
Research Article | DOI: https://doi.org/10.31579/2692-9406/112
1ΑΤΕΙ of Epirus, School of Health & Welfare, Department of Speech Therapy, Ioannina, Greece.
2 Private Speech Therapy Center, Thessaloniki, Greece.
3Greek Company of Alzheimer Disease «Saint John», Thessaloniki, Greece.
43rd Department of Neurology, Papanikolaou Hospital Thessaloniki.
5 University of Ioannina, Medical School, Department of Nervous System & Sensors
6Medical School, Democritus University of Thrace.
*Corresponding Author: Erkotidou Sofia, Thessalonikis 37B Pulaia, Thessaloniki, Greece.
Citation: Erkotidou Sofia, Grigorios Nasios, Tafiadis Dionisios, Magda Tsolaki and Eleni Erkotidou, (2022) Application of The Diagnostic Tool Efa-4 In Dementia. Biomedical Research and Clinical Reviews, 6(5); DOI: 10.31579/2692-9406/112.
Copyright: © 2022 Erkotidou Sofia, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 February 2022 | Accepted: 18 April 2022 | Published: 28 April 2022
Keywords: εfa -4; speech and language disorders; dementia, ad
Speech is a brain function that includes virtual, mobile and sensory part for the understanding and the production of spoken and written language. The aim of this study was to present the adaptation of the diagnostic tool Examining for aphasia – 4th edition (EFA -4) in the Greek language. In dementia and especially in Alzheimer’s disease (AD), the speech and language disorders are the main diagnostic features, along with the worsening impairment of memory. The diagnostic tool EFA-4 is a standardized, reliable and valid measure of speech and language disorders. The test was administered to 50 adults separately. The sample selection, although it had uniformity in age, was regardless of origin, marital status and socioeconomic status. According to the results of the research, the EFA-4 is perceived to be particularly useful in the setting of language deficits of the patients with AD, who participated in the survey.
The specific scientific term aphasia refers to any loss, partial or total, of language ability in children and adults, as well as to any general speech impairment after a normal brain establishment. Aphasia is defined as the acquired disorder of language understanding, production and symbolic knowledge [1]. In the case of aphasia the patient cannot speak, apply the correct meaning to words, understand speech and at times cannot write or read. Every aphasic disorder is different and unique and is morphologically affected depending on the locus, the severity and the starting point of the disfunction. Aphasia comes as a result of a brain damage (AEE, head injury). However, it has been proven that speech disorders and particularly aphasia are a common phenomenon of neurodegenerative diseases.
Speech disorders – Aphasia and Alzheimer’s (AD)
Scientific research has shown a great interest in speech disorders, aphasia, dementia and more particularly AD. It has been scientifically documented that aphasia is present in all kinds of dementia and is one of the diagnostic criteria [2,3,4]. Specifically, the first Alzheimer's patient was aphasic [5]. However, only recently has aphasia been acknowledged as a major feature of AD. AD is the most common type of dementia, representing the 2/3 of all dementias. In the past years it was considered relatively rare and specific to people under 65 years of age. In the first half of the 20th century there were only 100 AD cases noted. Nowadays we are aware of the exact opposite: the disease is extremely common, especially in developed countries, while there is an exponential growth in its frequency as people get older. Age is the most important danger factor for the application of the disease. Between the ages of 65 and 85 the prevalence of the disease is constantly increasing, reaching at the age of 85 a striking 35-40%. AD is not related to the typical aging process and is characterized by a non-typical decline of brain functions; among which speech has a central role. Language deficiencies are obvious from the very early stages of the disease [7]. All AD patients show aphasic speech disorders as dementia progresses [8]. AD speeds up speech decline independently of the patient’s age, compared to the decline present in typical aging and mild cognitive impairment – MCI (. Moreover, the type of speech impairment in AD is different from that in Vascular Dementias [10,11] or Front Temporal Dementias [12]. The functional use of language, or Pragmatics, contributes to the communicative loss in dementia [13]. There is poor maintenance threads in conversation, there is short but frequent change of subject, request for more instructions, pauses in speech production with many ambiguities, incoherent speech, difficulty in maintaining eye-contact and difficulty in giving turns during a conversation [14,17]. Pragmatic deficiency may depend on the kind of interaction [18]. AD speech is described as lacking coherence [16], deranged and shortened in content [16,19,20], as well as a wide use of vague references [15,16].
