
case report | DOI: https://doi.org/10.31579/2639-4162/070
Department of Psychiatry, Azerbaijan Medical University
*Corresponding Author: Karimova R.Z, Department of Psychiatry, Azerbaijan Medical University
Citation: Karimova R.Z, (2022) Antipsychotics For Psychosis In People With Vascular Dementia. General medicine and Clinical Practice, 5(4); DOI: 10.31579/2639-4162/070
Copyright: © 2022 Karimova R.Z, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 June 2022 | Accepted: 22 July 2022 | Published: 12 August 2022
Keywords: vascular dementia; psychotic symptoms; delusions; hallucinations; neuroleptics
In the clinic of dementia, not only cognitive, but also non-cognitive disorders are observed. In the treatment of these symptoms, the use of antipsychotics is necessary. As the etiology and pathogenesis of vascular dementia, which is a type of dementia, is multifactorial, it requires more careful treatment while treating with antipsychotics. The aim of the study was to study the effectiveness of neuroleptics used in the treatment of psychotic disorders in vascular dementia. This article describes which symptoms respond best to antipsychotic treatment and which side effects are more common during treatment. The study showed that psychotic symptoms (delusions, hallucinations), which are the main target of antipsychotics, respond less well to treatment than other symptoms. We hope that this article will help doctors choose the right tactics for the treatment of vascular dementia.
Dementia is a disorder of the upper cortex as a result of chronic and progressive disease of the brain. As the other types of dementia, the main symptom of vascular dementia is cognitive impairment. In many cases, along with cognitive decline, non-cognitive symptoms are also observed. Although the main focus and treatment is against cognitive decline, it is the non-cognitive symptoms that bother patients and those caring for them. The frequency of non-cognitive impairments in different types of dementia is also different [1,3, 5,11,12]. In vascular dementia, 1 psychopathological symptom is observed in 81.1% of cases, and 2 or more symptoms are observed in 15% of cases. There were reports of apathy in 56.6% anxiety and agitation in 18.9%, delusions in 14-27%, hallucinations in 5-14%, depression and disinhibition in 5.6%. of patients [7-10]. However, in any case, those who care for the patient are more concerned about psychopathological symptoms than the decline in cognitive function. Psychiatrists are often consulted for these symptoms.
Basic therapy for vascular dementia both prevents and affects the development of psychotic disorders. Sometimes such psychotic symptoms can develop and worsen against the background of basic therapy [6]. To date, the use of neuroleptics is not recommended due to the etiology and pathogenesis of dementia [4]. Randomized placebo studies have not been able to prove the effect of antipsychotics on behavior and psychotic symptoms. Thus, in the meta-analysis of 15 randomized studies and in the meta-analysis of 42 placebo-controlled studies, many neuroleptics were compared, and it was found that treatment discontinuation was more common because the expected effect was not achieved [6]. Unfortunately, most of these studies have been performed on patients with other types of dementia. More research is needed to investigate the use of neuroleptics in vascular dementia. Despite the relative effectiveness of neuroleptics in the treatment of behavioral problems and mental disorders in vascular dementia, we face serious safety shortcomings. Taking neuroleptics in itself increases the risk of cardiovascular complications (stroke, heart attack, lethal outcome). Also, in patients receiving neuroleptics, prolonged QT interval on the ECG, decreased cognitive function, decreased daily activity due to sedation and extrapyramidal effects, difficulty in care, deaths [2]. However, in many cases, given the severity of psychotic and behavioral disorders, the use of neuroleptics is necessary by comparing risk and benefit.
