
Research Article | DOI: https://doi.org/10.31579/IJBR-2021/052
1 Department of Institutional Research, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI
2Department of Nursing, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI
3Department of Dental Hygiene, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI
4Department of Mathematics and Engineering, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI
5Department of Biology, Chemistry, and Environmental Sciences, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI
6Department of Nutrition and Dietetics, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI
*Corresponding Author: Paul Andrew Bourne, Acting Director of Institutional Research, Northern Caribbean University, Mandeville, Manchester, Jamaica, WI
Citation: Anderson T., Jones A., Jones J., Toni-Ann Richards, Fallah J. (2022) Assessing Jamaicans Tolerance and whether this Influences Fear of Contracting the Coronavirus Disease 2019. International J. of Biomed Research. 2(5): DOI: 10.31579/IJBR-2021/052
Copyright: © 2022, Paul Andrew Bourne, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 January 2022 | Accepted: 07 February 2022 | Published: 27 April 2022
Keywords: tolerance; fear; COVID-19; jamaicans
Introduction: Some people cannot tolerate certain living conditions, resulting in their fear of the outcome of life.
Objective: The purpose of this study was to assess: 1) The degree of tolerance of certain living conditions among Jamaicans during the COVID-19 pandemic, 2) Identify the level of fear among Jamaicans of contracting COVID-19, and 3) Ascertain whether their degree of tolerance affected their fear of contracting COVID-19.
Methods: A quantitative research method design served to address the research objective. Using a convenience sampling method, the study population consisted of 1093 persons who participated in the study from different parishes across Jamaica. Researchers used Google Forms to collect the data, which was transferred to Statistical Packages for the Social Sciences (SPSS) for Windows version 25.0 for further data analysis.
Findings: Jamaicans moderately tolerate during the COVID-19 pandemic ((42.8±10.3, 95%CI: 42.2-43.4, out of 75.0), with Kingston and St. Andrew parish accounting for 50% (n=98) of the respondents. Most of the sampled respondents fear contracting COVID-19 (n=559), while those who are not fearful were n=534 of the total respondents.
Conclusion: Although these results cannot be generalized to the larger Jamaican population, the results indicate that tolerance does affect fear, and some Jamaicans moderately tolerate COVID- 19.
According to Adolphs (2013), fear is an intervening variable between sets of context-dependent stimuli and suites of behavioural response. Fear has impacted the decision-making of many persons. Likewise, persons cannot tolerate certain living conditions, and as such, they fear the unknown. A study was conducted to identify predictors of fear of the coronavirus three days after the World Health Organization declared a pandemic between March 14 and 17, 2020 (Blakey & Abramowitz, 2017). The results from this survey replicated findings from earlier studies. Results indicated that the 2009–2010 Swine flu pandemic and the 2015–2016 Zika virus outbreak caused fear among the affected population (Blakey & Abramowitz, 2017; Wheaton et al., 2012).
Similarly, in another study, health anxiety was related to increased fear of the current coronavirus pandemic. Furthermore, findings supported earlier reports that more media exposure is related to fear (Mertens et al., 2020). So how do people cope amid situations such as a pandemic? Does fear impede their ability to develop effective coping mechanisms? Do they become tolerant if they feel helpless in such stressful circumstances?
Tolerance is perceived as an attitude that implies accepting differences in beliefs and lifestyle and civilized behaviour with other people (Mahapatra, 2018). Since 2020, COVID-19 has changed people’s lives and the world (Haktanir, 2021). CDC (2019) states that COVID-19 is a dangerous disease caused by a virus discovered in December 2019 in Wuhan, China. It is highly contagious and is a pandemic. The virus mainly causes respiratory symptoms commonly associated with a cold, pneumonia, or flu. COVID-19 can also have adverse effects on other parts of the body and immunocompromised individuals as most at risk of complications, including death. Since the onset of the virus, the fear of contracting the coronavirus has been a constant struggle for numerous individuals worldwide. The purpose of this study is to assess Jamaican’s tolerance and whether this tolerance influences their fear of contracting COVID-19.
