
Case Report | DOI: https://doi.org/10.31579/2692-9759/131
Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
*Corresponding Author: Amit Mandal, Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
Citation: Amit Mandal, Oommen K George, (2024), Anomalous origin of Left Main coronary artery from right sinus presenting as non-ST elevation ACS: A case Report, Cardiology Research and Reports, 6(4); DOI:10.31579/2692-9759/131
Copyright: © 2024, Amit Mandal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 June 2024 | Accepted: 13 June 2024 | Published: 24 June 2024
Keywords: covid-19; internet; trolling; stalking; stashing; texting; bullying
Congenital anomalies of the coronary arteries are a cause of sudden cardiac death. Of the known anatomic variants, anomalous origination of a coronary artery from an opposite sinus of Valsalva (ACAOS) remains a major clinical issue and a challenging condition to treat. Congenital coronary anomalies are likely to be under-recognized, as completing an anatomic assessment in a very large portion of the population would seem unfeasible. However, we present a case report with image of a 54-year-old female presented with acute non-ST elevation ACS for which she underwent diagnostic angiography of the coronary system which revealed a common origin of both right and left main coronary artery from right sinus of Valsa.
Coronary artery anomalies (CAAs) are rare congenital defects involving the epicardial coronary arteries. The reported incidence of such anomaly ranges from 1% to 6% of the population undergoing a coronary angiography procedure and 0.3% of all autopsies. (1,2) CAAs can be classified based on coronary artery origin, course and anomalies of coronary termination(3). Herein, we present a case report with image of a 54-year-old female presented with acute non-ST elevation ACS for which she underwent diagnostic angiography of the coronary system which revealed a common origin of both right and left main coronary artery from right sinus of Valsa.
This 52-year-old lady was admitted with history of chest pain on exertion for past one month. It was retrosternal, radiating to back, associated with sweating and relieved with rest. There was worsening chest pain and for last 1-2 weeks and she started having rest pain on and off associated with sweating lasting for minutes to an hour. Last episode of pain was night before
admission which lasted for 2-3 hours and relieved slowly on its own. There was associated dyspnoea on exertion but there was no palpitations or syncope. There was no history of acute coronary syndrome or cerebrovascular accident in the past. There was history of diabetes mellitus and systemic hypertension for 15 years.
She was hemodynamically stable, and her systemic examination was unremarkable. Based on her investigations (elevated cardiac enzymes with T wave inversion in lead 1 and aVL) she was diagnosed with ACS-NSTEMI and was advised for early invasive PCI. She underwent coronary angiogram which showed anomalous origin of LM from right sinus (Fig1a-b) and double vessel coronary artery disease (Proximal LCx with tubular 60% stenosis, Distal LCx with a tubular 80% stenosis, super dominant RCA with diffuse disease, RPLB has proximal 80% stenosis in RPLB). She was advised CT coronary angiogram to assess vessel course followed by CABG with grafts to RCA and LCx with Coronary reimplantation.
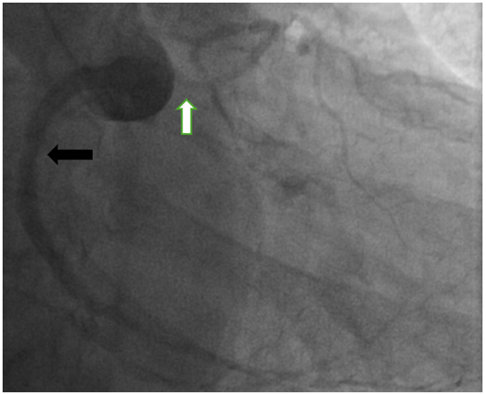
Fig1a: Aortic root angiogram showing same origin of both coronaries. (RCA: Black arrow, Left Main: white arrow)
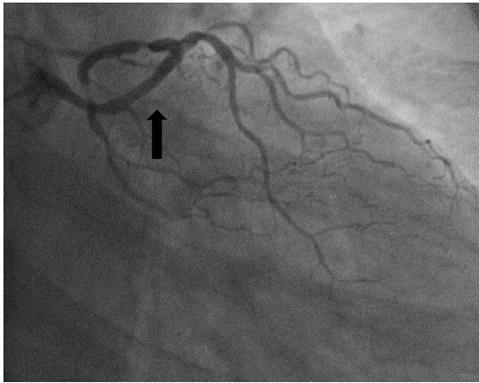
Figure 1b: LAO view to show left coronary system arising from right sinus. (black arrow)
Normally, there are 3 main epicardial coronary arteries: the right coronary artery, arising from the right sinus of Valsalva, and the left anterior descending and left circumflex coronary arteries, characterized by an initial common tract (the left main coronary artery) that emerges from the left sinus of Valsalva. (1) Coronary artery anomalies (CAAs) include several congenital conditions characterized by abnormal origin or course of any of the 3 main epicardial coronary arteries. Their clinical manifestations vary from silent bystanders to sudden cardiac death. As per previous studies, the incidence of CAA is between 1% and 6%. (1,2,4)
The clinical presentations of CAAs varies from being asymptomatic to chest pain, dyspnea, and dysrhythmia leading to SCD. (1) The underlying cause of sudden cardiac death in patients with congenital coronary abnormalities is multifactorial and has been attributed to contortion of the vessel’s slit-like, tangential origin during exercise leading to ischemia and resultant arrhythmia.
Anomalous origin of the left coronary artery from the right sinus of Valsalva may be further separated into four separate subtypes: (5)
Although the presence of a coronary artery anomaly (CAA) can be suspected in the case of a young individual with ischemia-like symptoms, however CAAs are more often incidental findings during workup for ischemic heart disease. CCTA is currently considered the gold standard, and cardiac magnetic resonance (CMR) is an alternative. (6)
Once an anomalous coronary artery is identified, it should be evaluated for hemodynamic significance, particularly in athletes, using stress testing, like exercise treadmill test, stress echocardiogram, and nuclear perfusion imaging (7) However there is no standardized protocols available for stratification of CAA-related ischemia.
In this report, we present a case with the classical angiographic finding with common origin of right and left main coronary arteries from the right sinus of Valsalva, i.e. Anomalous origin of left coronary origin from the opposite Sinus (L-ACAOS). She presented with acute coronary syndrome (NSTE-ACS) for which she was managed medically and later she was advised detail assessment of anatomy and the arterial course by CT coronary angiogram followed by CABG with grafts to RCA and LCx with Coronary reimplantation.
Treatment of an asymptomatic CAA is mostly observational and symptomatic patients almost always warrant surgical intervention. (8) Aim of surgery is to restore a dual coronary system through the reimplantation of the anomalous vessel in the ascending aorta. If the anomalous ostium is too distant from the aorta, the Takeuchi procedure can be performed by creating an intrapulmonary tunnel with a parietal flap from the pulmonary artery connecting the anomalous ostium to the aorta. (9) Coronary artery bypass graft could be a final alternative. (8) Postoperative outcome depends on left ventricular disfunction at baseline. Based on previous study published so far (n=65), operative mortality was 6.2% (10), however uniform long-term data is lacking.
The left main trunk arising from the right coronary cusp is a rare congenital anomaly associated with an increased risk of cardiac events and sudden deaths. In a patient with coronary artery disease, these anomalies may pose difficulties in their management using revascularization strategies. Further research is essential to broaden our knowledge and improve diagnostic and therapeutic modalities.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