To assess the effectiveness and safety of antipsychotics for the treatment of psychosis in people with vascular dementia
The study was conducted at the Republican Psychiatric Hospital of the Ministry of Health of the Republic of Azerbaijan in 2019-2022. The study included patients who had been treated for "vascular dementia with psychotic disorders" over the years. Patients with mild dementia and various degrees of psychotic disorders were selected according to the requirements of the study. Patients with moderate and severe dementia were excluded from the study on the advice of the Ethical Committee of the Azerbaijan Medical University. Patients with other types of dementia who had vascular dementia and no psychotic sympathy were not included in the study. Patients with previous diagnoses of schizophrenia, schizoaffective disorder, delirium, bipolar disorder, cognitive decline after Intracranial injury, persistent delirium, and other types of dementia were also excluded from the study. As the research was conducted during the Covid-19 pandemic, we faced many problems and limitations. During this period, there was a decrease in the number of patients admitted to the hospital. Patients were treated as much as possible on an outpatient basis. This was a decision taken to reduce their incidence of covid-19 virus. The psychotic condition of all admitted patients was acute. Therefore, it was difficult to compare the severity of non-cognitive symptoms in patients with vascular dementia. Because the scores of the patients on the scales were very close to each other. However, this helped us to avoid many of the mistakes that can be made when evaluating the course and outcome of treatment. Since the degree of expression, degree of distress, and severity of acute psychotic symptoms are almost the same, we think that we have more accurately measured the effectiveness of the drugs we used in treatment.
All patients included in the study were examined by a therapist and a neurologist and, if necessary, referred to a cardiologist, endocrinologist and surgeon. A Mini-Mental State Examination (MMSI) scale and a modified Khachinsky ischemia assessment scale were completed for the patient to be included in the study. Patients who scored 20-23 on the MMSI scale (mild dementia) and more than 7 on the other scale were included in the study. Brief Psychiatric Rating Scale (BPRS) and Neuropsychiatric Inventory (NPI) were completed for each patient before and 4 weeks after treatment. The dose was reduced when side effects were observed during the study. When side effects did not end and the patient was disturbed, he/she was excluded from the study with the patient's consent. The decision to continue treatment and research during the study was voluntary by the patient and his / her relatives. He/she was excluded from the study at their request. The data were statistically processed to objectively evaluate all the data obtained.
77 patients participated in the study. Their mean age was 72.3 ± 0.9 (57-91). The social demographic indicators of the patients are given in the table (Table 1).
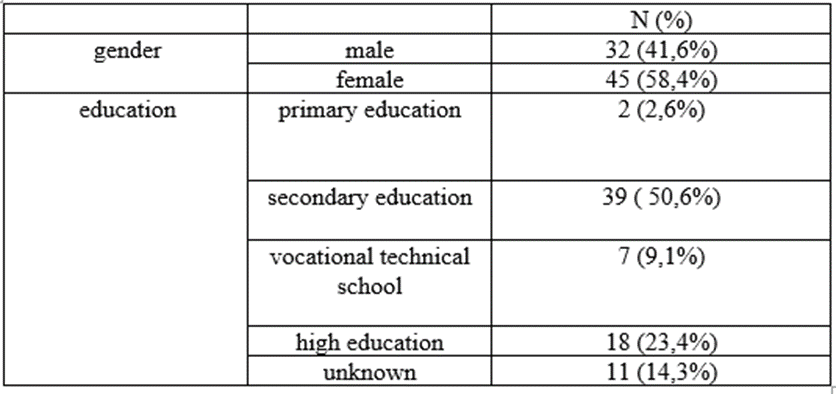
Table 1.Socio-demographic indicators of patients participating in the study
The average score of patients on the MMSI (Mini-Mental State Examination) scale was 20.4 ± 0.4. The average score on Khachinsky's modified schedule of ischemia was 11.8 ± 0.4. As noted, two scales were used to study the dynamics of non-cognitive symptoms: the Brief Psychiatric Rating Scale (BPRS) and the Neuropsychiatric Inventory (NPI). The use of the NPI scale in the evaluation of the diagnosis and treatment of dementia and neurodegenerative diseases was both more convenient and allowed to assess the symptoms observed only in dementia. Thus, the NPI scale is completed by the clinician in a short period of time based on the information provided by the patient. This scale is considered a validated asset. The NPI scale covers 12 symptoms. These include: delusions, hallucinations, aggression / agitation, depression / dysphoria, anxiety, euphoria, apathy, disinhibition (impulsive and thoughtless actions), lability, aberrant / motor behavior, sleep and nightime behavior disorders, appetite and eating disorders. First of all, it is clarified whether there are any symptoms in the last 4 weeks. If the answer is positive, the frequency of symptoms, the degree of expression, the degree of distress are evaluated [20-26].
