
case report | DOI: https://doi.org/10.31579/2690-1897/188
Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), PMB 5022, Awka. Anambra State, Nigeria.
*Corresponding Author: Nonso Mbah, Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), PMB 5022, Awka. Anambra State, Nigeria.
Citation: Nonso Mbah., (2024), Appendiceal Mucocele: Delayed Presentation, Treatment and Literature Review, J, Surgical Case Reports and Images, 7(3); DOI:10.31579/2690-1897/188
Copyright: © 2024, Nonso Mbah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2024 | Accepted: 18 April 2024 | Published: 26 April 2024
Keywords: mucocele; delayed presentation; appendix; missed diagnosis; uncommon
Appendiceal mucocele is a non-specific term for 4 different pathological conditions of the vermiform appendix in which there’s an abnormal accumulation of mucinous material within the distended appendix. It is an uncommon condition. Missed diagnosis still occurs pre-operatively despite the availability of valuable ancillary imaging facilities. Open meticulous surgical treatment which avoids rupture or spillage of the mucinous content offers the best chance of cure.
Carl von Rokitansky of Vienna, Austria was the first to describe mucocele of the appendix in 1842.1 Since then, 4 different pathological conditions have been recognized to present under this non-specific terminology.2 The common feature in all cases is the abnormal distension of the vermiform appendix due to large accumulation of mucin.
The specific disease states which present as appendiceal mucocele (AM), and their respective incidence (%), are notably:
Mucoceles which are less than 2cm in diameter are usually simple retention cysts while mucosal hyperplasia, mucinous cystadenoma and mucinous cystadenocarcinoma are most likely to be greater than 2cm.2 While AM due to simple retention cyst and mucosal hyperplasia are non-neoplastic, the other 2 are neoplasms. Mucinous cystadenoma is a benign neoplasm with a very good prognosis, occurs with the highest incidence, and has approximately 20% risk of spontaneous rupture. Mucinous cystadenocarcinoma is malignant with the possibility of spontaneous rupture in 6% of cases. It also has poor prognosis with high rate of metastasis to the lymph nodes and liver.3
Being a heterogenous entity, AM has variable clinical presentations. It may be asymptomatic, with the diagnosis made as an incidental finding during imaging studies, or laparoscopic investigation for other abdominal conditions.4 Symptomatic cases may attend with abdominal pain, nausea, poor appetite, vomiting, change in bowel habit, weight loss, abdominal distension, rectal bleed or the presence of a painful palpable mass in the abdomen.3,4 Hospital presentation may either be as an acute condition similar to acute appendicitis, or for chronic symptoms as was the case with our patient.
Sonographic features typically associated with AM are ≥15mm outer diameter of the vermiform appendix and the onion-skin appearance.5 A multidetector CT scanner is the preferred diagnostic imaging modality. Pathognomonic CT findings include a well-encapsulated, rounded or tubular cystic mass adjacent to the caecum, as well as the presence of wall calcifications in 50% of cases.6 Preoperative colonoscopy is also diagnostic of this condition if it shows the peculiar “volcano sign” which is due to the presence of a mount-like elevation of the appendix orifice with a central crater from which yellowish mucoid material exudes.7
A dreaded complication of AM is the rupture or spillage of the mucin-producing epithelial cells within the peritoneal cavity and the attendant risk of developing pseudomyxoma peritonei (PMP). When PMP develops in patients with AM other than those with mucinous cystadenocarcinoma, survival and prognosis are better. By contrast, the prognosis of PMP is worse when associated with the cystadenocarcinoma.8,9
Similarly, AM due to simple retention cyst, mucosal hyperplasia and the benign mucinous cystadenoma have excellent post-operative outcome, with 5-year survival rates of 91 – 100%. Conversely, mucinous cystadenocarcinoma, being the malignant form of AM, has poor prognosis after appendicectomy, with 5-year survival rate of 25%.10
Mrs O. C, 69 years old widow, Para 9, presented at a private health facility in July 2021 with 1- year history of painful abdominal mass lesion. The pain was biting in character with a mild to moderate severity score of 3-5/10. She had associated change in bowel habits characterized by upwards of 2 days of constipation. No associated vomiting or weight loss. The patient reported having a background history of high blood pressure and bilateral knee arthritis. Her regular tablet medications comprised of Amlodipine, Losartan, Hydrochlorothiazide, Digoxin, Clopidogrel, Atorvastatin, Paracetamol and Diclofenac. The past surgical history was unremarkable.
On physical examination, she was afebrile (Temp 36.6oC), BP was 106/84mmHg, PR 90/min. She was moderately obese with a BMI of 34.1 (weight 95kg, height 1.67m). Her abdomen was globally soft and contained a slightly tender, mobile intra-abdominal mass at the right iliac fossa. It was firm in consistency with vague margins. The digital rectal examination was normal.
The pre-operative haematological investigations were unremarkable.
Her abdomino-pelvic sonography reported a mixed solid and cystic right adnexal mass with no definite vascular features and was suggestive of ovarian cyst with intra-cystic haemorrhage.
Computerised tomography (CT) scan report documented a right lower abdominopelvic cystic mass, probably a mesenteric cyst.