Theories help to explain facts, aids in understanding the natural world, and enable the prediction of the unknown based on what is trustworthy or known. Theories are either scientific or non-scientific (American Museum of Natural History, 2021). A theoretical framework supports theories and consists of concepts, definitions of concepts. Researchers demonstrate an understanding of theories and concepts relevant to their study through theoretical frameworks, enabling them to add to the body of knowledge in a particular field. This current study used the “Protection and Motivation” theory as a part of the theoretical framework for the analysis.
Rogers’ protection motivation theory (PMT, 1975, 1983) explains individual motivation to react to threats to protect themselves or others. This theory is a popular framework that explains specific responses to various triggers that inform individuals of possible threats. Lippke and Plotnikoff (2009) expanded on the PMT, integrating it into the Transtheoretical Model (TTM), introducing stages to explain why persons develop protection motivation. Furthermore, it explains the role fear plays in the decision-making process and the course of action regarding health and wellness. The concepts of fear, risk as a factor for motivation, and coping assessment are constructs addressed in the theory. The PMT consists of two appraisals: threat appraisal and coping appraisal. This current study focuses on the coping appraisal that consists of three constructs. These three constructs are:
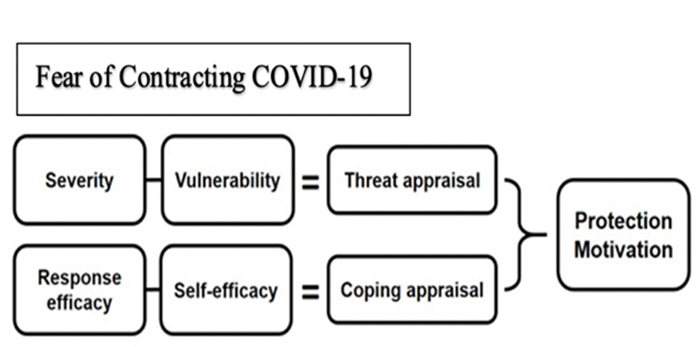
The nature of personal beliefs is expounded upon. For example, fear is manifested from the perceived severity of a health condition the patient might have. Some disease states are perceived as highly threatening (stroke, cancer), while others are not so concerning (weight gain). The patient is more likely to develop motivation depending on the severity of the health risk factor. However, vulnerability plays a role in the longevity of these developments. Therefore, risk assessment depends on severity and vulnerability.
The current COVID-19 pandemic in Jamaica in March 2020 caused various new measures and protocols. With the implementation of these new measures, we aim to determine the effects on tolerance level and how it influences the fear of Jamaicans in contracting the COVID-19 disease. The PMT underpins the constructs of this research since the idea includes fear as part of its framework. This current research will focus on the preventative measures of wearing face masks, hand sanitizing, vaccination, and social distancing. Based on the PMT, current researchers anticipate that persons will make risk assessments during the decision-making process and apply one or more preventative measures to allying fears they have toward contracting COVID-19. However, Milne et al. (2002) contend that fear rarely changes behaviour. This current study will focus on the response efficacy aspect of the PMT to assess the recent recommendations by government and public health and safety officials.
This study assesses Jamaican’s tolerance and whether the degree of tolerance influences their fear of contracting the Coronavirus disease. The study highlights the degree of tolerance among Jamaicans during the COVID-19 pandemic, how fearful Jamaicans are in acquiring COVID-19, and whether their degree of tolerance affects the fear of contracting COVID-19.
For the past year and a half, “COVID-19” has wreaked havoc globally. COVID-19 has by far been the number one topic worldwide. The resulting devastation has constantly been in the mainstream and social media platforms. The virus’s devastating number of deaths and fear continue to affect the world population. From the onset, COVID-19 was accompanied by a fear of avoiding it at all costs. For example, disease expert Charles CHIU stated that this new virus spreading in China is “definitely something to worry about” (Bai Nina, 2020). In one study, more than one-third out of 207,341 persons reported fear of contracting COVID-19. COVID-19 has caused people to face multiple stressful challenges, some driven by fear. This state of being can be extremely overwhelming on a person’s tolerance and ability to cope. Furthermore, people’s general level of risk tolerance is more predictive of COVID-19 fear. Some researchers found a growing incidence of “mental and physical exhaustion surrounding the COVID-19 pandemic. Furthermore, they contend that as a result, most individuals practice less caution as the pandemic lingers compared to the first outbreak (Haktanir, 2021).
