
case report | DOI: https://doi.org/10.31579/2692-9392/126
1 Pneumo-allergology of Pediatrics
2 Department, Mother and Child Hospital A. Harouchi UHC Ibn Rochd, Hassan II University, Casablanca Faculty of Medicine and Pharmacy
*Corresponding Author: Alaoui-Inboui Lalla Fatima Zahra, Pneumo-allergology of Pediatrics.
Citation: FZ. Alaoui-Inboui, A. Jouida, S. Salimi and B. Slaoui, (2022) Arteria Lusoria: An Anatomical Curiosity And A Clinical Entity: About Three Case Reports. J. Archives of Medical Case Reports and Case Study, 5(5); DOI:10.31579/2692-9392/126
Copyright: © 2022 Alaoui-Inboui Lalla Fatima Zahra, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 May 2022 | Accepted: 31 May 2022 | Published: 06 June 2022
Keywords: pulmonary vascular malformation; arteria lusoria; infants
Pulmonary vascular malformations are a set of abnormalities, some of which are quite common, as arteria lusoria. It is a congenital malformation in which the right subclavian artery does not come from the right brachiocephalic trunk, but originates directly from the left aortic arch, downstream from the other large arterial trunks.
Pulmonary vascular malformations are a set of abnormalities, some of which are quite common, as arteria lusoria. It is a congenital malformation in which the right subclavian artery does not come from the right brachiocephalic trunk, but originates directly from the left aortic arch, downstream from the other large arterial trunks. Its prevalence is 0.5-2.5%. Many arteria lusoria cases are unnoticed. It can be discovered during signs of respiratory tract compression and/or the esophagus such as dyspnea or dysphagia or even repeated respiratory infections. It was therefore interesting to recall, on the light of these case reports, the embryological origin as well as the clinical and radiological characteristics of this congenital defect. Its management remains medical with simple monitoring, if it is asymptomatic. Surgery would be necessary once symptomatic or when it is associated with a Kommerell diverticule
Clinical Case n°1:
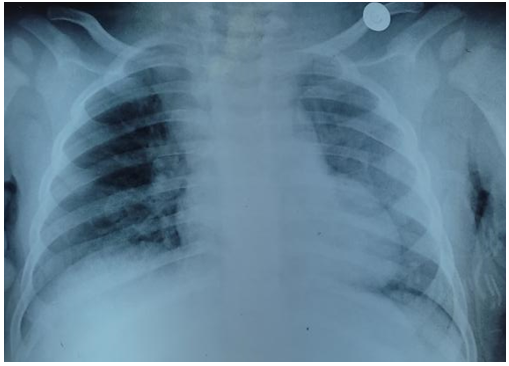
It is a 10-month-old female infant. She came up for a second episode of wheezing dyspnea with a free interval. The first wheezing dyspnea episode appeared at the age of 8 months. The clinical check up underlined respiratory distress by a suprasternal pull, a subcostal pull and an intercostal pull. The pulmonary examination found out bilateral and diffuse rasps. further clinical examination was without particularities. front chest x-ray showed out bronchial syndrome with a right apical pulmonary focus (Figure 1). The patient was first treated for acute viral bronchiolitis. but while the respiratory symptomatology persisted beyond the 10th day, a thoracic angioscan was performed. It confirmed the right subclavian artery passage into the retroesophageal associated with infectious pulmonary disease (Figure 2). with this congenital defect, an echocardiogram was perfomed. the outcome was normal. Management consisted of infectious pulmonary disease treatment based on cephalosporin third-generation antibiotic therapy (50mg/kg/day intravenous) with respiratory great improvement.

Case report n°2 :
It is a 4 month old female infant. She suffered from recurrent wheezing from birth without free interval, associated with bronchial obstruction. The clinical examination noted respiratory distress by nose wings beating, suprasternal indrawing, chest indrawing, intercostal indrawing and seesaw breathing. A polypnea at 88 c/min. Pulmonary examination revealed bilateral and diffuse whistling rales. Further clinical examination was normal. A front chest X-ray revealed bronchial syndrome with bilateral alveolar foci (Figure 3). The thoracic CT angiography confirmed the right subclavian artery passage into the retro-oesophageal with ground glass areas and scattered foci of condensation related to an infectious pneumopathy (Figure 4). An infection checkup was performed. It was with no anomaly. Echocardiography was normal. It was also normal. treatement management consisted of pneumonia treatment with intravenous antibiotic therapy based on 3rd generation cephalosporin (50mg/kg/d). The outcome was favorable, with respiratory symptoms improvement. The patient is followed in consultation.


