
Research Article | DOI: https://doi.org/10.31579/2694-0248/048
1 Pharmacy Department, The Royal Melbourne Hospital, Melbourne, VIC, Australia.
2 Melbourne Epicentre, The Royal Melbourne Hospital, Melbourne, VIC, Australia.
3 University of Melbourne, Statistics and Data Science, Melbourne, VIC, Australia.
*Corresponding Author: Van N. Tran, Orthopaedic Clinical Pharmacist, The Royal Melbourne Hospital: City Campus Pharmacy Department Grattan Street, Parkville Victoria Australia 3050.
Citation: Van N. Tran, Brennan J. Fitzpatrick and Sourav Das, (2022), Antiemetics and Apfel Scores in Orthopaedic Surgery, J Clinical Orthopaedics and Trauma Care, 4(5); DOI: 10.31579/2694-0248/048
Copyright: © 2022, Van N. Tran. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 June 2022 | Accepted: 01 August 2022 | Published: 30 August 2022
Keywords: Apfel score; surgery; patients; post-operative nausea and vomiting; antiemetic agents; perioperative medicine; orthopaedics
Background: Postoperative nausea and vomiting (PONV) is a common complication following orthopaedic surgery. Only a few risk factors have consistently been reported to be independent predictors for PONV.
Aim: To report Apfel scores for orthopaedic patients then correlate these scores to the number of antiemetics prescribed and subsequently administered in both the perioperative and post operative setting and determine if screening for Apfel scores is beneficial to predict PONV.
Methods: A retrospective analysis of patients admitted under orthopaedic units between 1st July2019 and 31st July 2019 was conducted at a tertiary teaching hospital in Australia. Patients were screened and allocated an Apfel score and antiemetics agents prescribed and subsequently administered were recorded.
Results: A total of 115 patients were screened for inclusion. Of these four patients met this exclusion criteria, resulting in a total sample size of 111 patients. An Apfel score of two was reported in 45.0% of patients, followed by 28.8%of patients scoring three, with 12.6% scoring one. Only 5.4% of patients scored the highest risk of four, with 8.2% of patients with no Apfel score documented.
Conclusion: Orthopaedic patients tend to score two or more in their Apfel score placing them at higher risk of postoperative nausea and/or vomiting according to the collectively validated Apfel’s simplified risk score. There was no statistically significant relationship between theApfel score and the number of antiemetic agents prescribed or administered from both the perioperative and post-operative setting following orthopaedic surgery in this cohort of adult patients.
Postoperative nausea and vomiting (PONV) is a significant complication that has been commonly reported following surgery [1]. In Australia approximately 10.6 million people were hospitalised during 2016-2017 [2]. One in four of these patients required surgical procedures. Approximately 30% of all post-surgical patients and up to 80% of those classified as high risk of PONV patients will develop symptoms of nausea and/or vomiting following some degree of surgical intervention [3].
PONV is defined as any nausea, retching or vomiting occurring during the first 24-48 hours post-surgical procedure [3]. Unresolved nausea and vomiting are often associated with a delay in recovery following a surgical procedure [4]. In adults, only a few risk factors have consistently been shown to be independent predictors for PONV. These include patient-related factors such as female gender, non-smoking status, history of PONV and postoperative opioids usage. Collectively these risk factors are known to be incorporated in the Apfel score [5].
Apfel et al. established these risk factors by analysing prospectively collected data on patients from two centres of different countries who underwent general anaesthesia with volatile anaesthetics [6]. Apfel et al. concluded that these established patient specific risk factors could therefore be used to predict PONV in patients worldwide [6]. Studies investigating the relationship between the type of surgery and incidence of PONV have reported conflicting results [7]. Orthopaedic surgery is generally considered high risk of PONV due to extensive bone manipulation, high opioid usage, frequency of high-risk patients and prolonged general anaesthetic exposure [8].
Identifying high risk patients and ensuring that they are given appropriate prophylactic antiemetic agents during the surgery is considered best practice in preventing PONV [1). This audit will report Apfel score for orthopaedic patients then correlate these scores to the number of antiemetics prescribed and subsequently administered during surgery, in the post-anaesthetic care unit (PACU) and post-operatively in the surgical ward.
Study design:
An inpatient retrospective audit was conducted at a major tertiary teaching hospital in Australia. Patients were asked if they had a history of PONV during their routine medication history consultation during the audit period, which was recorded via the template sticker (Refer to Appendix A) and filed in patient medical records. Data was then collected by reviewing patients’ electronic medical records in the following month. Patients were included in the four-week audit period if they underwent orthopaedic surgical management. Ethics approval was obtained by the ethics approval committee at The Royal Melbourne Hospital: Office of Research, Melbourne Health (ref QA2018046).