The patient was worked up for elective exploratory laparotomy. Intra-operatively, there was an enlarged dumb-bell shaped mass lesion with a wide base at the position of the vermiform appendix at the ileo-caecal junction (fig. 1). There were no visibly enlarged mesenteric lymph nodes. The rest of the abdominal viscera, including the liver, were macroscopically healthy looking.
The tumour was delivered from the abdominal cavity, doubly ligated at the base and excised (figure. 2 and 3). The stump was buried and the laparotomy wound was closed by mass closure. She had 1 unit of blood transfusion intra-operatively. Her post-operative course was uneventful. She was discharged from the hospital on the 4th post-operative day after the restoration of regular bowel movements.
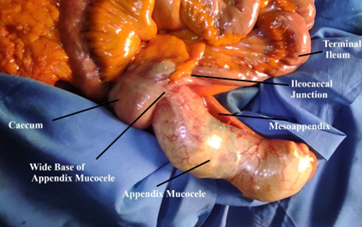
Figure 1: Intra-operative insitu Appendiceal Mucocele.

Figure 2: Ligated base of Appendix Mucocele
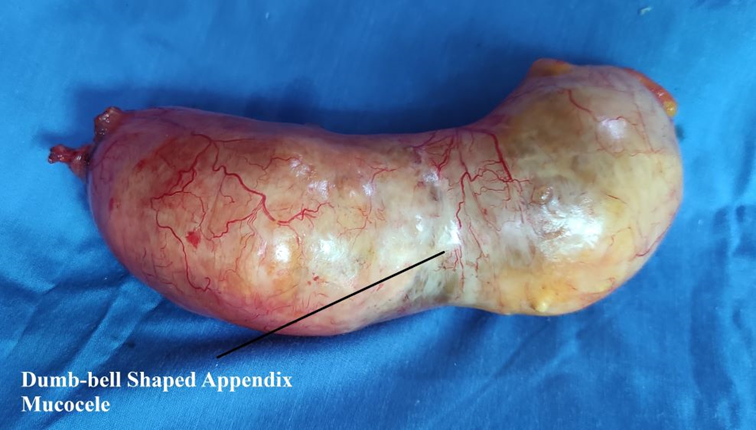
Figure 3: Intact resected dumb-bell shaped Appendiceal Mucocele.
The histology report documented a 15cm x 6cm x 6cm enlarged and cystic appendicectomy tissue which weighed 295g and was filled with mucinous material. It had mucinous epithelial lining associated with dense inflammation on the collagenous wall including inflammatory giant cells. No atypia was noted. Histological diagnosis was Mucinous cystadenoma with foreign body granuloma.
The patient has remained asymptomatic on follow-up 2 years after surgical treatment.
Appendix mucocele is a difficult condition to diagnose. Despite well established sonographic and CT features of AM, the pre-operative diagnosis was completely missed in our case due to the non-familiarity with this condition by the attending sonologists and radiologists. The incidence is 0.2% to 0.7% in all appendicectomy specimens.2 Its rarity necessitates a high index of clinical suspicion and familiarity with the imaging features if cases are not to be missed, both by the radiologists and the clinicians.
The heterogenous nature of AM makes the clinical presentation ambiguous. Cases presenting in emergency rooms as acute appendicitis had previously been reported, even in pregnancy.4,11 Conversely, due to the mildness of the symptoms in some patients, late presentation with symptoms lasting for months, as in the case presented here, abound.12,13 The presence of an abdominal lump could be obvious to both the patient and clinician. In such situations, the differential diagnoses in either gender include mesenteric cyst, intussususception, colonic tumour, and in females may also suggest ovarian cyst, tubal pregnancy, uterine fibroid or tubo-ovarian abscess. Cases of AM which are diagnosed pre-operatively may benefit from surveillance colonoscopy. This investigation facilitates the identification of synchronous and metachronous colonic tumours, which if present would influence the extent of the planned definitive surgical resection.5,6 Our patient didn’t receive colonoscopy, as her AM was discovered intra-operatively.
The intact mucocele does not pose a threat to the patient. Conversely, when it is perforated or ruptured either iatrogenically or due to delayed presentation, there is spillage of the mucin-producing epithelial cells into the peritoneal cavity. This complication is associated with a high probability of precipitating pseudomyxoma peritonei, a potentially
catastrophic condition for which treatment is problematic and long term results are unsatisfactory.8 It is for these reasons that the open surgical
approach is favoured by many surgeons over the laparoscopic technique, for the resection of AM.14 The advantages of the open operation include meticulous tactile tissue handling and the opportunity to directly inspect parts of the abdominal cavity where mucinous tumours are most common. The favourable outcome of our case was predicated not only on the benign mucinous cystadenoma histology of her AM, but also on the use of laparotomy for her treatment which ensured the mucocele was not ruptured iatrogenically. However, recent reports posit that the operation for AM can alternatively be performed laparoscopically, both safely and successfully, by adhering to safety rules which include the use of an endobag to remove the mucocele and ensuring the conduct of the procedure by a surgeon who is experienced in advanced laparoscopy.15
In conclusion, a high index of clinical suspicion and familiarity with the characteristic imaging features are required for the pre-operative diagnosis of appendiceal mucocele by both the radiologist and clinician. Meticulous surgical technique is mandatory during the resection of the lesion in order to avoid iatrogenic rupture and the precipitation of such catastrophic complication as pseudomyxoma peritonei.
None.
None.
This case report is exempt from ethical approval in our institution.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