Lexical – semantic deficiencies in AD are characterized by a restricted vocabulary use [21] and difficulty in naming(22), which are probably caused by an interruption in cognitive processing, perhaps during the pre-lexical stage. Lexical difficulty is one of the early deficiencies noted in people suffering from dementia [23]. Naming difficulty is the central issue of the many researches concerning speech disorders in dementia(24,25,26,27,28).The majority of researches seem to support the view that the initial interruption in word recovery is due to a cognitive and not a perceptive deficiency.
Furthermore, syntax remains unaffected in AD, except for the last stage [24,25,29,30,31]. Nevertheless, there have been reported syntactic errors such as phrase and sentence loss, as well as interruption of phrases and grammatical disagreement [32]. The perception of syntax is relatively more affected than the production [33,34]. One explanation could be that syntax is a relatively automatic cognitive function which remains unaffected during a general cognitive decline [35].
As far as phonology is concerned, phonological decline in AD patients are very rare and present only in the last stages. Even though phonological errors have been reported in some researches, they appear to be a part of a higher semantic or syntactic decline and not an individual decline in verbal sounds or morpho-phonemes (individual linguistic units that signify a change in meaning).
Schematically AD can be divided into three stages. The speech disorders of each stage can be presented as follows. In the first stage of AD, as far as pragmatics is concerned, there is difficulty in the use of naming references, difficulty in coherence, instruction, narration of stories, understanding of humour and sarcasm, there is difficulty in understanding abstract notions, difficulty in starting speech production as well as in retaining the subject of a conversation. Additionally, there is an ambiguous use of language while there need to be repeated clarifications. In semantics there is difficulty in finding the required word and frequent use of periphrasis as well as hand gestures. In syntax and phonology, during this stage, we come up with almost no error. In the second stage of mild AD, there is a poor usage of the naming reference, as far as syntax is concerned, lack of coherence and difficulty in preserving the subject of conversation. There is little use of abstract ideas and frequent repetitions. Speech is largely depended on stereotypic expressions. In Semantics, there is poor word flow with a limited vocabulary and increased use of periphrasis and failing replacements. There is frequent use of empty speech. In Syntax there are occasional grammatical errors and difficulty in understanding complex structures. In phonology there are generally no errors at all. In the third, also known as late, stage of AD there is lack of coherence, difficulty in maintaining eye contact, expression of irrelevant ideas, persistence, irrational speech and even silence. In Semantics there has been observed paraphasia, echolalia, extremely poor understanding, severely weakened naming ability, frequent ideoglossia and incomprehensible speech. In Syntax, while grammar remains generally unaffected, there is a fragmented use of incomplete sentences and phrases, as well as a poor understanding of grammatical structures. In the late stage phonological errors are more common.
It is therefore made clear that speech disorders are part of each of the three stages. Despite the universality of aphasia, in dementia the qualitative substance as well as its severity vary depending on the pathological process and its detection [6]. It is the duty of health professionals to do an initial correct diagnosis and then create a complete treatment plan. What we should keep in mind is that the more accurate the diagnosis is the more effective will the treatment be.
Diagnosis
The existence of dementia must be attested by a clinical examination – application of criteria DSM-IV, NINCDS-ADRDA – and the stage of the disease must be confirmed with the Mini-Mental State Examination (MMSE). During the paraclinic control, along with the blood and biochemic routine tests, there also needs to be a measuring of Vitamin B12 level and of the Thyroid hormones [36,37].
In our effort to improve the diagnosis and to better specify the patients’ speech difficulties we translated and adapted the diagnostic testing EFA-4 (Examining for Aphasia) into the Greek language.