Coelho et al. (2020) identified predictors of fear of the Coronavirus three days after the World Health Organization (WHO) declared the coronavirus outbreak a pandemic between March 14 and 17, 2020. The results support earlier studies on the 2009–2010 Swine flu pandemic (Blakey & Abramowitz, 2017) and the 2015–2016 Zika virus outbreak (Wheaton et al., 2012). These studies found that health anxiety was related to increased fear (Blakey & Abramowitz, 2017; Wheaton et al., 2012). This would be the current case seen in society about the current Coronavirus pandemic. Mertens et al. (2020) argued that more media exposure is related to fear.
According to Coelho et al. (2020), precise reports and estimates on the mortality rate are hard to conduct because many infected persons are asymptomatic. Furthermore, people interact without knowing who may be infected, adding ambiguity and creating uncertainty intolerance. Uncertainty intolerance is associated with fear caused by the acute perception of the unknown (Carleton, 2016). One of the issue relating to COVID-19 is its uncertainty relating to life, death, and treatment, and as such explains people’s reluctance not to be continuously thinking about it, which may harm the well-being of an individual owing to the predominant focus on negative emotions (McEvoy, et al., 2019; Nall, 2018; Robinson & Smith, 2021; Testoni, et al., 2021; University of Illinois at Chicago, 2016). In general, individuals will certainly require some tolerance to fear, especially now.
This study has a descriptive research design, using a quantitative research approach to answer the research question “Assessing Jamaicans tolerance and whether this influences their fear of contracting the Corona Virus disease.” According to Mcleod (2021), quantitative research involves objectively collecting and analysing numerical data to describe, foretell and control the variables of interest. The goals of quantitative analysis include testing final relationships between the different variables, generalizing results to broader populations and making predictions. This method served to gather information to achieve the following research questions: What is the degree of tolerance among Jamaicans during the COVID-19 pandemic? How fearful are Jamaicans in contracting COVID-19? Does tolerance affect the fear of Jamaicans contracting COVID-19? The composition of this study is a cross-sectional study. To select the population, convenience sampling was used. Convenience sampling (also known as availability sampling) is a specific type of non-probability sampling method that relies on data collection from population members who are conveniently available to participate in the study. According to the book “Research Methods for Business Students,” Convenience sampling is a type of sampling where the first open primary data source will be used for the research without additional requirements. In other words, this sampling method involves getting participants wherever you can find them and typically wherever is convenient. In inconvenience sampling, no inclusion criteria were identified before selecting subjects.
All subjects were invited to participate. Data were collected from September 29, 2021, to November 17, 2021. The study involved data being collected from 1093 participants. The sample size was calculated based on the population size of Jamaica for the end of 2019 (i.e., 2,734,092) as showed by the Statistical Institute of Jamaica (2022), a confidence interval of 95%, and a margin of error of 2.965% (i.e., the determined sample was 1,093). It included both females and males from the fourteen parishes across Jamaica. A research team was selected and trained by a statistician/methodologist who taught research methods inclusive of ethics to the group. Each member of the research team had to successfully complete a course in Ethics from The Global Health Network before he/she was eligible to participate in the data collection phase of the project. The team members were assigned particular regions in Jamaica, and they were given a specified criteria for data collection from participants.
The participants were informed about the purpose of the study and its essence. Information obtained was kept confidential, and persons were not required to give personal information. Survey questionnaires, including twenty-two close-ended questions with the Jeffrey Simons Distress Tolerance scale, were created on Google Forms. Messages containing the link for the survey questionnaire were sent out with details of the study and instructions on social media platforms to be completed by Jamaicans eighteen years and older. The data obtained were displayed in tables, and a graph. It was further analyzed with the aid of Google form, Microsoft Office Excel, and IBM Statistical Packages for the Social Sciences (SPSS) for Windows 25, where descriptive statistics were done, which included frequencies, central tendencies, a measure of dispersion, percentages, graphs, confidence intervals, correlation, scatterplots, regression cross-tabulation, and chi-square. In addition, exploratory factor analysis was done on the tolerance index, and its suitability and appropriateness were the reason for the usage of this variable to assess tolerance among Jamaicans (Appendix).
