
Case Report | DOI: https://doi.org/10.31579/jsrbi.2021/013
*Corresponding Author: SULE Muhammad Baba, Appendicitis Presenting With Peri-Appendiceal Abscess in an Adult Male: Ultrasonographic Findings and Case Report.
Citation: Sule MB, Erinle SA, Umar AU, Gele IH, Joshua GK, Ribah MM, (2021) Appendicitis Presenting With Peri-Appendiceal Abscess in an Adult Male: Ultrasonographic Findings and Case Report. J. Scientific Research and Biomedical Informatics, 2(2); Doi:10.31579/jsrbi.2021/013
Copyright: © 2021 SULE Muhammad Baba, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 March 2021 | Accepted: 09 April 2021 | Published: 14 April 2021
Keywords: appendicitis; abscess; phlegmon; right iliac fossa
Acute appendicitis is defined as inflammation of the vermiform appendix, with about 2% and 6% of these cases presenting as appendiceal mass, often described as inflammatory phlegmon or abscess.
A 45-year-old trader was referred for abdominal and pelvic ultrasound scan on account of right iliac fossa pain, right iliac fossa swelling, vomiting and fever for almost two-weeks duration.
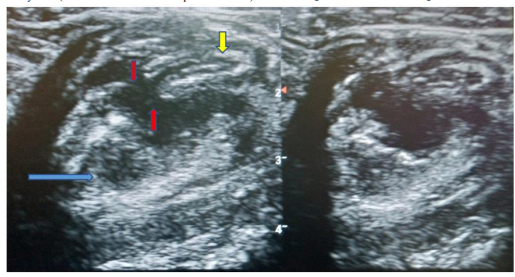
The ultrasonography demonstrated a mass measuring about 37mm x 24mm in dimension with a non-compressible dilated blind-ending tube (7mm) in the right iliac fossa region with sonographic probe tenderness, discontinuity in the anterior and posterior walls more in the posterior wall, with associated collection of heterogeneous reflectivity (abscess)around the areas of discontinuity more posteriorly measuring about 7 milliliters in volume. There is prominence of the peri-cecal fat and associated sentinel loops of bowel around the site most likely from the inflammatory process. The remaining abdominal and pelvic organs show normal appearances.
A diagnosis of acute appendicitis with peri-appendiceal abscess was made ultrasonographically, the patient had emergency appendectomy with abscess drainage, rehydration and antibiotic therapy.
We report a case of acute appendicitis with peri-appendiceal abscess in an adult male with review on the ultrasonographic features.
Acute appendicitis is one of the most common cause of acute abdomen, this has been classified as either uncomplicated and complicated form, and has a life time risk of about 7-8%, with the highest incidence in the second decade [1].
Complicated appendicitis describes the presence of a palpable mass, an appendiceal phlegmon (this is an inflammatory tumor consisting of the inflamed appendix and adjacent viscera with the greater omentum), or localized abscess (a pus-containing appendiceal mass) without distinction [1-3].
Acute appendicitis is often fixed by the patient’s self defense mechanisms either by formation of an inflammatory mass (an appendiceal phlegmon) or a circumscribed abscess (an appendiceal abscess), almost always presenting as a palpable mass days after onset of symptoms, and occurring in about 2-7% of all cases of appendicitis [1,4,5].
An appendiceal abscess is a condition in which an abscess is formed around the appendix as a result of appendiceal perforation or extension of inflammation to the adjacent tissues due to aggravation of appendicitis [6].
Appendicitis is often a common differential diagnosis among the large number of cases presenting in the emergency unit on account of acute abdominal pain, and more common in the male gender with more than 70% of cases presenting in individuals less than 30 years of age [7,8].
The vermiform appendix anatomically has varying location with respect to the caecum and can originate within a 360o circumference around the caecum, this is most likely responsible for the varying form of presentation during appendicitis [7,9].
Appendicitis been regarded as the most common cause of acute abdomen, presents as a triad of pain in the right iliac fossa, fever, and vomiting that often requires surgical intervention10.
Radiological imaging most especially ultrasonography and computed tomography (CT) are vital in making the diagnosis of appendicitis with concomitant complications, CT regarded as most vital, though ultrasonography is more preferred in children (most likely from radiation dose) [1,11-13].
Appendicitis with appendiceal abscess have been managed by nonsurgical and surgical approach, the surgical approach is mainly by appendectomy and regarded the mainstay of treatment with mortality rates of about 0.5-2.4% and 0.07-0.7% for patients with or without perforations [1,14].
