
Research Article | DOI: https://doi.org/10.31579/2640-1045/114
1Assistant Professor, Department of Pathology, Gazi Medical College, Khulna, Bangladesh.
2Associate Professor, Department of Laboratory Medicine, Bangabandhu Sheikh Mujib Medical University.
3Pathology Resident, Dhaka Medical College.
4Associate Professor, Department of Pharmacology & Therapeutics, Gazi Medical College, Khulna, Bangladesh
5Assistant Professor, Department of Laboratory Medicine, Bangabandhu Sheikh Mujib Medical University.
6Lecturer, Department of Pathology, National Institute of Ophthalmology & Hospital.
7MS in Microbiology, Bangladesh University of Health Sciences.
8Professor, Department of Laboratory Medicine, Bangabandhu Sheikh Mujib Medical University.
*Corresponding Author: Mesbah Uddin Ahmed, 7MS in Microbiology, Bangladesh University of Health Sciences, Bangladesh.
Citation: T Rahman,S Islam, A Ferdous, B Islam, Mesbah U Ahmed, et al. (2022). Assessment of Fatty Liver Diseases Based on Serum Ck-18 Fragment, Gamma Glutamyl Transferase and Aspartate Aminotransfease /Alanine Aminotransferase Ratio. Endocrinology and Disorders. 6(1): DOI:10.31579/2640-1045/114
Copyright: © 2022 Mesbah Uddin Ahmed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 November 2021 | Accepted: 28 December 2021 | Published: 05 January 2022
Keywords: serum CK-18 fragment level; gamma glutamyl transferase level; nonalcoholic fatty liver disease
Background: Nonalcoholic fatty liver disease (NAFLD) is a serious clinical problem because of its worldwide distribution and potential adverse sequel. The global prevalence of NAFLD is increasing gradually. NAFLD can be estimated by both invasive and non-invasive methods.
Objective: The aim of this study was to determine the role of serum cytokeratin-18 (CK-18) fragment, gamma glutamyl transferase (GGT) and aspartate aminotransfease (AST)/alanine aminotransferase (ALT) ratio (AAR) in the assessment of different types of NAFLD patients especially NASH.
Methods: This cross sectional study was conducted in the Department of Clinical Pathology, Bangabandhu Sheikh Mujib Medical University. Forty patients who fulfilled the criteria of NAFLD were enrolled in this study. Serum CK-18 fragment level was measured by enzyme linked immune sorbent assay (ELISA) method. Serum gamma glutamyl transferase (GGT) and aspartate aminotransfease (AST)/alanine aminotransferase (ALT) ratio (AAR) reports were collected from patient’s file. Biopsy material was sent to the Department of Pathology, BSMMU for complete histopathological examination.
Results: Positive and significant co-relation was found between serum CK-18 fragment with NAS whereas positive but not significant correlation was seen between serum GGT and NAS and negative and not significant correlation was found between serum (AAR) and NAS.
Conclusion: Serum CK-18 fragment level may be used for assessing NASH in NAFLD patients.
Nonalcoholic fatty liver disease (NAFLD) is one of the common forms of chronic liver diseases [1]. It is currently estimated that the global prevalence of NAFLD is one billion [1]. This prevalence is increasing gradually which will become the major economic burden [2, 1]. In a study Nonalcoholic steatohepatitis (NASH) was observed in 42.4% of NAFLD cases in Bangladesh [3]. Histologically nonalcoholic fatty liver disease is classified into nonalcoholic fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH) [4]. Among them NASH may be present in one third of NAFLD [5]. Nonalcoholic steatohepatitis is a potentially serious condition. The prevalence of NAFLD is 15% in Asian population and 20 to 30% in United States [6]. It is thought to be the hepatic manifestation of metabolic syndrome [7]. The detection of CK18 fragment can differentiate NASH from NAFL or simple steatosis in this way.
The research protocol of this study was approved by the Ethical Institutional Review Board of BSMMU, Dhaka prior to the commencement of it. This cross sectional study was conducted in the Department of Clinical Pathology, in collaboration with Department of Hepatology and Department of Pathology, in Bangabandhu Sheikh Mujib Medical University, Dhaka from March’ 2014 to February’ 2015. 40 NAFLD patients of above 18 years old ages of both sexes who admitted in the Department of Hepatology were included in the study. Patients having history of alcoholism more than 210gm/wk for male and 140gm/wk for female, any condition like decompensated cirrhosis of liver, infected with hepatitis B and C virus infection, drug induced fatty liver, hepatocellular carcinoma, autoimmune liver diseases, hemochromatosis, wilson’s disease and patients with hypothyroidism were excluded from the study. Total NAFLD patients were divided into three groups according to the NAFLD activity score (NAS); NASH Clinical Research Network histological scoring system which is based on histopathological examination [8]. After taking informed written consent, a careful history was taken and the detailed information was recorded by the investigator in a predesigned questionnaire. The serum separation, storing and ELISA procedure were done in the Clinical Pathology Department, BSMMU. CK-18 fragment level is measured by Enzyme linked Immuno Sorbent Assay (ELISA) based on double antibody sandwich technology. Hematoxylin & Eosin and Masson’s Trichome stains were used and evaluated using NASH Clinical Research Network histological scoring system to diagnosis the NAFLD. All data were recorded systematically in a preformed data collection sheets and expressed as mean±SD. For all statistical tests we considered p value <0>
A total of 40 patients with NAFLD were included in this study. In this study, histopathology was considered as gold standard to divide the patients into 3 groups based on Nonalcoholic fatty liver disease activity score (NAS), including Group A : 1 to 2 = simple fatty liver disease; Group B: 3 or 4 = Borderline NASH Patients and Group C: 5 to 8 = Definite NASH.