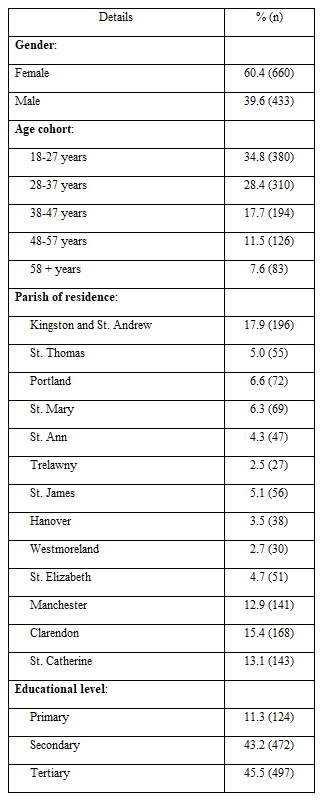
Table 1 depicts the demographic characteristics of the sampled population, such as gender, age, parish of residency, and educational level. More women (n=660, 60.4%) participated in the study compared to men (n=443, 39.6%). The majority of the study participants were between 18–27-year-old (n=380, 34.8%), followed by 28-37 years old (n=310, 28.4%). Those between the ages of 38-47 years and 48-57 years were 17.7% (n=194) and 11.5% (n=126) respectively. Those 58 years and older were 7.6% (n=83) of the total study participants. The parish of Kingston and St. Andrew had the largest number of participants at 17.9% (196), with Trelawny having the least (2.5%, n=27). The majority of participants were educated at either the secondary (43.2%, 472) or the tertiary level (45.5%, 497), with only 11.3% (n=124) at the primary level.
The researchers examined the suitability and appropriate of using a Distress Tolerance Scale (DTS) in Jamaica and this was done by way of exploratory factor analysis before the index was constructed for usage. Cronbach alpha for the DTS 0.883, which means that the DTS is suitable for exploratory factor analysis. Using exploratory factor analysis, the 15-item DTS was found to be suitable and appropriate for assessing Distress Tolerance for the Jamaican population―KMO = 0.912, P < 0>
The findings revealed that on average distress tolerance among Jamaicans was a moderate one (42.8±10.3, 95%CI: 42.2-43.4, out of 75.0), and this is recorded during the COVID-19 pandemic. The continuous variable was converted into an ordinal variable for the purpose of this analysis, which is depicted in Figure 1.
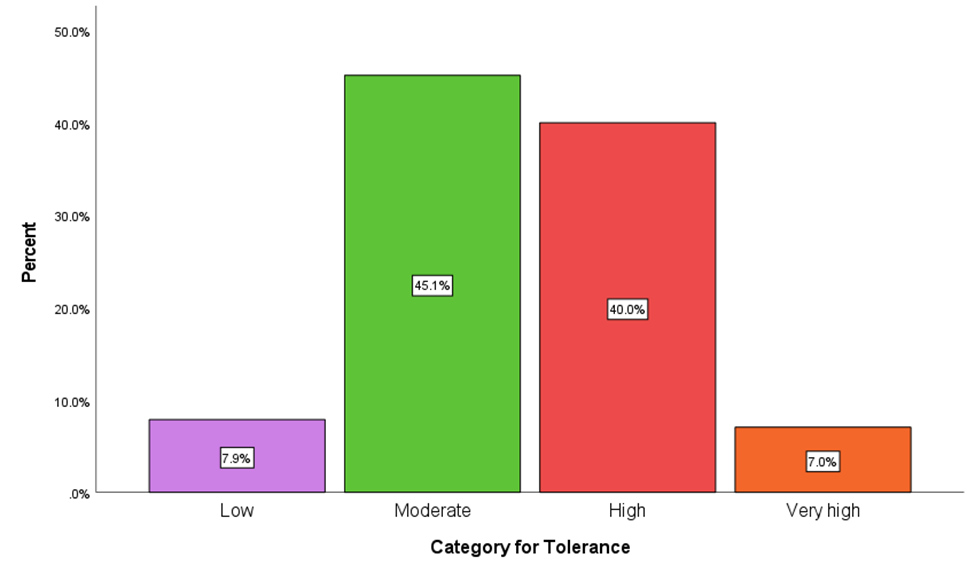
Figure 1 The tolerance of Jamaicans during COVID-19 at the time of the data collection. The findings show that 7.9% of the sampled population have a low tolerance level, 45.1% have a moderate tolerance level, 40% have a high tolerance level and, 7% have a very high tolerance level. This finding revealed that Jamaicans are moderately tolerant of the COVID-19 pandemic.