Frequency is rated as:
1 - Occasionally - less than once per week
2 - Often - about once per week
3 - Frequently - several times per week but less than every day
4 - Very frequently - daily or essentially continuously present
Severity is rated as:
1 - Mild - produces little distress in the patient
2 - Moderate - more disturbing to the patient but can be redirected by the caregiver
3 - Severe - very disturbing to the patient and difficult to redirect
The score for each domain is: domain score = frequency x severity
Distress is scored as:
0 - no distress
1- minimal
2 - mild
3 - moderate
4 - moderately severe
5 - very severe or extreme.
Prior to treatment, the mean score on the NPI scale was 58.7 ± 2.0 (23-106), and in the 4th week of treatment it dropped to 13.9 ± 1.8 (0-64). In other words, a decrease of 76.3 Perecntage was recorded in the total scores. Before treatment for BPRS, the score was 33.4 ± 1.4 (9-67), and then 14.2 ± 1.2 (3-48). There is a 57.3 Perecntage decrease in scores on this scale. If the decrease between pre- and post-treatment scores on the NPI scale is more than 30 Perecntage, it is considered that there is a positive dynamics in the course of symptoms, and neuroleptics are effective. Based on this rule, the degree of expression, degree of distress and frequency of occurrence of each symptom were calculated separately. In order to more clearly observe the effectiveness of neuroleptics, it was assumed that the change in scores had a treatment effect if it was more than 30 Perecntage, and that the treatment effect was small if it was less than 30 Perecntage. Cases of no change in scores were also investigated. We think that such a conditional separation allows us to draw more accurate conclusions (Table 2).

Table 2. Dynamics of scores on the scales used
The table below shows the scores of the NPI scale before and 4 weeks after treatment (Figure 1).
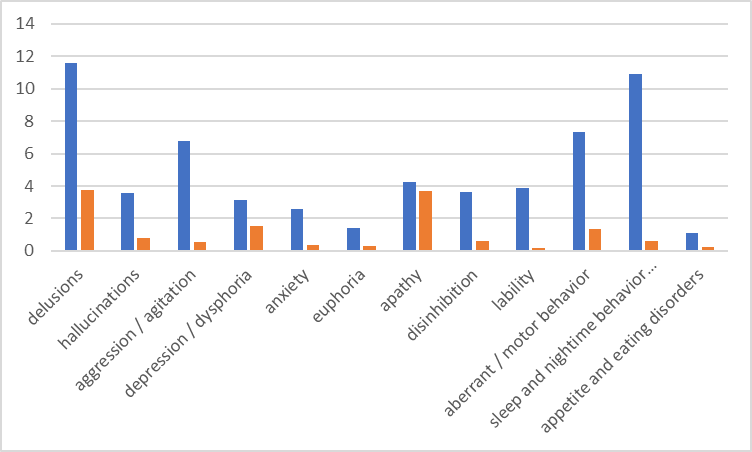
Figure 1. Changes in the overall symptom score on the NPI scale before and 4 weeks after treatment .
Assessing the degree of expression, distress, and frequency of each symptom on the NPI scale allowed us to study the effects of neuroleptics in more detail. The regression to assess changes in symptom scores and symptom dynamics on the NPI scale and BPRS scale was calculated in the following tables. (Table 3. and Table 4.).