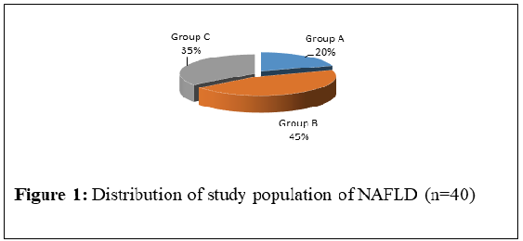
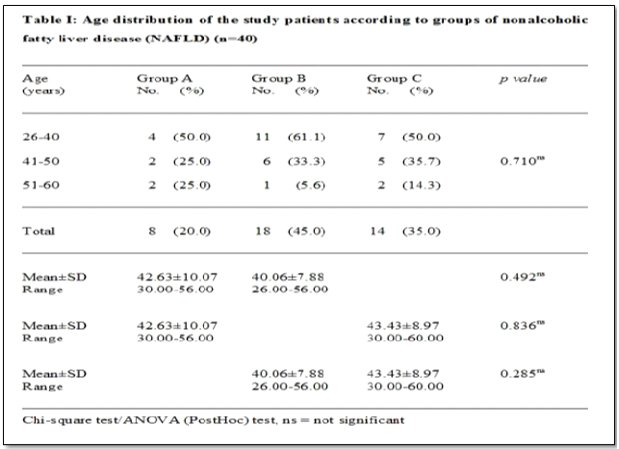

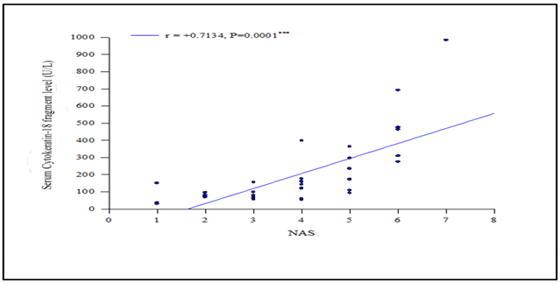
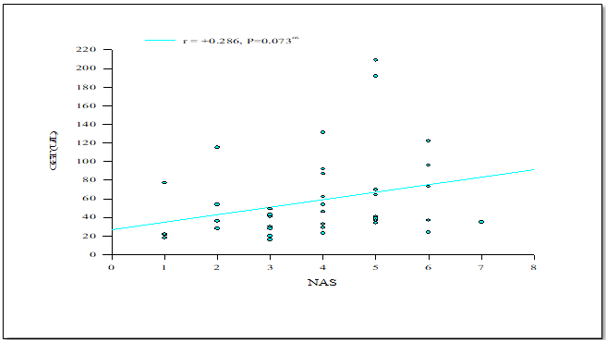
This cross sectional study was conducted in the department of Clinical Pathology in collaboration with department of Hepatology, BSMMU, Dhaka. In this study, we investigated 40 NAFLD patients who fulfilled the inclusion criteria of the study. In this study, out of 40 patients of NAFLD, histopathological examination showed that 8 (20%) patients had simple fatty liver (Gr-A), 18 (45%) had borderline NASH (Gr-B) and 14 (35%) had NASH (Gr-C). Regarding the age, in this study, out of 40 patients, the mean (±SD) age of Group A (=simple fatty liver) patients was 42.63±10.07 (range 30-56) years, Group B (= borderline diagnosis) was 40.06±7.88 (range 26-56) years and Group C (=NASH) was 43.43±8.97 (range 30-60) years. In this study, patients with NASH were found at 30-60 years age group. Alam et al. mentioned that NASH affects the population with mean age 40±9.7 with range from 30-50 of Bangladesh [3]. Aktas et al. observed that the mean age of NAFLD patients was 47±12 (years) with range from 35-59 in his study [9]. Papatheodoridis et al. showed that mean age of NASH patients in his study was 48±13 (35-61).10 Our study findings were similar with these studies. Analysis of gender distribution showed out of 40 NAFLD patients 12 were male and 28 were females. Male female ratio was 1:2∙3. Out of 8 patients of Group A, 3(37.5%) were male and 5(62.5%) were female; out of 18 patients of Group B, 4(22.2%) were male and 14(77.8%) were female; and out of 14 Group C patients, 5(35.7%) were male and 9(64.3%) were female. In this study females were predominant among three Groups. Alam et al. observed that female were predominant in NAFLD patients in Bangladesh [3]. Aida et al. also noticed female predominance in NAFLD patients in Japan [11]. Our study findings were consistent with these studies. In this study, Pearson's correlation-coefficient (r) test was performed to compare the relationship between the levels of CK-18 fragment with NAFLD Activity Score (NAS). We observed a positive correlation between GGT and NAS but not significant. Pearson’s correlation coefficient was +0.286, p lessthan 0.05. Feldstein et al., Papatheodoridis et al. and Grigorescu et al. also found no significant correlation between GGT and NAS [8,10, 12]. So, our study was consistent with these studies. In the present study, we found a negative correlation between AST-ALT ratio and NAS, not significant Pearson’s correlation coefficient was -0.133, (p lessthan 0.05). In the study Feldstein et al. there was also no significant correlation found between AST-ALT ratio and NAS [8]. This finding supported our study.
Our data revealed that there was statistically significant correlation between serum CK-18 fragment level with different types of NAFLD whereas, serum GGT and ALT-AST ratio were not significant statistically. In this aspect, we concluded that Serum CK-18 fragment level can be used for early detection, reduce progression, assessment of the prognosis of NASH in NAFLD patients.
Authors of this study are thankful to the authority of the Department of Hepatology, BSMMU, Department Pathology, BSMMU and the Department of Clinical Pathology, BSMMU, for their nice cooperation during sample collection, laboratory procedure and also thankful to the study subjects for their active and enthusiastic participation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