Table 2 shows the cross-tabulation of tolerance based on gender. Overall, across the board, 660 women and 433 men were used to examine whether there is a statistical association between the genders for this study. The cross-tabulation revealed no statistical relationship between tolerance level and gender of the sampled respondents (ꭓ2 (3) = 2.212, P = 0.530)―among women, 41.1% had high tolerance level compared to 38.3% of men.
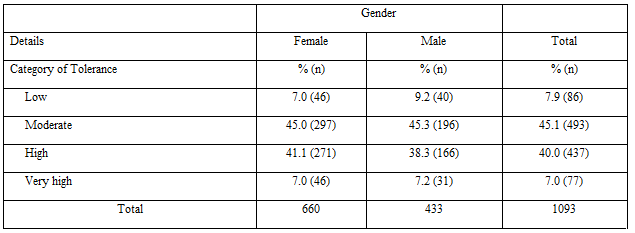
Table 3 presents the cross-tabulation of the tolerance level of the sampled respondents by age. The results indicate that participants between 38-47 years old had a low tolerance level of 5.7% (n=11), while those 58 years and older had a low tolerance of 6.0% (n=5), and 9.4% (n=29) for those 28-37 years. Furthermore, the Chi-square test revealed that there is no statistical relationship between tolerance level and the age of the sampled respondents (ꭓ2 (12) = 12.395, P = 0.415).
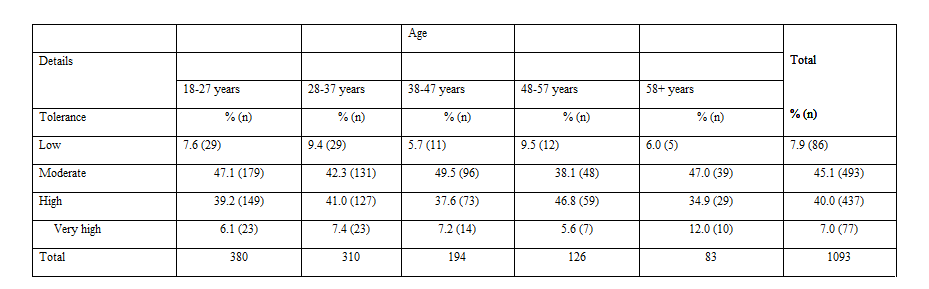
Table 4 presents the cross-tabulation of the tolerance level of the sampled respondents by the parish. The findings show that there is a statistical relationship between tolerance level and the parish of residence among the sampled respondents (ꭓ2 (36) =70.083 ˃ P ˂ 0.001). Of the sampled respondents, people who reside in Portland had the least level of tolerance (0%), while those who dwelled in St. Ann had the highest level of tolerance (17.0%, n=8).