Case report n°3:
It is a 13 month old male infant. He was admitted for recurrent wheezing management without a free interval. The wheezing had appeared early from the first month of life, complicated by solids dysphagia. Clinical examination noted respiratory distress, mainly intercostal indrawing and seesaw breathing. A chest X-ray revealed 2 right and middle upper lobe alveolar foci. The echocardiogram was normal. A chest CT angiography confirmed right subclavian artery origin on the posterior part of the arch of the aorta with contiguous origin of the 2 primitive carotid arteries. Treatment consisted of surgery. The outcome was favorable with progressive symptomatology improvement.
Arteria lusoria or the right retroesophageal subclavian artery is the most common aortic arch malformation. It takes its origin directly from the aorta and thus joins the right upper limb by taking an aberrant tract. Its prevalence is 0.5-2.5% [1]. The arches insert directly onto the arch in the following order: the right common carotid artery, the left common carotid artery, the left subclavian artery, and, finally, the right subclavian artery. This particular disposition is the result of embryonic development anomaly [2].
The right subclavian artery results from a sequential interruption of the fourth right aortic arch remodelling, from the distal part of the dorsal aorta to the fourth arch, and finally from the sixth cervical intersegmental artery [3]. The right dorsal aorta involves distally to the sixth cervical intersegmental artery by vasoconstriction, and due to the aorta caudal growth, fixed by its thoracic parietal branches, it will remove allowing to release the Right subartery of it 's connection to the thoracic aorta. There is an abnormal degeneration of the fourth right aortic arch, and an absence of involution of the distal part of the right dorsal aorta. The aberrant right subclavian artery will therefore no longer be connected to the proximal part of the arch (ascending aorta) but will be tied to the descending aorta by the right dorsal aorta sequel [4]. It then becomes the fourth and last stick branch. (Figure 5)

This pathophysiology defect remains unknown and may include an hemodynamic factor, genetic and evolutionary origin [5]. Clinically, arteria lusoria is often asymptomatic, it is not a complete ring around the esophagus or trachea [6]. It is discovered in most of the cases incidentally during a thoracic check up for other pathologies for example cardiovascular malformations, namely a Fallot tetralogy or aorta coarctation.
In infants and young children, vascular rings show out by respiratory symptoms [7]. As for adult subjects, clinical signs may appear late. Fanette J reports, in her series of 150 cases, that arteria lusoria becomes symptomatic in adults but interrogation often finds out repeated respiratory disorders during childhood, sugesting an old and spontaneously regressive tracheal compression [8].
Arteria lusoria becomes symptomatic in 3 cases [6]:
- When the trachea and esophagus are compressed between the arteria lusoria back and the bi-carotid trunk forward
- When there is an aneurysm of this artery hence a daunting complication
- During artery's atherosclerotic degeneration, or during fibromuscular dysplasia's occurrence.
Among the most classic and well-known clinical manifestations is dysphagia as mentioned in the third case report. In this infant, the association of dysphagia with dyspnea raised fear of possible tracheal compression, which required surgical management. In children, in most of the cases, it is the aberrant right retro-esophageal subclavian artery that lead to trachea compression and can shows out in respiratory symptoms. They are due to the compression applied by the aberrant artery on the the infant's not yet rigid trachea [9]. This respiratory symptomatology can range from acute respiratory distress with polypnea, pulling, cyanosis and bronchial superinfection to single polypnea often associated with chronic cough [10] Which is consistent with the last two report cases.
Radiologically, this artery appears on a plain x-ray by a superior mediastinal fluid tone opacity, in contact with the upper right edge of the aorta arch. An esophagus opacification makes it possible to highlight an oblique impression on the top right of the esophageal wall. This esophageal transit is mainly fulfilled in infants, more rarely in adults [6]
The chest angioscan is the imaging technique of choice to assess these abnormalities more accurately and quickly for its spatial resolution. The scan shows a vessel that originates from the posterior side of the aorta and reaches the upper right limb through the posterior mediastinum, most of the time following a retroesophageal path. Magnetic raisonance imaging, if performed, easily shows this abnormality in the posterior coronal slice. It highlights a vessel that originates from the aortic isthmus, which has an oblique path up and to the right and joins the axillary region, sagittal plans show retro-esophageal localization [11]
In cases of asymptomatic arteria lusoria, management often consists of simple monitoring. However, surgical choice is suggested for dysphagia and complicated forms. Surgical treatment is based on a re-implantation of the right subclavian artery either directly onto the right common carotid artery or with a prosthetic tube at the ascending aorta [12]. The outcome is often certain after an early and adequate management as in the 3 case report.
Aortic arcs' anomaly should be looked for in case of chronic respiratory symptoms not responding to drug treatment in the infant. An early diagnosis with complete radiological investigations is necessary in order not to delay therapeutic management and to avoid severe complications. Arteria lusoria is a fairly common vascular malformation often asymptomatic and it is is of fortuitous discovery. It's diagnosis should lead to look for cardiac abnormalities and large vessels. Its course is often favorable after early and adequate management.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
