | ||
| Below 20 | 362 | 4.13 |
| 20-29 | 2896 | 33.04 |
| 30-39 | 3393 | 38.71 |
| 40 and above | 2115 | 24.13 |
| Educational Level | ||
| No formal Education | 18 | 0.21 |
| Primary Education | 126 | 1.44 |
| Secondary Education | 5307 | 60.54 |
| Tertiary Education | 3315 | 37.82 |
| Marital Status | ||
| Single | 31 | 0.35 |
| Married | 8691 | 99.14 |
| Divorced/Widowed | 44 | 0.50 |
| Employment Status | ||
| Unemployed | 334 | 3.81 |
| Self-employed | 2495 | 28.46 |
| Private sector employee | 1854 | 21.15 |
| Public sector employee | 3956 | 45.13 |
| Student | 127 | 1.45 |
| Residence | ||
| Rural | 1706 | 19.46 |
| Urban | 7060 | 80.54 |
Table 1: Socio-Demographic Information of Participants
| Variable | Frequency (n = 8766) | Percentage (%) |
| How many times have you been pregnant including this present one (Gravida)? | ||
| 1 | 1893 | 21.59 |
| 2-3 | 5592 | 63.79 |
| 4-5 | 834 | 9.51 |
| More than 5 | 447 | 5.10 |
| How many deliveries have you had (Parity)? | ||
| None | 1912 | 21.81 |
| 1 | 3189 | 36.38 |
| 2-3 | 3127 | 35.67 |
| 4 or more | 538 | 6.14 |
| Did you experience any complications during previous pregnancies? | ||
| Yes | 715 | 8.16 |
| No | 6158 | 70.25 |
| Not Applicable | 1893 | 21.20 |
| If yes, please specify | ||
| Pre-eclampsia | 217 | 30.35 |
| Placenta previa | 11 | 1.54 |
| Premature birth | 408 | 57.06 |
| Others | 79 | 11.04 |
| Have you ever had a Cesarean section? | ||
| Yes | 3009 | 34.33 |
| No | 5757 | 65.67 |
| If yes, how many times? | ||
| 1 | 1674 | 55.63 |
| 2-3 | 1324 | 44.00 |
| More than 3 | 11 | 0.37 |
| Have you had any previous miscarriages? | ||
| Yes | 811 | 9.25 |
| No | 7955 | 90.75 |
| Do you have a history of placenta previa in previous pregnancies? | ||
| Yes | 39 | 0.44 |
| No | 8727 | 99.56 |
| At what gestational age were you diagnosed with placenta previa (if applicable)? | ||
| First trimester | 00 | 0.00 |
| Second trimester | 11 | 28.21 |
| Third trimester | 28 | 71.79 |
| Have you ever had multiple pregnancies (twins, triplets, etc.)? | ||
| Yes | 1719 | 19.61 |
| No | 7047 | 80.39 |
| Have you experienced any bleeding during this pregnancy? | ||
| Yes | 683 | 7.79 |
| No | 8083 | 92.21 |
| Do you have a history of diabetes (gestational or otherwise)? | ||
| Yes | 561 | 6.40 |
| No | 8205 | 93.60 |
| Have you ever been diagnosed with fibroids? | ||
| Yes | 1105 | 12.57 |
| No | 7661 | 87.39 |
| Have you ever had uterine surgery apart from C-sections? | ||
| Yes | 1111 | 12.67 |
| No | 7655 | 87.33 |
| Have you ever used assisted reproductive technology (e.g., IVF)? | ||
| Yes | 985 | 11.24 |
| No | 7781 | 88.76 |
| Do you have a history of anemia during pregnancy? | ||
| Yes | 1008 | 11.50 |
| No | 7758 | 88.50 |
Table 2: Obstetric and Gynecological History of Participants
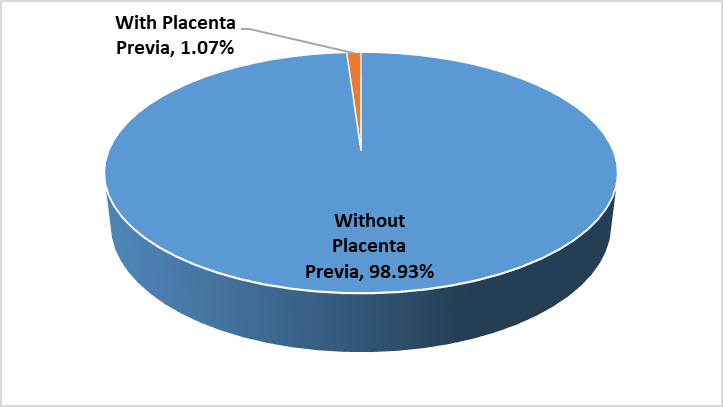
Figure 1: Occurrence of Placenta Previa.