Purpose
The aim of our research was to manage to give another diagnostic look for Dementias. The diagnostic approach should be characterized by reliability and validity , including new measurement methods of aphasia. Our purpose as therapists is to be able to rely on the results of our measurements in order to improve the therapeutic processes for these people. This improvement will help us improve the daily lives of patients with dementia.
What is EFA-4 diagnostic testing
EFA-4 is a regulatory, reliable and valid measuring of aphasia. It is suitable for adults whose language functions weakened after a normal establishment of language. EFA-4 offers to the clinic a method for evaluating possible aphasic linguistic deficiencies and other acquired disorders which are usually closely related to language functions. It also allows the examiner to find out about the individual’s participation in activities that might have been amended by aphasia.
EFA -4 Subtests
EFA-4 includes 10 subtests which have been created in order to evaluate the basic brain functions. Those subtests include visual recognition, acoustic recognition, tactile sensing, the acoustic comprehension of oral speech and the silent recognition with understanding. Additionally, verbal as well as non-verbal behaviour is tested, meaningful speech production and meaningful writing ability. Finally, we evaluatecommunicative and descriptive speech.
The parts of EFA-4
EFA-4 consists of the examiner’s manual, a book of images, a results record sheet – diagnostic form, an answer sheet – short test form, a brief diagnostic sheet, a form of personal medical records and an object box.
In the research conducted we used the results record sheet – the diagnostic form, the results record form and the object box.
The use of EFA-4
EFA-4 is a well structured tool with excellent psychometric properties. It has five main uses: (a) to detect the existence of aphasia, (b) to define the severity of aphasic signs and symptoms and their effect on life participation and activities, (c) to set goals for the rehabilitation of communication, (d) to record the progress made during the treatment, and (e) to inform and consult patients of aphasia, their families and the supporting social network, as well as to inform the doctors, the medical staff and Insurance Funds.
Scoring of the testing
The activities are scored with 2, 1, or 0. The main parameters of the test taker’s answers that should be taken into account during the scoring are accuracy, consistency and effectiveness. An activity should be scored with a 2 for an answer that is correct, direct and effectively produced as well as when the test taker indicates or writes correctly as required.
Scoring 1 should be given for an answer that is correct but according to the examiner is delayed or inefficiently produced (usually due to non-standard, unsteady or poorly coordinated verbal or writing movements). Scoring 1 should also be given when an answer itself is correct, but the form of the answer is not correct (i.e. a written answer to an oral question).
Scoring 0 should be given if the test taker does not respond to the activity at all, or answers incorrectly. The examiner should indicate the cases where there is no answer by writing down N/A (No Answer) next to the activity along with 0.
The scoring of answers in EFA-4 activities requires a careful observation of the behaviours and clinical judgement.
Research design
The research was divided into four parts. We began with the translation of both examinations in Greek. Then we did a pilot research to check the adaptations to the Greek language. The third part consists of the administration of the test, the coding data and the introduction of the data. The fourth part is about the analysis of the data and the interpretation of the results.
Translations and adaptation of the axamination
The translation of EFA-4 from English into Greek was done in the following procedure: the original versions of the examination were translated independently by three native speakers of Greek who were efficient in both written and spoken English. The three Greek versions were again translated into English by three different native speakers of English who were efficient in written and spoken Greek. From the three translations, the stimulus – images that were accurately translated from English into Greek and vice versa – were included in the final versions of the examination. Furthermore, the three Greek versions were given to three bilingual (English-Greek) judges, along with the English versions, in order to attest the final outcome. Finally, two speech therapists and a linguist – who edited the changes in both linguistic and lexical level – were chosen to check whether the adaptations were adequate and they attested the final Greek version.
Pilot research
The pilot research was conducted from July 2010 to January 2011 in order to define the difficulty of the objects and to verify their accuracy and other characteristics.
Sample
In the current research the examination was administered to 100 adults separately (50 with AD and 50 as control group). The sample selection, although it had uniformity in age, was regardless of origin, marital status and socioeconomic status. It should be noted that in order to successfully administrate the scale and measurements we had to reassure the participants that their personal data would remain confidential and that they would have to sign a participation letter.
