
Research Article | DOI: https://doi.org/10.31579/2694-0248/053
Department of Orthopaedic Surgery. Full professor. University Children's Hospital of Camagüey. Camagüey city. Cuba.
*Corresponding Author: Alejandro Alvarez López, Department of Orthopaedic Surgery. University Children's Hospital of Camagüey. Camagüey city. Dolores Betancourt No 2. Camagüey city. Camagüey. Cuba.
Citation: Alejandro A. López, (2023), Arthrodiastasis in Knee Osteoarthritis, J. Clinical Orthopedics and Trauma Care, 5(1); DOI:10.31579/2694-0248/053
Copyright: © 2023, Alejandro Alvarez López. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 January 2023 | Accepted: 26 January 2023 | Published: 13 February 2023
Keywords: knee osteoarthritis; knee joint distraction; arthrodiastasis; external fixation; surgical treatment
Background: Knee osteoarthritis is a common disease and affects a large group of patients, especially those over 40 years of age. Treatment can be conservative or surgical; the latter one includes those that preserve the joint, such as arthrodiastasis.
Aim: to provide updated and detailed information on arthrodiastasis for patients suffering from knee osteoarthritis.
Methods: PubMed, Hinari, SciELO and Medline databases were searched for citations from October 1st 2022 to November 30th 2022 using the EndNote search manager and reference manager. Out of 162 articles, 30 selected citations were used in this review, being 23 of the last five years.
Results: the effects of arthrodiastasis in patients with osteoarthritis of the knee are mentioned. The procedures that can be combined with this surgical modality, both arthroscopically and with biological rescue therapies are described. Reference is made to the indications for arthrodiastasis and the main differences with osteotomy and arthroplasty. The results of arthrodiastasis by various authors in patients with osteoarthritis of the knee are shown.
Conclusions: arthrodiastasis is a surgical method that preserves the knee joint, its indications are very specific and it is not a frequently used modality. To achieve distraction of the joint, an external fixation device is needed, which is applied for an average time of six weeks. Complications are minimal and are mostly related to the use of the distraction device.
Osteoarthritis is the most frequent chronic degenerative disease, affecting 10% of the population after the age of 60, according to Goh et al. [1].
Treatment aims to relieve pain and improve joint function, for this purpose conservative and surgical techniques are used, the latter justified by the failure of the first one [2,3].
Surgical techniques are subdivided into those that preserve the joint such as: arthroscopy, osteotomy, proximal fibula ostectomy, which can be carried out both in isolation and in combination with other surgical procedures [4,5].
On the other hand, surgeries that do not preserve the joint include arthroplasty and arthrodesis; the arthroplasty can be partial or total [6].
Arthrodiastasis (joint distraction) of the knee is an alternative surgical method that preserves the patient's joint, which was initially introduced to correct joint malalignment and treat contractures; it is used in diseases of the knee, hip such as Perthes disease, in addition to ankle and knee osteoarthritis [7,8].
The main purpose of arthrodiastasis in patients with primary knee osteoarthritis lies in slowing down the degenerative process of the joint and avoiding more complex procedures like arthroplasty. For its realization, external fixators are used, which are used for a period of approximately six to eight weeks. [9,10]
Because of the increasing number of patients suffering from knee osteoarthritis in the population, the search for less expensive and effective treatment alternatives, the authors of this paper aims to provide updated and detailed information on arthrodiastasis for patients suffering from knee osteoarthritis.
An extensive literature search in various data bases such as: PubMed [https://pubmed.ncbi.nlm.nih.gov/], Hinari [https://www.who.int/hinari/es/], SciELo [https://scielo.org/es/] and Medline [https://medlineplus.gov] was carried out with search term including ' knee distraction AND knee osteoarthritis', 'arthrodiastasis AND knee osteoarthritis', 'knee joint distraction' from October 1st 2022 to November 30th 2022. Out of 162 articles, 30 selected citations were used in this review, being 23 of the last five years.
A review of biomechanical studies, originals, and case presentations in patients who underwent arthrodiastasis because of knee osteoarthritis were considered. Studies on animals and patients with knee fractures were excluded.
Mechanism of action and devices
The repair of cartilage damaged by degenerative arthropathy is based on three aspects when applying arthrodiastasis, the first that due to distraction, compression and shear forces on the cartilage are avoided and therefore reduce further tissue injury; second, the nutrition of the cartilage is maintained both with or without weight bearing of the extremity and third, during arthrodiastasis a transient periarticular osteopenia is triggered, which modifies the sclerosis present in the subchondral bone and therefore decreases the mechanical impact of the cartilage. In addition to what was stated previously, while distraction is applied, a large number of repair cells are released, which improves the biochemical and mechanical environment of the joint [11,12].
Arthrodiastasis is performed using an external fixation device consisting of two dynamic bars, one medial and the other lateral, joined by eight wires, half in the femur and the other in the tibia. At surgery, a distraction of two millimeters is performed, and then one millimeter per day until reaching five, an element that is verified by means of serial X-rays of the joint. After obtaining the desired distraction, medical discharge was given under prophylactic anti-thrombotic measures and the support of the extremity was allowed with the help of crutches. Serial cures of the wires are performed to avoid infection. At six weeks the external fixation is usually removed [13,14].
This joint distraction procedure can be combined with others such as those performed arthroscopically and include: debridement, microfractures, and nanofractures [15,16].