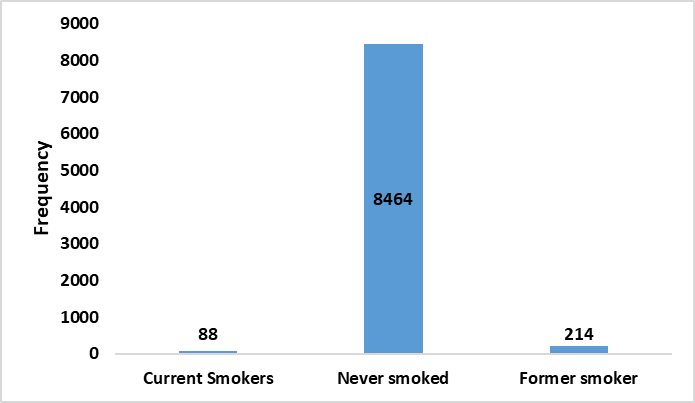
Figure 2: Smoking of Tobacco.
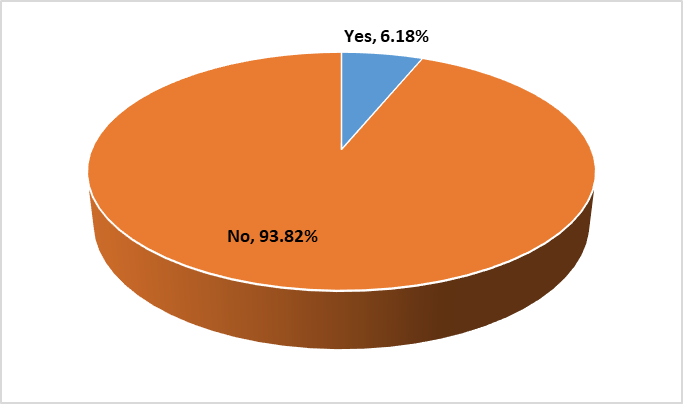
Figure 3: Consumption of Alcohol.
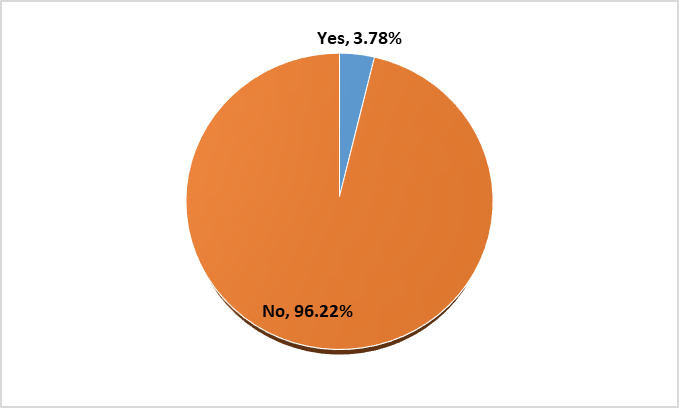
Figure 4: History of Hypertension.