Inclusion criteria:
Patients were eligible for inclusion in the audit if they were admitted between 1st July 2019 to 31st July 2019, under specific orthopaedics codes (ORTHO, ORTHS, ORTHM) and under went a surgical procedure as retrieved from the hospital’s central database patient management system. Bone related operative intervention under the units of general orthopaedics (ORTHO), spinal related surgeries (ORTHS) or high risk orthomedical (ORTHM) patients, were all collectively categorised as orthopaedic surgery.
Exclusion criteria:
Patients were excluded if one or more of the following criteria were met: continual repeated antiemetics prescribed during hospital stay; patients under the age of 16;intensive care unit (ICU) admission; chemotherapy treatment; non-operative management (conservative management); deceased during the admission. A chemotherapy agent is defined as specific chemical agents or drugs that are selectively destructive to malignant cells and tissues used for the treatment of cancer [9].
Outcome measures:
The primary outcome was the distribution of Apfel score, a measure of risk of PONV. The secondary outcome was to determine if there was a correlation between Apfel score and the number of antiemetic prescribed and Apfel score and the number of antiemetic administered during surgery, in PACU or post-operatively on the surgical ward.
Data Collection:
Data was obtained through collecting patient information from medical records via electronic contents manager and pathology viewer program. Data was examined and entered via the Research Electronic Data Capture: RED cap® [10] tool by two auditors, to maintain reproducibility and to strengthen the auditing process via reduction in potential for measurement bias. The clinical pharmacist of the unit screened and completed the Apfel score for orthopaedic patients for the audit period. Auditors screened the anaesthetic record forms for peri-operative antiemetic data and the national inpatient medication chart for prescriptions of antiemetic agents and number of these orders administered for post-operative data.
Data Analysis:
Results from the data collection tool were analysed manually and using pivot tables in Microsoft Excel. The data was analysed to obtain the agents and number of patients prescribed and administered each antiemetic (when required) post-operatively. Patient characteristics were recorded (Refer to table 1) to display the cohort of patients that were included.
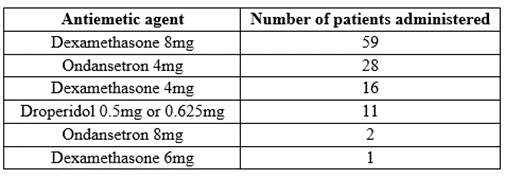
Table 1: Patient characteristics
Statistical analyses were performed using the IBM SPSS statistical software[11]. The association between prescription of antiemetic drugs for the ward setting and Apfel score is shown in (Graph1). In Table 2, we present the parameter estimatesand corresponding odds ratios of a logistic regressionwith dichotomized dependent variable, prescription of antiemetic drugs, with Apfel score as covariates [12]. A poisson log-linear regression model is used to study the association between the number of prescribed antiemetic drugs versus Apfel scores.

Graph 1: Bar plots show the distribution of number of antiemetic agents’ vs Apfel Score

Table 2: Anti-emetic agents administered during surgery.
A total of 115 patients were screened for inclusion from 1st July 2019 to 31st of July 2019. Of these four patients met the exclusion criteria, resulting in 111 patients included in this audit (Refer to Figure 1: Flow diagram).

Flow Diagram
Patient characteristics
Patient characteristics are summarised in Table 1. The sample size included 55.8 % males and 44.2% females. Female median age was 56 with males slighter younger at 48. Males were heavier (average weight 87.6kg) compared to females (average weight 76.5kg),with one male patient in excess of 145kg, influencing the overall average weight. Females were shorter by comparison to males and were slightly less (1.2%) likely to smoke.
Females had more co morbidities but proportionately lower history of PONV (Refer to Table1).
Apfel Score
An Apfel score of two was reported in 45.0% of patients, followed by 28.8% of patients scoring three, with 12.6% scoring one. Only 5.4% of patients scored the highest risk of four, with 8.2% of patients with no Apfel score documented (Refer to Graph 1).
Number of antiemetic agents prescribed and administered in theatres
A higher proportion of patients included in the study had an ApfelScore of two. Of these a high majority received at least one intraoperative agent. But the administration of at least one medication agent was disproportionately higher for the Apfel score two.
