
Research article | DOI: https://doi.org/10.31579/2694-0248/022
* Vreden National Medical Research Center of Traumatology and Orthopedics.
*Corresponding Author: Tsybin Aleksandr Vladimirovich, Vreden National Medical Research Center of Traumatology and Orthopedics.
Citation: Tsybin Aleksandr Vladimirovich, V.V. Lubchak (2021). ASPID classification of post-Traumatic Acetabular Deformities in Primary total hip Arthroplasty. J. Clinical Orthopedics and Trauma Care, 3(2); DOI:10.31579/2694-0248/022
Copyright: © 2021 Tsybin Aleksandr Vladimirovich, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 December 2021 | Accepted: 20 December 2021 | Published: 27 December 2021
Keywords: acetabulum; posttraumatic deformity; total hip arthroplasty; aspid
Total hip arthroplasty (THA) is a successful surgical procedure that allows to quickly relieve pain, restore joint function and improve the quality of life of patients. The results of arthroplasty in patients with consequences of acetabular fractures are worse in comparison with other causes.
Material and Methods. We evaluated 117 computed tomograms with post-traumatic changes in the acetabulum. 241 displacements of the walls of the acetabulum were revealed and analyzed. All cases were separated according to three criteria: localization, degree of displacement and present or absence of pelvic discontinuity. It was revealed that the number of cases with a displacement of the walls by 5-6 mm significantly fewer than cases with an offset from 0 to 4 and more than 6 mm, thus, these groups are isolated from each other. It can also be seen that the number of cases with a wall displacement of more than 15 mm is significantly greater than other cases, which also allows isolate this group.
Results. Based on the data obtained, an original ASPID classification of post-traumatic acetabular deformities was proposed, based on the localization of the deformity, the degree of displacement and the state of the pelvis. Based on the analysis of the literature and our own experience, an algorithm for choosing surgical options for implantation of the acetabular component, depending on the deformity, is proposed. The alphanumeric code used in the classification is universal, allows you to personalize each specific case and easily analyze the databases to assess the results of arthroplasty.
Total hip arthroplasty (THA) is a successful surgical procedure that allows to quickly relieve pain, restore joint function and improve the quality of life of patients. Hip arthroplasty has a history of more than fifty years and therefore the indications, contraindications and long-term results are widely described in the publications and registries of arthroplasty.
According to the literature, the results of arthroplasty in patients with consequences of acetabular fractures are worse in comparison with other causes. Stibolt et al (2018) note a relatively high rate of complications after primary arthroplasty in patients with consequences of acetabular fractures [1]. In a review publication, Hamlin et al. (2017) point out the lack of data on the results of primary arthroplasty in patients after acetabular fractures. The authors of the article suggest that the lack of comprehensive data on the results of primary arthroplasty in patients after trauma to the acetabulum may be associated with a relatively small number of cases with this pathology (about 10%), but requires study in order to improve the results [2]. Stibolt (2018), made a systematic review of 1830 publications and notes a 10-year survival rate of an endoprosthesis in patients of this group of 83.74%, which is also lower in comparison with the results of primary arthroplasty for other causes [1].
In Russia, there were some attempts to develop a systematic approach to total arthroplasty for post-traumatic deformities of the acetabulum, but did not find widespread use [3; 4].
Analysis of literature on primary hip arthroplasty indicates the absence of a generally accepted system assessment of post-traumatic acetabular deformities, which in turn makes it extremely difficult both to analyze the results of primary arthroplasty in this group of patients, and to develop a systematic approach to choosing surgical strategy.
According to the endoprosthetics register of Russian Vreden register of arthroplasty, in the period from 2013 to 2018, 1157 primary hip arthroplasties were performed for post-traumatic coxarthrosis (after hip and acetabular fractures). When analyzing medical records, it was found that post-traumatic deformities of the walls of the acetabulum were present in 313 cases (27%). Of which computer preoperative tomograms of the pelvis were performed in 117 patients. Thus, based on the inclusion criteria for further analysis, we used 117 cases of primary THA with post-traumatic deformities of the walls of the acetabulum. In this sample, the number of men significantly exceeds the number of women (80 men, 37 women), the age of patient’s ranges from 43 to 76 years, the average age was 59 ± 7 years. Of these, 9 cases (8%) were in combination with pelvic discontinuity.