| Variable | Frequency | Percentage (%) |
| How often do you attend antenatal care services during pregnancy? | ||
| Regularly (as recommended) | 7967 | 90.88 |
| Occasionally | 709 | 8.09 |
| Rarely | 90 | 1.03 |
| How satisfied are you with the information and care provided by healthcare professionals regarding pregnancy complications, including placenta previa? | ||
| Very satisfied | 2654 | 30.27 |
| Satisfied | 3719 | 42.43 |
| Neutral | 1696 | 19.35 |
| Dissatisfied | 444 | 5.07 |
| Very dissatisfied | 253 | 2.89 |
| Have you ever faced challenges in accessing antenatal care or ultrasound scans during pregnancy? | ||
| Yes | 994 | 11.34 |
| No | 7772 | 88.66 |
Table 3: Healthcare Services and Accessibility
| Risk Factors | Occurrence of Placenta Previa | p-value | |
With Placenta Previa (n = 94) | Without Placenta Previa (n = 8672) | ||
| Age (in Years) | 0.041* | ||
| Below 20 | 00 (0.00%) | 362 (100.00%) | |
| 20-29 | 00 (0.00%) | 2896 (100.00%) | |
| 30-39 | 21 (0.62%) | 3372 (99.38%) | |
| 40 and above | 73 (3.45%) | 2042 (96.54%) | |
| How many times have you been pregnant including this present one (Gravida)? | 0.216 | ||
| 1 | 22 (1.16%) | 1871 (98.84%) | |
| 2-3 | 32 (0.57%) | 5560 (99.43%) | |
| 4-5 | 20 (2.40%) | 814 (97.60%) | |
| More than 5 | 20 (4.47%) | 427 (95.53%) | |
| How many deliveries have you had (Parity)? | 0.005* | ||
| None | 00 (0.00%) | 1912 (100.00%) | |
| 1 | 00 (0.00%) | 3189 (100.00%) | |
| 2-3 | 37 (1.18%) | 3090 (98.82%) | |
| 4 or more | 57 (10.59%) | 481 (89.41%) | |
| Did you experience any complications during previous pregnancies? | 0.039* | ||
| Yes | 33 (4.62%) | 682 (95.38%) | |
| No | 61 (0.99%) | 6097 (99.01%) | |
| Not Applicable | 00 (0.00%) | 1893 (100.00%) | |
| Have you ever had a Cesarean section? | 0.009* | ||
| Yes | 89 (2.96%) | 2920 (97.04%) | |
| No | 5 (0.09%) | 5752 (99.91%) | |
| Have you had any previous miscarriages? | 0.062 | ||
| Yes | 2 (0.25%) | 809 (99.75%) | |
| No | 92 (1.16%) | 7863 (98.84%) | |
| Do you have a history of placenta previa in previous pregnancies? | 0.000* | ||
| Yes | 39 (100.00%) | 00 (0.00%) | |
| No | 55 (0.63%) | 8672 (99.37%) | |
| Have you ever had multiple pregnancies (twins, triplets, etc.)? | 0.001* | ||
| Yes | 91 (5.29%) | 1628 (94.71%) | |
| No | 3 (0.04%) | 7044 (99.96%) | |
| Have you experienced any bleeding during this pregnancy? | 0.000* | ||
| Yes | 69 (10.10%) | 614 (89.90%) | |
| No | 25 (0.31%) | 8058 (99.69%) | |
| Have you ever had uterine surgery apart from Cesarean sections? | 0.001* | ||
| Yes | 74 (6.67%) | 1037 (93.33%) | |
| No | 20 (0.26%) | 7635 (99.74%) | |
| Have you ever used assisted reproductive technology (e.g., IVF)? | 0.511 | ||
| Yes | 15 (1.52%) | 966 (98.07%) | |
| No | 79 (1.01%) | 7702 (98.93%) | |
| Do you smoke or have you ever smoked? | 0.000* | ||
| Current Smokers | 62 (70.45%) | 26 (29.55%) | |
| Never smoked | 00 (0.00%) | 8464 (100.00%) | |
| Former smoker | 32 (14.95%) | 182 (85.05%) | |
| Do you consume alcohol? | 0.614 | ||
| Yes | 7 (1.29%) | 535 (98.71%) | |
| No | 87 (1.06%) | 8137 (98.94%) | |
| Do you have a history of hypertension? | 0.594 | ||
| Yes | 4 (1.21%) | 327 (98.79%) | |
| No | 90 (1.07%) | 8345 (98.93%) | |
| Have you ever been diagnosed with fibroids? | 0.011* | ||
| Yes | 66 (5.97%) | 1039 (94.03%) | |
| No | 28 (0.37%) | 7633 (99.63%) | |
Table 4: Risk Factors associated with Placenta Previa
This study assessed the risk factors associated with placenta previa among pregnant women attending a tertiary health institution in Southeast Nigeria. The majority of participants (38.71%) were aged 30–39 years, with only 4.13% being below 20 years. Notably, the occurrence of placenta previa was significantly higher in women aged 40 and above (3.45%) compared to other age groups (p = 0.041). This aligns with the findings of Srisupundit et al. [13], who reported that advanced maternal age is a significant risk factor for placenta previa. The higher risk among older women could be attributed to increased parity and uterine scarring from previous pregnancies [14].