Data collection
The administration of the examination took place at the Outpatient Department of the C’ Neurologic Clinic of G.H. Papanikolaou, in the presence of the patients and their caregiver. After the introductions with the test takers we proceeded to the explanation of the purpose of the examination and we asked for their consent by signing the participation letter. Afterwards the test takers were seated in front of a table across and slightly to the right of the examiner. The lighting conditions were appropriate and the materials were placed in such a way that the patients could see and use them without difficulty. The examination was distributed to all participants under the same procedure, and it followed the instructions found in the administrative manual.
During the evaluation the examiner did not change their facial expression or express verbal disapproval. However, in order to obtain the highest performance on the part of the test takers, the examiners tried to encourage them. They were supportive but objective. They would tell the participants when they did well and they calmed them down when they failed. According to Schuell (1964), a simple and honest way to do that, is to comment on reality when the test taker faces a difficulty with a task. This will help the patient relax, get back on track and clear his mind in order to proceed. This is what each examiner should learn. This is not an easy work nor does it aim to simply collect random numbers. The aim is to have the best possible cooperation between the patient and the examiner. There should be successful communication, always with a smile and discussion.
The duration of the examination varies from participant to participant but the average is between 45 to 60 minutes.
Standardness or nonstandardness control of the observations’ distribution for the whole sample as well as the subgroups was done using the Kolmogorov – Smirnov method. The Standardness control showed that our sample had a standard distribution. An independent sample t-test was conducted in order to see whether there is a statistically significant difference between standard witnesses and dementia patients. The analysis gave us the following Table 1.
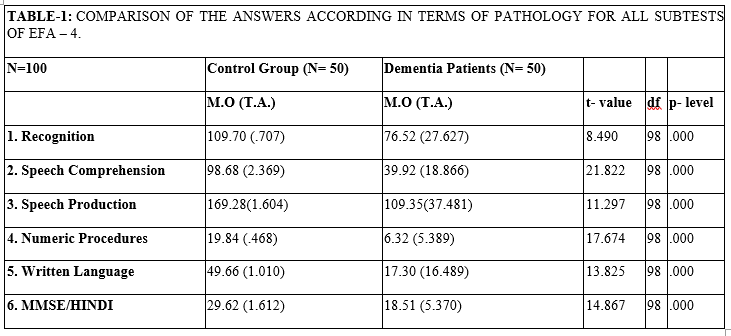
According to Table 1, there were statistically significant differences between the two subgroups in all subtests of the speech scale and MMSE/HINDI. All measurements are attested by the διαστήματα εμπιστοσύνης of the statistical analysis.
In our effort to relate the educational level with pathology separately, in terms of the subtests and MMSE/HINDI scale, we came up with the following Table 2:

Table 2 shows that answers are affected by educational level, but such relation is not statistically significant. In contrast to pathology and MMSE/HINDI, where the relation presents a statistical significance.
In trying to examine whether the stimuli for every scale axis separately affect the final performance, we created a multiple linear model for all stimuli. From the statistical analysis for the pathological sample we came up with Table 3:
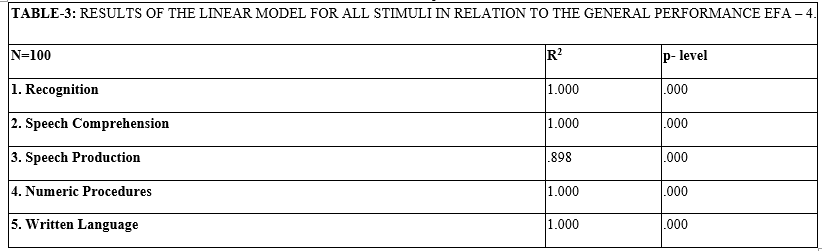
Whether the selection of stimuli affects the parameter of the test that explains the existence of a satisfactory level of promptiness, the above Table gave us statistically significant effects for every scale axis separately, but further improvements are possible.
In order to check the predictive accuracy we used the application of the paired sampled t-test, on the basis of pathology –with which we evaluated the performances for every test thematic – and we examined the possibilities of rejection or verification of our zero hypothesis. The results aresummarized in Tables 4 and 5.