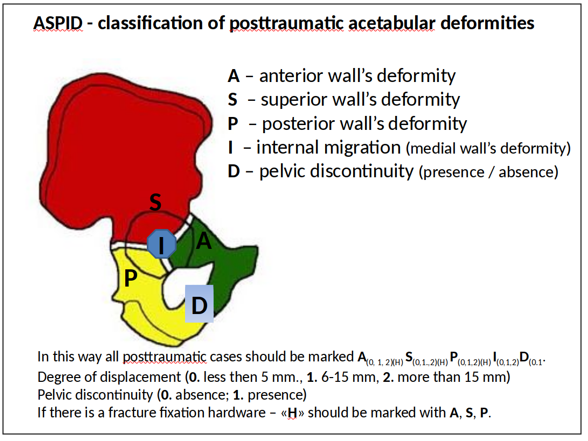
When measuring the degree of displacement during post-processing of axial slices obtained after CT, multiplanar reconstructions of images were performed in three perpendicular planes with additional control of the initial position of the pelvis using 3D reconstructions. The displacement of the fragments (walls) was measured between two parallel planes (lines) passing tangentially to the most distant points of the deformation contour resulting from the displacement of the fragments. To describe the localization of deformities, we used the main surgical landmarks of the acetabulum: the anterior (A), superior (S), posterior (P) and internal (I) walls, which in the Latin alphabet, based on the first letters of the landmarks names, made it possible to form the abbreviation ASPID (anterior, superior, posterior, internal walls, D - pelvic discontinuity)[5].
When analyzing computed tomograms, it was determined that in total in 117 cases we were considering, 241 displacements of the walls of the acetabulum were revealed (Table 1).

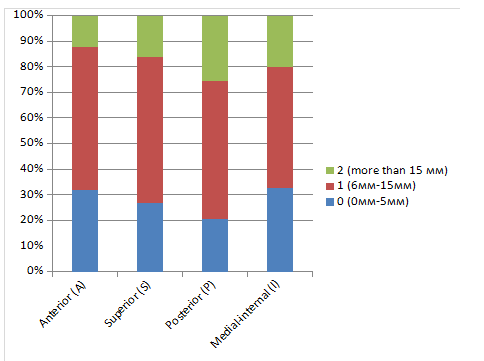
Then we analyzed the distribution of values (mm) separately for each wall of the acetabulum. The average displacement values have also been determined (fig. 1).
In 12 cases (1%) out of 117, a simultaneous displacement of all four walls of the acetabulum was revealed. The average displacement of the walls in these cases is presented in Table 3.

Based on the table compiled during the description and analysis of tomograms of patients with post-traumatic acetabular deformities, the distribution of values displacement values in mm was analyzed separately for each wall. As a result of the analysis, it was revealed that the number of cases with a displacement of the walls by 5-6 mm significantly fewer than cases with an offset from 0 to 4 and more than 6 mm, thus, these groups are isolated from each other. It can also be seen that the number of cases with a wall displacement of more than 15 mm is significantly greater than other cases, which also allows isolate this group. Based on the analysis of the data obtained, we have developed three degrees of displacement for each wall of the acetabulum: 0 degree - 0-5 mm, 1 degree - 6–15 mm, grade 2 - more than 15 mm. Based on the data obtained, we proposed an original ASPID classification of post-traumatic acetabular deformities (Figure 2).
The analysis of publications on hip arthroplasty in patients with consequences of acetabular fractures [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25] was carried out. Based on the analysis of publications and our own experience in THA, we proposed an algorithm for choosing surgical options depending on the deformation of the acetabulum [26, 27].
According to the proposed algorithm, the necessary options for implantation of the acetabular component are selected based on the table, taking into account the alphanumeric code in each specific case.
In our opinion, the presented assessment system and the display of acetabular deformity by an alphanumeric code makes it possible to accurately describe the indicated changes in the support structures, to note the presence of hardware and the state of pelvis (pelvic discontinuity).
In our opinion, this gives a fairly complete picture of the acetabulum for preoperative planning. On the one hand, the proposed classification allows you to personalize data for the most accurate planning the operation, on the other hand, the presence of an alphanumeric formula allows you to collect and structure data for statistical processing, which, in turn, may be a key factor for the further development of an algorithm for choosing surgical tactics. Currently, the proposed classification is used to form the base data and analysis of the results of primary arthroplasty in patients with post-traumatic acetabular deformities. The use of an alphanumeric code greatly facilitates the formation of a sufficiently detailed database indicating the state of each wall of the acetabulum, the presence of hardware and the state of the pelvic ring of the operation, which in the future will make it possible to analyze in detail a set of factors that may be the reasons for aseptic loosening of the acetabular component of the endoprosthesis. The basic principles of the algorithm for the selection of surgical strategy according to the localization and degree of displacement of the acetabular walls, in our opinion, the congruence of the standard hemispherical acetabular cup. In addition, such an algorithm is based on the general principles of THA and should take into account the use of additional options, starting with autologous bone grafting, additional fixation of the component with screws, the use of trabecular metal augments and custome made implants, which in some cases are extremely necessary. In the future, a multicenter study is planned to assess the effectiveness of the ASPID classification, correction of the algorithm and, provided the study is successfully completed, the proposed assessment system can be introduced into the practice of orthopedic surgeons.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