Compared to the Apfel score of zero we did not see a significant increase in medications prescribed for the other Apfel score groupings (refer Graph 2). All patients with an Apfel score of 2 received at least one intraoperative agent with 33% of these patients receiving more than one prophylactic antiemetic agent. Of the patients with an Apfel score greater than or equal to 3, 47% received more than a single intraoperative antiemetic agent (Refer to Graph 2).

Graph 2: Number of agents administered peri-operatively (prophylaxis)
Post-operatively in PACU patients were prescribed a mean of 1 antiemetic, 93% of anti- emetic orders in PACU were ondansetron (Refer to Graph 3). A total of 14 patients required at administration of at least one anti-emetic for PONV treatment in PACU (Referto Graph 4).

Graph 3: Number of antiemetic prescribed for PACU

Graph 4: Number of antiemetic administered in PACU
In the theatre setting, dexamethasone 8mg was the most commonly administered agents for PONV prophylaxis, followed by ondansetron 4mg. Droperidol at various doses was the least common agent administered in a theatre setting (Refer to Table 2).
Number of antiemetic agents prescribed and administered in the ward setting.
Most audited patients (n=61) were prescribed only one antiemetic agent, followed by 42 patients who were prescribed for two antiemetic agents, with only four patients that had three agents prescribed. There were four patients that did not have any antiemetics prescribed.
Ondansetron was the most commonly administrated antiemetic agent in the ward setting. A total of 21 patients were given only a single dose, followed by 13 patients who were given two doses, with eight patients given 3 or more doses, of which 1 of these patients was administrated 14 doses in total.
Metoclopramide was the second most commonly administrated antiemetic agent. A total of 6 patients were given one dose, two patients were given two doses, with only one patient who was given three doses. There were nil documented doses administered for domperidone, prochlorperazine or cyclizine in this cohort.
Overall, there was no significant association demonstrated between prescription of antiemetic drugs with Apfel score (Refer to Figure 1: Bar plots show the distribution of number of antiemetic agents vs Apfel score). The data shows that there is a sharp jump in the prescription of one antiemetic agent for patients with an Apfel score of two. However the rate of increase in the number of drugs prescribed is not consistent across Apfel scores. Also antiemetic prescription rates decline both above and below the Apfel score of two.
The observation that there is a greater incidence of PONV in women is purported to be related to hormone fluctuations; particularly variations in progesterone and gonadotrophin (follicle stimulating hormone and luteinising hormone)levels (13). Our study had a relatively even number of males and females eliminating the potential bias of gender over-representation.
Several mechanisms have been postulated for the favorable outcomes produced by cigarette smoke. Firstly, it is possible that tobacco contains an anti-emetic substance providing relief from PONV. However, no such substance has been found to date.
Tolerance to nicotine, which is an emetogenic substance, is another plausible hypothesis. Other possible mechanisms include: effect of smoking on the dopaminergic system which plays an important role in the pathophysiology of nausea and vomiting and the effect of environmental pollutants and chemicals that are present in cigarette smoke which can actas potent inducers of liver enzymes (6, 14). It has been proposed that recovery from anaesthesia, including recovery from PONV, could be enhanced by inducing those enzymes that are responsible for the metabolism of anaesthetic agents (6). In this study, approximately 70% patients were non-smokers, evenly distributed amongst male and female participants.
Higher cortical centres such as the limbic system can also be involved especially if the patient has a history of PONV (15). They promote nausea and vomiting associated with unpleasant taste, sight, smell, memory and fear. Patients who have experienced motion sickness or PONV in the past have a well-developed reflex arc which increases their risk of experiencing PONV (15).
Although this study did not report data on opioids, nausea and vomiting induced by opioid use is a well-known effect attributable to agonist activity in both central and peripheral nervous systems (16). Low doses of opioids activate µ-opioid receptors located in the chemoreceptor trigger zone which is involved in nausea and vomiting (17). It has been hypothesized that opioids can also directly act on the vestibular apparatus and increasing the vestibular sensitivity (18). Since the vestibular apparatus has a direct input to the vomiting centre, it is considered to be a significant pathway in the stimulation of opioid induced nausea and vomiting (19). It is appreciated that opioid induced nausea and vomiting is a complex phenomenon involving different pathways with mechanisms of actions still unknown for some (16).
Long and complicated surgeries will often involve more extensive use of anaesthetics resulting in more post-operative complications such as PONV. Future studies could investigate the importance of these other significant factors in causing PONV.
There is also potential for this study to expand into other speciality units such as laparoscopy, plastic surgery, otorhinolaryngology, urology, neurosurgery, ophthalmology and gynaecology before extrapolating the results found in this study to other speciality units (20).