In terms of educational level, a majority (60.54%) had secondary education, and 37.82% had tertiary education. However, there was no significant association between education level and placenta previa occurrence. Similarly, marital status did not show any substantial link with placenta previa, as nearly all participants (99.14%) were married. This finding differs from previous research by Sekiguchi et al. [15], which found that single women were more likely to experience placenta previa. This variation could be due to cultural differences and the predominance of married women in this study population.
The study revealed that multiparity (having 4 or more deliveries) was a significant risk factor for placenta previa (p = 0.005), with a prevalence of 10.59% among women with 4 or more deliveries. This finding aligns with the results of Adekanle and Adeyemi [16], who indicated that multiparity is a strong predictor of placenta previa. The higher risk could be due to repeated stretching and scarring of the uterine lining, which may predispose women to abnormal placental attachment [17].
A history of previous cesarean sections was another significant risk factor, as women with prior C-sections had a 2.96% occurrence of placenta previa (p = 0.009). This result supports the findings of Silver [18], who reported a strong association between cesarean deliveries and subsequent placenta previa due to scar formation in the uterus. Additionally, the study found that a history of placenta previa in previous pregnancies was a strong predictor of recurrence, with 100% of those with a previous history experiencing it again (p = 0.000). This is consistent with the study by Cunningham et al. [19], which indicated that women with a history of placenta previa have a tenfold increased risk of recurrence.
The occurrence of placenta previa was also significantly associated with multiple pregnancies (p = 0.001), as 5.29% of women with twins or triplets experienced placenta previa. This finding corresponds with the research of Jauniaux et al. [20], who noted that multiple gestations are linked to an increased risk of placenta previa, possibly due to an increased placental surface area required to support the pregnancy.
The study found that smoking was significantly associated with placenta previa (p = 0.000), with 70.45% of current smokers experiencing placenta previa. This aligns with the findings of Salihu et al. [21], who established that smoking increases the risk of placenta previa by up to fourfold, likely due to the vasoconstrictive effects of nicotine, which can affect placental implantation.
A history of fibroids was another significant risk factor, with 5.97% of women with fibroids experiencing placenta previa (p = 0.011). This finding is consistent with the study by Masukume et al. [22], which demonstrated that fibroids could interfere with normal placental implantation, leading to an increased risk of placenta previa.
In contrast, factors such as alcohol consumption and hypertension were not significantly associated with placenta previa in this study, which differs from some previous studies [23]. The lack of a significant association in this population might be due to the lower prevalence of these conditions among the study participants.
The majority of participants (90.88%) regularly attended antenatal care services, which is encouraging. However, the occurrence of placenta previa among women who attended antenatal care regularly suggests that early detection and management strategies should be enhanced. This finding is in line with the study by Fausett and Saade [24], which emphasized the importance of regular antenatal care in reducing the complications associated with placenta previa.
This study identified advanced maternal age, multiparity, previous cesarean sections, history of placenta previa, multiple pregnancies, smoking, and fibroids as significant risk factors for placenta previa. These findings are consistent with many previous studies, though some differences were observed, possibly due to variations in population characteristics and healthcare practices. Early detection and targeted interventions for high-risk women could help reduce the incidence and complications associated with placenta previa in Southeast Nigeria.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