At the distraction time, therapies such as biological rescue through the administration of platelet-rich plasma and others like the administration of intra-articular hyaluronic acid can be applied [17,18].
Indications
The indications for arthrodiastasis are various, but most authors agree on its performance in young patients under 60 years of age, in whom it is convenient to apply surgical techniques that preserve the joint, other elements to take into account are the patients weight, since most authors recommend its use in patients with a body mass index below 35 kg/m2, in addition to joint mobility, which must be normal or at least 120 degrees of flexion. Indications according to the opinion of some researchers are shown in Table 1.
| Author/Year | Indications |
| Jansen, et al. [19] (2021) | Age less than 65 years, radiographic status according to Kellgram and Lawrence of two or more, intact ligaments, normal range of motion (at least 120 degrees of flexion) and body mass index less than 35 kg/m2. |
| Besselink, et al. [20] (2020) | Patients under 65 years of age with varus deformity, normal range of motion (flexion greater than 120 degrees), stable knees and body mass index less than 35 Kg/m2. |
| Van der Woude, et al. [21] (2017) | Failure of conservative treatment, visual analog pain scale ≥ 60 mm and age less than 60 years. |
| Intema, et al. [22] (2011) | Age less than 60 years, visual analogue pain scale ≥ 60 mm, and radiographic signs of tibiofemoral osteoarthritis. |
Table 1: Surgical indications for arthrodiastasis in patients with primary knee osteoarthritis according to some researchers.
Differences between arthrodiastasis, osteotomy and arthroplasty
There are differences between the surgical techniques of arthrodiastasis, osteotomy and arthroplasty when taking into account several factors such as: joint mobility, cost, degree of disease and conservation of the joint (Table 2) [23-25].
| Factors | Arthrodiastasis | Osteotomy | Arthroplasty |
| Joint mobility after the procedure | Delayed six to eight weeks. | From one to two weeks. | Immediate
|
| Cost | Low | High | Very high |
| Grade of knee osteoarthritis according to radiographic classification. | Intermediate degrees
| Intermediate degrees
| The most advanced of the disease.
|
| Joint preservation. | Yes | Yes | No |
Table 2: Main differences between arthrodiastasis, osteotomy and knee arthroplasty.
Results of arthrodiastasis in patients with knee osteoarthritis
The studies consulted for the preparation of this article show the results in patients with knee osteoarthritis treated by arthrodiastasis in a follow-up period of 12 to 60 months, with a number of patients ranging from 15 to 62 (Table 3).
| Authors/Years | Number of patients | Follow-up | Results |
| Jansen, et al. [19] (2021) | 20 | 2 years | Clinical results are not inferior to arthroplasty and high tibial osteotomy. |
| Besselink, et al. [20] (2020) | 20 | 2 years | The clinical benefits and the increase in cartilage thickness are maintained two years after treatment. |
| Hoorntje, et al. [26] (2020) | 16 | 5 years | No differences were found between the results compared with osteotomy, it is a viable option for young patients. |
| Takahashi, et al. [27] (2019) | 62 | 1 year | Similar results at 12 months after osteotomy and total arthroplasty. |
| Van der Woude, et al. [28] (2017) | 20 | 5 years | Prolonged clinical benefits. Useful in young patients with severe knee osteoarthritis. |
| Dong et al. [29] (2017) | 15 | 18 months | The combination of distraction with arthroscopic debridement is effective in relieving pain and improving joint function. |
| Intema, et al. [22] (2011) | 20 | 1 year | Good clinical benefits are obtained. |
Table 3: Results of arthrodiastasis of the knee in gonarthrosis.
In relation to the type of external fixation to be used, it could be monopolar, bipolar (Figure 1) or circular, there are no biomechanical differences according to a study carried out by Chowdhury et al. [30].
Figure 1. Bipolar external fixation used for knee distraction in a patient with gonarthrosis.
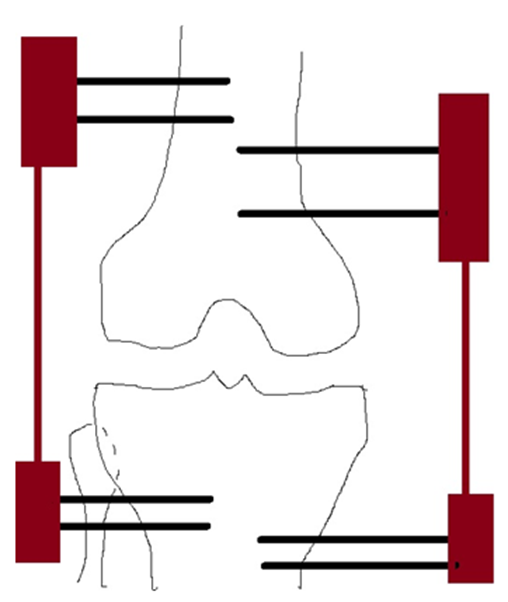
Figure 1: Graphic representation of a bipolar external fixator to perform arthrodiastasis of the knee.
The most common complications in patients treated by arthrodiastasis are: pin infection used in the distraction, possibility of osteomyelitis even after three weeks after removing the device, failure of the desired distraction, bone fractures in the area of the pins, and joint stiffness requiring manipulation under anesthesia [29,30].
Arthrodiastasis is a surgical method that preserves the knee joint, its indications are very specific and it is not a frequently used modality. To achieve distraction of the joint, an external fixation device is needed, which is applied for an average time of six weeks. Complications are minimal and are mostly related to the use of the distraction device.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