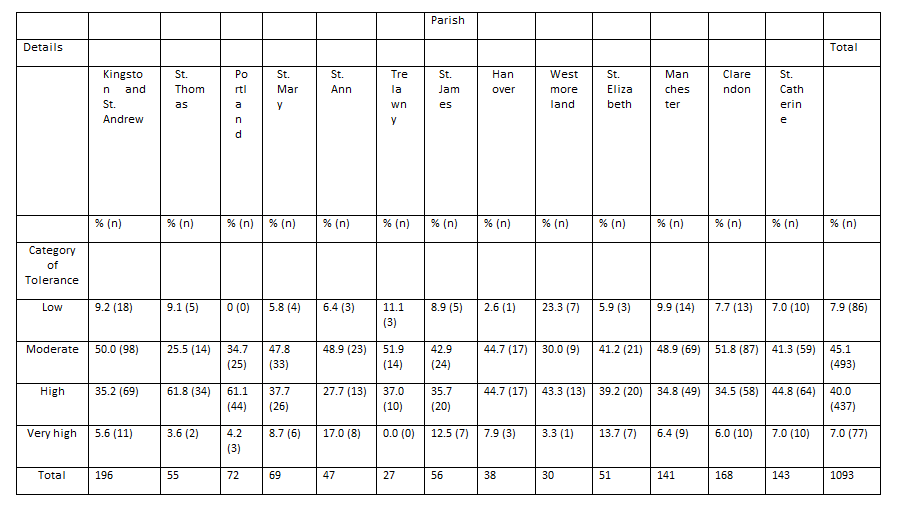
Table 5 shows the cross-tabulation of tolerance level of the sampled respondents by educational level. Chi-square test indicates that there no statistical relationship between tolerance level and the educational level of the sampled respondents (ꭓ2 (6)=9.801, P = 0.133).
Table 6 depicts the cross-tabulation of tolerance level of the sampled respondents who currently have or do not have COVID-19. The findings indicate a statistical relationship between tolerance level and those currently diagnosed with COVID-19 (ꭓ2 (3)=13.080, P = 0.004). Of the total respondents (n=1093), 78 (7.1%) indicated that they are currently infected by COVID-19, while 1015 (92.9%) denied experiencing COVID-19. Furthermore, those with the most COVID infections were at the “Moderate” tolerance category level (50%, n=39), while those with the lowest rate of infections or no infection was at the “Very high” tolerance category level (7%, n=71).
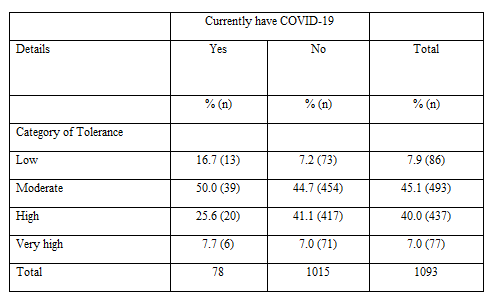
Table 7 shows the cross-tabulation of tolerance levels of the sampled respondents who have or have not contracted the COVID. Chi-square test showed that there is a statistical association between the two aforementioned variables [ꭓ2 (3) = 14.313, P = 0.003]. Among those who denied ever having COVID-19, most were at the “Moderate” tolerance category level (46.7%, n=398) compared to 46.7% (398) who indicated having not contracted COVID-19. Furthermore, the cross tabulations revealed that 39.0% (94) those who have contracted COVID-19 had a high tolerance level compared to 40.3% (343) of those who have not contracted the virus.
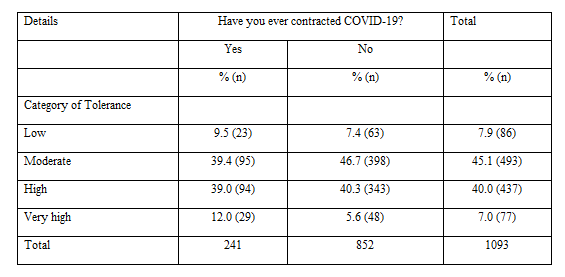
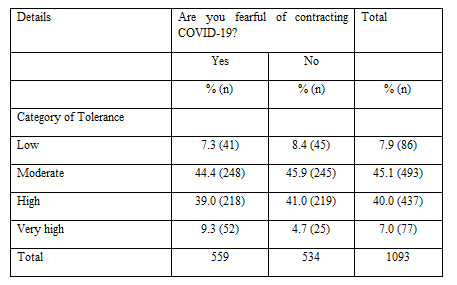
Table 8 shows the cross-tabulation of tolerance level of the samples respondents who are fearful of contracting COVID-19. Chi-square test revealed that the is statistically significant relationship between the two previously mentioned variables (ꭓ2 (3) = 9.107, P = 0.028. Of those who are fearful of contracting COVID-19, 39.0% (218) have a high level of tolerance compared to 41.0% (219) who are not fearful of contracting the virus.