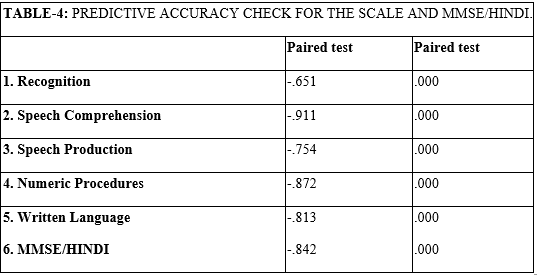
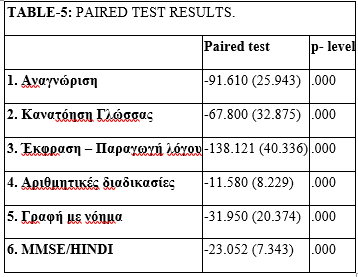
According to the Table above, there are satisfactory levels of accuracy and unequivocal differences on the basis of pathology.
Finally, for the structural validity (or validity of the notional structure) and reliability control, we created the reliability indicator of internal validity – relevance of the thematic indicators alpha Cronbach, split half, and Kuder – Richardson. These results are summarized in Table 6.
As far as the internal relevance control or the uniformity of the scale stimuli are concerned, we calculated the alpha Cronbach’s factor. The analysis provided us with the following:
Reliability Coefficients 5 items Alpha = .924 N of Cases = 100
Another method has to do with internal relevance control or uniformity about scale stimuli the coefficient alpha Cronbach’s splits in half. From this analysis we came up with the following (Table 6):
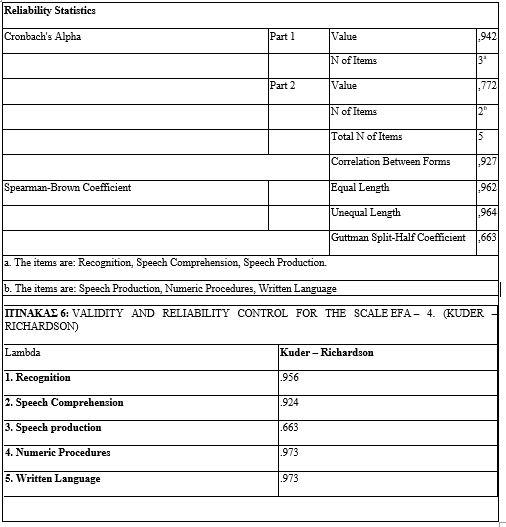
As you can see, the above Table presents satisfactory validity and reliability levels.
The aim of this research was the pilot application of EFA-4 in Greek language to dementia patients. Additionally, our aim was to test whether the selected stimuli can lead to a possible diagnosis of the existence of speech disorders in dementia, as well as the validity and reliability control of the specific test. The results of the research are summarized in the following list:
1. There is a statistically significant difference between the average rate of answers of the control group and the dementia patients, for all EFA-4 axis.
2. There is a statistically significant difference between the average rate of answers between the average rate of answers of the control group and the dementia patients, for MMSE/HINDI.
3. To the question whether educational level affects performance for EFA-4 axis, there was a statistically insignificant inverse correlation effect (due to low educational level of the sample).
4. To the question as to whether pathology affects performance for the EFA-4 axis there was a statistically significant inverse correlation effect (that is, the more advanced the stage is the less effective the performance is for all axis of the test). This effect varied from 65,1% for reading and 91,1% for comprehension.
5. To the question whether there is a relation between MMSE/HINDI scale and EFA-4 axis, the answer is that there is a statistically significant proportional relationship, with a positive correlation of 84,1% for reading and 94,9% for comprehension.
6. As to whether each stimulus separately can -and to what extend- explain the level of each EFA-4 axis, the research showed that they can actually be explained to a high or even absolute degree.
7. To the question whether we have a reliable scale – measuring tool, the research showed that the current form of the scale is actually a highly reliable tool.
8. Finally, to the question whether we have a valid scale – measuring tool, the research showed that for the specific age group the scale is considered a valid tool.
It should be mentioned that there are no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