Table 3. Dynamics of symptoms on the NPI scale

Table 4. Dynamics of indicators on the brief psychiatric assessment schedule
As noted, a modified Khachinsky ischemia assessment scale was completed for each patient prior to treatment. The primary goal in filling this scale was to differentiate vascular dementia from Alzheimer's dementia by studying the degree of ischemic brain damage. Patients included in the study had to score at least 7 points on this scale. Elevated scores were an indication of higher ischemic changes in the brain. This fact was confirmed by a neurologist's examination and MRI. We also tried to study the effect of neuroleptics on the degree of ischemic brain damage. In other words, the study of how pathological changes in the brain in vascular dementia affected the course and outcome of treatment. A very weak negative correlation was observed between the scores of the Khachinsky scale and the indicators (p> 0.05). As the main goal of the study was to study the effectiveness of neuroleptics in the treatment of psychotic symptoms, more attention was paid to these 2 symptom-delusions and hallucinations (Table 5).
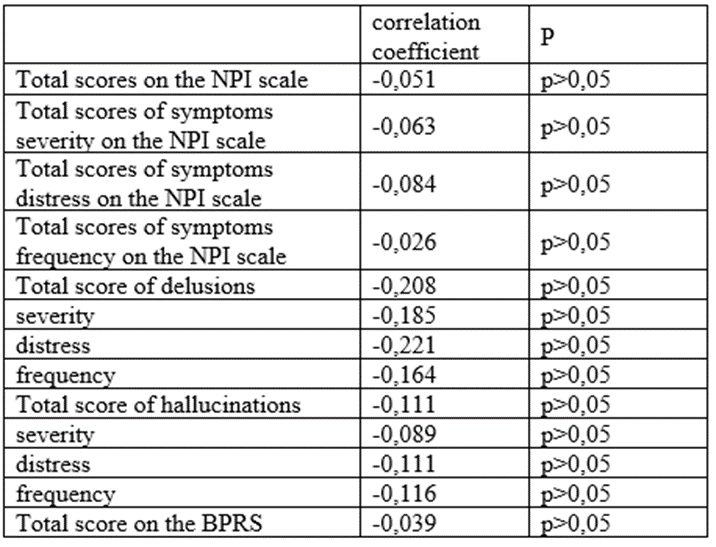
Table 5. Correlation coefficient between the scores of the Khachinsky scale and the scores of the NPI and BPRS scale.
On the NPI scale, delusions are assessed on item 1, and hallucinations are assessed on item 2. Because the degree of symptom distress is based on the subjective feelings of the caregiver and the physician and his or her ability to manage those symptoms, it does not allow an objective assessment of changes in symptom consciousness before and 4 weeks after treatment. In order to calculate the severity of each symptom separately, as expressed in the guidelines of the NPI scale, it is necessary to multiply the degree of expression of the symptom and the frequency of occurrence. Based on this suggestion, we decided to calculate the severity of each symptom before and after treatment. This will allow us to study the severity of non-cognitive symptoms observed in the clinic of vascular dementia. It will also allow us to evaluate the effectiveness of neuroleptics in the treatment of psychotic symptoms. A 30 Perecntage decrease in total scores on the NPI scale indicates that treatment is effective. In this way, it is possible to calculate the decrease in points for each symptom. However, in order to more clearly observe the dynamics of individual symptoms, we consider the above method more appropriate.
As can be seen from the table, in two of the 77 patients on the NPI scale, no delusions were observed before treatment. In 2 out of 75 patients, delusions are moderate (6-8 points). In 73 patients, delusions were sharply expressed and assessed as severe. After 4 weeks of treatment with neuroleptics, no delirium was observed in 35 patients (47.9 Perecntage). In 18 patients (24.7 Perecntage) the symptoms were moderate. In 7 patients, the effect of neuroleptics in the treatment of delusions was not observed. We see interesting results in the observation of the dynamics of hallucinations on the NPI scale. Thus, hallucinations are not observed in 53 (68.8 Perecntage) of 77 patients who applied to the hospital in acute psychotic will. Hallucinations are mild in one of 24 patients, moderate in 2 patients. Severe dementia was reported in 21 patients. In the 4th week of treatment with neuroleptics, hallucinations were not observed in 66 patients. In other words, 13 out of 21 patients recovered. It is assessed as mild in 5 patienlets. In only 2 patients, the effect of neuroleptics in the treatment of hallucinations was not observed (Table 6 and 7).