Case Report
A 45-year-old trader was referred for abdominal and pelvic ultrasound scan on account of right iliac fossa pain, right iliac fossa swelling, vomiting and fever for almost two-weeks duration.
The patient has had similar right iliac fossa pain in the past with similar symptoms and has had repeated episodes of intake of antibiotics, analgesics and antipyretics on those occasion.
On physical examination, he is febrile to touch, not pale, anicteric, not dehydrated and not in any form of respiratory distress or in any form of altered conscious state. He had some swelling with rebound tenderness over the right iliac fossa and also warm to touch more in the right iliac fossa.
The blood pressure is about 120/80mmHg, pulse rate was about 72 beats/minute, respiratory rate was about 12 cycles/minute. The blood electrolyte, urea and creatinine were also normal (12milligram per deciliter and 1.1milligram per deciliter of blood for urea and creatine respectively).
The patient had result of his packed cell volume (40%), full blood count with differentials showing leukocytosis (13000 white blood cells per microliter) in favor of the lymphocytes (6500 lymphocytes in 1 microliter of blood). The erythrocyte sedimentation rate was also normal (10 millimeters per hour).
The ultrasonography (carried out using both 3.5 and 7MHz transducer probes) demonstrated a mass measuring about 37mm x 24mm in dimension with a non-compressible dilated blind-ending tube (7mm) in the right iliac fossa region with sonographic probe tenderness, discontinuity in the anterior and posterior walls more posteriorly, and associated collection of heterogeneous reflectivity (abscess) around the areas of discontinuity more posteriorly measuring about 7 milliliters in volume (figure 1). There are associated sentinel loops of bowel around the site most likely from the inflammatory process. Prominence of the peri-cecal fat is also demonstrated. The remaining abdominal and pelvic organs show normal appearances.
A diagnosis of acute appendicitis with peri-appendiceal abscess was made ultrasonographically, the patient had emergency appendectomy with abscess drainage, rehydration and antibiotic therapy. The post-operative specimen had no features of malignancy following histology.
The patient spent two-weeks on admission, got better without any complications, he was discharged for follow-up visits after two weeks, following which he was discharged from the clinic.
Discussion
Acute appendicitis is often fixed by the patient’s self defense mechanisms either by formation of an inflammatory mass (an appendiceal phlegmon) or a circumscribed abscess (an appendiceal abscess), almost always presenting as a palpable mass days after onset of symptoms, and occurring in about 2-7% of all cases of appendicitis [1,4,5]. The case under review has clinical and imaging features of acute appendicitis, presented with a palpable right iliac fossa mass and diagnosed ultrasonographically as having peri-appendiceal abscess, thereby conforming to these literatures.
Acute appendicitis is one of the most common cause of acute abdomen, this has been classified as either uncomplicated and complicated form, and has a life time risk of about 7-8%, with the highest incidence in the second decade [1]. The index case is a 45-year-old male, that presented as with features of acute abdomen, with imaging and clinical features of complicated appendicitis; formation of abscess cavity.
Appendicitis often presents with a triad of pain in the right iliac fossa, fever, and vomiting that often requires surgical intervention [10]. The case under review is not an exception, he also presented with right iliac fossa pain and swelling, vomiting and fever, thereby conforming to this literature.
The vermiform appendix anatomically has varying location with respect to the caecum and can originate within a 360o circumference around the caecum, this is most likely responsible for the varying form of presentation during appendicitis [7,9]. The appendix in the index case was retrocecal and diagnosed following examination with both 3.5MHz and 7MHz transducer probes respectively.
Radiological imaging most especially ultrasonography and computed tomography (CT) are vital in making the diagnosis of appendicitis with concomitant complications, CT regarded as most vital [1,11-13]. The index case was diagnosed following ultrasonography, though CT was not carried out on this patient, thereby conforming to these literatures.
Ultrasound imaging is regarded vital in the diagnosis of the appendix with abscess collection, the features are normally non-compressible dilated blind-ending aperistaltic tube, appendicolith, loculated and prominent peri-cecal fluid and prominent peri-cecal fat [10]. The case under review also had most of these features following ultrasonography, and thereby conforming to this literature.
Appendicitis with appendiceal abscess have been managed by nonsurgical and surgical approach, the surgical approach is mainly by appendectomy and regarded the mainstay of treatment with mortality rates of about 0.5-2.4% and 0.07-0.7% for patients with or without perforations [1,14]. The index case had surgical removal of the appendix and drainage of the abscess, thereby conforming to these literatures.
Conclusion
Acute appendicitis is relatively common, patients with features of this condition should be adequately examined clinically and by ultrasonography to prevent onset of complications and rule-out other differentials like malignancies of the appendix.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