The novel Coronavirus (SARS-COV-2), which emerged in Wuhan, China, in December 2019 and subsequently became a pandemic, is a member of the family of viruses that can lead to diseases ranging from mild colds to severe Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS). Considering humanity’s struggle against epidemics from the past to the present, it is well-known that epidemics have psychological, economic, and social effects on individuals (Korkmaz & Güloğlu, 2021). Besides the fear of being infected with COVID-19 and the consequences for oneself or loved ones, the strict measures taken to prevent the spreading of the pandemic might increase the probability of developing mental health problems. This study aimed to assess Jamaican’s tolerance and how it affects their fear of contracting COVID-19. Therefore, the following research questions were formulated, which helped to develop a questionnaire for data collection. The research questions were: What degree of tolerance among Jamaicans during the COVID-19 pandemic? How fearful are Jamaicans in contracting COVID-19? Does tolerance affect the fear of Jamaicans contracting COVID-19? The targeted population was 1067 Jamaican’s 18 years and older. However, the final sample for the research was n= 1093 respondents.
The findings from the research indicated that more females, 60.4% (n=660), took part in the questionnaire than males, 39.6% (n=433). Most of the respondents were aged 18-27 years, 34.8% (n=380). The majority was from Kingston and St. Andrew, 17.9% (n=196). Concerning tolerance and gender, all 45.1% (n=493) of the sampled respondents had a moderate tolerance level. Females accounted for n=297 of the sampled respondents, which were higher than males that accounted for n=196 of the sampled respondents.7% (n=46) of females had a low level of tolerance while 9.2% (n=40) of males had a low tolerance level, 41.1% (n=271) of females had a high tolerance level compared to males where 38.3% (n=166) of them had a high tolerance level. The data also showed that 7.0% (n=46) had a very high tolerance level, while 7.2% (n=31) of males had a very high tolerance level. In support of these results, a study was conducted by (Rokosz & Poprawa, 2021); the study aimed to evaluate the psychometric properties of a Polish adaptation of the Distress Tolerance Scale (DTS). One thousand two hundred ten individuals aged between 18 and 69 participated in the study (45% men, 51% women). The results from this study showed that men have a higher level of distress tolerance than females, compared to results of this research which shows that females have a higher distress tolerance level than males.
According to Janmaat and Keating (2017), the new millennials are likely to be more tolerant than older age groups and earlier generations of young people. Concerning age, it was revealed that most of the respondents, 45.1% (n=493), have a moderate tolerance level. There were more responses of moderate tolerance from persons with ages ranging between 18-27 years, 47.1% (n=179). A significant amount of the sampled respondents also has a high level of tolerance, as evidenced by 40% (n=437), representing a total of 1093 respondents. 7.9% (n=86) of the respondents represent those with a low tolerance level, and 7.0% (n=77) have a very high tolerance level. Regarding parish, most moderately tolerant respondents reside in Kingston and St. Andrew with 50% (n=98) and the least tolerant from Westmoreland 30% (n=9). Kingston and St. Andrew have the highest number of respondents with a low tolerance level with 9.2% (n=18), and Trelawny has the least amount.
Of the sampled respondents, 45.1% (493) of them had a moderate tolerance level concerning tolerance and education. In comparison, 40% (437) had a high level of tolerance., 47.1% (234) of those who have a moderate level of tolerance has a tertiary education, and 38.8% (183) of those with secondary education had a high level of tolerance. Janmaat and Keating (2017) found that the percentage of 25- to 65-year-olds completing tertiary-level education increased. This process, which led to new generations being even better educated than previous ones, is likely to have produced growth in tolerance because of the strong association between educational attainment and tolerance at the individual level, which is one of the most consistent findings in social science research. Several reasons have been proposed why more educated people are more tolerant. Some of these reasons are that education enhances the knowledge and reasoning skills of people, education cultivates tolerance directly through socialisation: the longer individuals stay in the education system, the more they are exposed to tolerance as the core value that it promotes and thus the more likely they are to internalise it, education enhances the competitive position of individuals and diminishes feelings of economic insecurity.