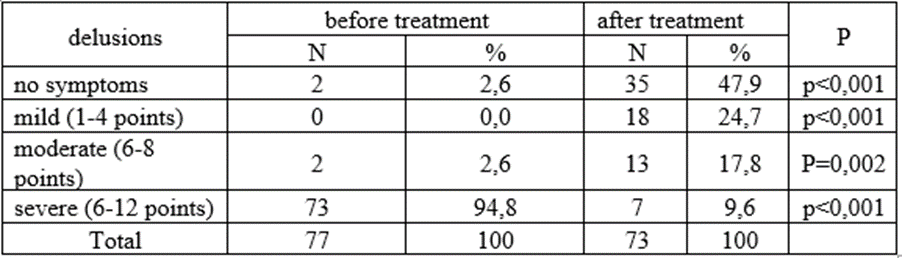
Table 6. The severity of delusions.

Table 7. The severity of hallucinations.
Numerous studies have shown that the use of neuroleptics is life-threatening and often unreasonable for patients with dementia. It was also found that there were more cases of discontinuation of treatment due to the lack of effect of treatment with neuroleptics. Aging is itself a modified pharmacokinetics and pharmacodynamics. Because psycho-pharmacology is very specific in the elderly, the development of side effects of psychotropic drugs is also different. One of the most important issues for us is to study the side effects of psychotropic drugs in the elderly population, which complicate treatment and sometimes even lead to death. The situation is even more difficult with vascular dementia. Despite the relative effectiveness of neuroleptics in the treatment of behavioral problems and mental disorders, we face serious shortcomings in terms of safety. In general, the use of neuroleptics increases the risk of cardiovascular complications. In patients receiving this group of drugs, prolonged QT interval on the ECG, decreased cognitive function, decreased daily activity due to sedation and extrapyramidal effects, and maintenance difficulties. However, in many cases, the use of neuroleptics is necessary by comparing the risks and benefits. It is very important to know in advance which patients will develop side effects during treatment. With this in mind, we also studied the side effects of neuroleptics in our study. The study found that side effects were more common in patients with high Khachinsky scores (Table 8). Side effects observed during treatment were: parkinsonism, muscle weakness, hypotension, convulsions, urination, drowsiness, gait changes (Table 9).
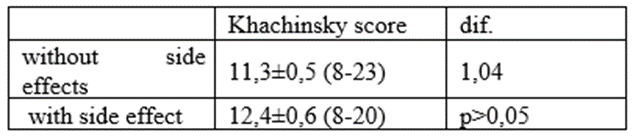
Table 8. Correlation between scores on the Khachinsky scale and observation of side effects.