This study had a small sample size of 111 patients in total. Of these patients, 8% did not have their risk score assessed and therefore, were excluded from further analysis Due to the small sample size statistical significance of the relationship between Apfel score and requirement for treatment in PACU could not be determined. Bigger studies conducted across multiple centres are required to test reproducibility and therefore confirm validity of the results found in this smaller study.
There is a vast amount of evidence to suggest that prophylactic use of antiemetic agents pre-surgery can reduce the incidence of PONV especially in patients who are considered high risk. Further studies are required to establish the Apfel score as a risk factor tool in the pre-operative setting.
For intra-operative antiemetic prophylaxis, dexamethasone was the most commonly administered agent, a reflection of recommended guidelines (1). In patients at higher risk of PONV with an Apfel score greater than two, national and local guidance recommends the administration of at least two anti-emetics during surgery. During our study period only 47% of patients received at least two anti-emetic agents for PONV prophylaxis despite an Apfel score greater than two.
Ondansetron is a 5HT3 antagonist, which was the most commonly prescribed anti-emetic agent during the study period followed by metoclopramide (dopamine antagonist). Other agents such as droperidol, prochlorperazine and cyclizine were less commonly prescribed. The prescribing patterns for these agents could be attributed to the availability of medications on the ward and relative ease of access. Use of ondansetron in the management of PONV is a well-established recommendation and considered first line of treatment (1).
Although metoclopramide is not one of the suggested first line therapies for the management of PONV, due to its easy access and availability in larger quantity per dispensing via the pharmaceutical benefit scheme (PBS), it is widely used by prescribers. Cyclizine, droperidol and dexamethasone are as effective drug choices for the relief of PONV. Other contributing factors such as being non-PBS, increased cost and being notas readily available may also decrease its overall use on the wards. Adopting a multi-modal approach with different agents should be considered for patients who are at moderate to high risk as antiemetic agents work independently and are similarly effective, producing a superior result (21). Consequently, the combined effects of these agents would produce a superior response when compared to each individual agent alone.
Data was collected from scanned medical records. The limitation of collecting data retrospectively meant there was a potential for incomplete data. A total 8.1% of patients did not have completed Apfel score documented by the clinical pharmacist. Omitted data affects overall results which may mislead conclusions. A relatively small sample (n=115 patients) size will also affect the limited ability to demonstrate statistical significance, leads to a higher variability, which may lead to bias. Larger studies involving patients from multiple specialities are suggested to validate the results found in this study.
The type of surgery undertaken by each patientwas not recorded. There is some evidence to suggest that patients undergoing high risk orthopaedic surgeries (neck of femur and pelvic fractures), are at greater risk of postoperative nausea and vomiting when compared to low-risk orthopaedic surgeries (joint dislocations and arthroscopic procedures) (22).
The authors recognised detailed reporting of specific surgical procedures may influence the incidence of PONV and this may inevitably affect the prescribing of antiemetics administered to the patient and thus recommended this be reviewed in future research proposals(23).
Other clinically significant risk factors such as anaesthetic technique (general anaesthesia compared to local anaesthesia) and duration of surgery were not assessed in this study.
Orthopaedic surgeries can be of variable duration resulting in differing frequencies in the occurrence of PONV. In this study, the investigators did not take into account the type of orthopaedic surgery that the patients were subject to nor was the duration of surgery reported.
PONV is a common side effect following operative management. The Apfel score includes four variables used as independent predictors for the incidence of PONV. Apfel score for orthopaedic patients are largely concentrated about two or more in their Apfel score placing them at high theoretical risk of PONV.
Overall, there was no relationship between the Apfel score and the number of antiemetic agents prescribed or administered in adult orthopaedic patients, though most patients with a score of two received one antiemetic agent. The recording of an Apfel score in orthopaedic patients did not influence the number of antiemetic agents prescribed nor the number of doses administered, thus pre-screening orthopaedic patients for Apfel scores in this study was not beneficial to predict PONV.
Head of Department: The head of the department, Mr Paul Toner, has given permission for the manuscript to be published.
Potential Conflicts of Interest Statement: None to declare
Acknowledgements: We acknowledge Stefanie N. Edwards, Emily J. Ferraro, Federica Marafioti, Thi Nguyen, Alia Rafhi and On Na Lam, RMIT pharmacy students, for their role as auditors, and The Royal Melbourne hospital pharmacy practice research committee for their contributions and assistance with the review of this report. Study data were collected and managed using the RED Cap® electronic data capture tool hosted by the Royal Melbourne Hospital Business Intelligence Unit.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