The sampled respondents were asked whether they have currently had COVID-19 or not; 78 of the sampled respondents stated that they currently have COVID-19, while the remaining 1015 denied having COVID-19. Based on the results obtained from doing a crosstabulation, 44.7% (n=454) of those who denied having COVID-19 had a moderate tolerance level. 50% (39) of those with COVID-19 also have a moderate tolerance level. Only 7.0% (n=71) of those who denied having COVID-19 have a very high level of tolerance, while 7.7% (n=6) of those who have COVID-19 have a very high level of tolerance. 16.7% (n=13) of the respondents who have COVID-19 have a low tolerance level, while 7.2% (n=73) of the respondents who do not have COVID-19 have a low tolerance level.
One question from the survey asked the respondents if they had ever contracted COVID-19; of the 1093 respondents, 241 stated that they had contracted COVID-19, while 852 said they had not contracted COVID-19. 46.7% (n=398) who denied contracting COVID-19 have a moderate level of tolerance, 7.4% (n=63) have a low level of tolerance and 40.3% (n=343) have a high level of tolerance. Those who stated that they have contracted COVID-19 also have a moderate level of tolerance with a percentage of 39.4% (n=95), 9.5% (n=23) have a low level of tolerance and 39% (n=94) have a high level of tolerance.
Fear is an adaptive response in the presence of danger. However, when threat is uncertain and continuous, as in the current coronavirus disease (COVID-19) pandemic, fear can become chronic and burdensome. A study was conducted to identify predictors of fear of the coronavirus, three days after the World Health Organization declared the coronavirus outbreak a pandemic between March 14 and 17, 2020. The results from this survey replicate findings from earlier studies. Particularly, it was found that, as in the 2009–2010 Swine flu pandemic and the 2015–2016 Zika virus outbreak (Blakey & Abramowitz, 2017; Wheaton et al., 2012), health anxiety was related to increased fear of the current coronavirus pandemic. Furthermore, the findings replicate earlier reports that more media exposure is related to fear (Mertens et al., 2020). From the findings of this survey majority of the sampled respondents are fearful of contracting COVID-19; this is represented by n=559 of the total respondents, while those who are not fearful are represented by n=534 of the total respondents. Those who are fearful have a moderate tolerance level represented by a percentage of 44.4% (n=248), those who have a low tolerance is represented by a percentage of 7.3% (n=43), the persons who have a high tolerance level is represented by a percentage of 39% (n=318) and 9.7% (n=52) have a very high tolerance level. The respondents who are not fearful of contracted COVID-19 also have a moderate level of tolerance, 45.9% (n=245), 8.4% (n=45), 41% (n=219) are highly tolerable and 4.7% (n=25) have a very high tolerance level.
From the study conducted, we can conclude that tolerance does affect the fear of Jamaicans contracting COVID-19. Based on the survey, few persons highly tolerant of effects of the COVID-19 pandemic but rather moderately tolerating it. Most of these persons are between ages 18-27. According to Janmaat and Keating (2017), the new millennials are likely to be more tolerant than both older age groups and earlier generations of young people. The researchers believe that this is so because younger adults can find new ways to make living comfortable and it is easier now than before since we are living in a technological era. Additionally, these persons reside in the parish of Kingston and St. Andrew. This is the main cities of the country and so resources such as internet is easily accessible and more prevalent, which may help to explain why tolerance level is higher in these parishes. 241respondents stated that they have contracted COVID-19 while 852 stated that they have not contracted COVID-19. This may be due to the fact that are taking precautionary measures hence there are not a lot of persons contracting COVID-19. The findings suggest that the majority of the sampled respondents are fearful of contracting COVID-19 (n=559) of the total respondents compared to those who are not fearful (n=534) furthering indicating that tolerance does affect fear.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