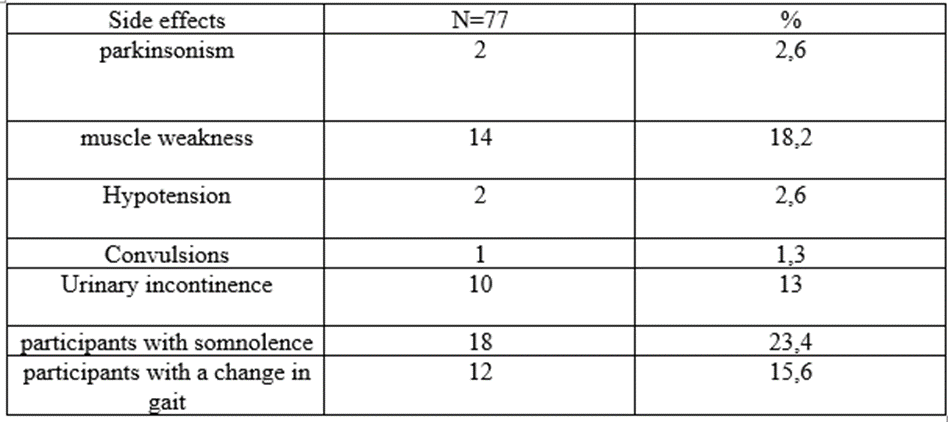
Table 9. Side effects observed in patients
The study involved 77 patients, 32 (41.6 Perecntage) men and 45 (58.4 Perecntage) women. Subjectively, 19 (24.7 Perecntage) patients recovered psychotic symptoms and 48 (62.3 Perecntage) patients improved their condition. In 10 patients, no change in psychotic symptoms was observed during the first 4 weeks of neuroleptic treatment. In 4 of these 10 patients, treatment was discontinued within 4 weeks on the advice of a physician, as the side effects were significant and the severity and number of side effects increased while taking the neuroleptic. In the other 3 patients, no improvement was observed during 4 weeks of treatment. After 4 weeks, the dose was increased, but an increase in side effects was observed. On the advice of a doctor and with the consent of the patient, the patient's relatives were transferred to another neuroleptic. One patient completed 4 weeks of treatment, but as there was no change in psychotic symptoms as a result of treatment, the patient left the study at the patient's request and was transferred to another type of neuroleptics. Two patients with no change in subsequent psychotic symptoms continued the treatment with an increase in dose for 4 weeks. Of course, these percentages could be subjective. In many cases, subjective and objective assessments do not coincide. To do this, we assessed the patient's initial condition, the course of treatment and the results with the help of jokes. We compared the obtained results on the basis of statistical calculations. Four patients died during the study. Two of them died of complications of the covid-19 virus, and the other two died of concomitant cardiac diseases, despite constant medical supervision. The results of the treatment are presented in the table below (Table 10).

Table 10. Outcome of treatment of psychotic symptoms observed in vascular dementia.
The main reason for VaD patients to go to a psychiatric hospital is psychotic symptoms. According to the NPI scale, delusions, motor disorders, and sleep disorders score higher. This means that these symptoms are more pronounced in vascular dementia. During the first 4 weeks of treatment with neuroleptics, lability, sleep disorders, aggression respond better. Given that a 30 Perecntage decrease in scales was noted as an improvement, there was no improvement in apathy with neuroleptics. Depressive symptoms improved by 50.7 Perecntage. Although the scores of delusions and hallucinations were higher than the scores of other symptoms at the initial examination, after treatment, the scores decreased by 67.3 Perecntage and 78.1 Perecntage, respectively. Unfortunately, psychotic symptoms (delusions, hallucinations), which are the main target of neuroleptics, respond less well to treatment than other symptoms. Side effects are more common in patients with more ischemic brain damage. Eight out of 77 patients refused treatment due to side effects. However, in many cases it is necessary to use neuroleptics by measuring the phase of harm and benefit. In this case, it is recommended to start with a small dose and gradually increase the dose. It is advisable to keep the dose as small as possible even during the first 4 weeks. This will both reduce the development of side effects that can lead to treatment rejection and reduce mortality.
This study has some limitations. This study was not intended to assess regional differences. Despite the obvious limitation of this study due to the small number of samples, we can argue that it shows promising data.
The article carried out by own financial resource.
Authordeclare that the manuscript is submitted on behalf of all author. None of the materialin this manuscript has been published previously in any form and none of the material is currently under consideration for publication elsewhere other than noted in the cover letter to the editor.Author declare to have any financial and personal relationship with other people or organizations that could inappropriately influence this work. Author contributed to and have approved the final manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
