
Case Report | DOI: https://doi.org/10.31579/2690-4861/008
1 Lecturer/Consultant Pathologist, Department of Paraclinical Sciences, Faculty of Medical Sciences, the University of the West Indies, Trinidad.
2 Senior Lecturer/Consultant Pathologist, Department of Paraclinical Sciences, Faculty of Medical Sciences, the University of the West Indies, Trinidad.
*Corresponding Author: Srikanth Umakanthan, Lecturer/Consultant Pathologist, Department of Paraclinical Sciences, Faculty of Medical Sciences, The University of the West Indies, Trinidad.
Citation: Srikanth Umakanthan, Wayne Mohammed. (2020) Angiomatous meningioma: A rare case report. International Journal of Clinical Case Reports and Reviews. 2(2); DOI:10.31579/2690-4861/008
Copyright: © 2020 Srikanth Umakanthan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 January 2020 | Accepted: 07 February 2020 | Published: 21 February 2020
Keywords: hemanigioblastomas and hemangiopericytomas ; angiomatous ; meningiothelial cells
Meningiomas are the most common intracranial neoplasms [1]. They arise from the meningiothelial cells of the arachnoid villi and present with headache and dizziness as most common symptoms [2]. WHO has classified meningiomas into grade 1 to 3 based on cellularity, nucleocytoplasmic ratio, mitosis and necrosis.
Meningiomas are the most common intracranial neoplasms [1]. They arise from the meningiothelial cells of the arachnoid villi and present with headache and dizziness as most common symptoms [2]. WHO has classified meningiomas into grade 1 to 3 based on cellularity, nucleocytoplasmic ratio, mitosis and necrosis. Angiomatous meningioma is a rare subtype of WHO grade 1 meningioma which histological show mengiothelial cells with high vascular component in the tumor tissue. This subtype requires immunohistochemical evaluation to differentiate from hemanigioblastomas and hemangiopericytomas [3]. This case report is of a 64-year-old male diagnosed histologically as angiomatous meningioma describing his clinical, radiologic and histopathologic features.
A 64-year-male presented with history of disorientation and left sided headaches for approximately 6 weeks. His general physical examination and systemic examination was uneventful. Laboratory analysis revealed no abnormality. Radiology report showed findings of left large intra-axial frontal mass with multiple cystic densities and suggested a differential diagnosis of Glioblastoma multiforme and lymphoma. The patient underwent tumoral excision and the tissue was fixed in 10% formalin solution and sent to histopathology department. Gross examination showed five fragments of tan and haemorrhagic, firm tissue with the largest tissue measuring 4.6x3.7x2.0 cms and smallest measuring 0.9x0.8x0.5cms. On cut section it showed multiple cystic areas with spongy consistency. The tissue was subjected to routine Histological processing and then the paraffin blocks were cut with thickness of 4µ and stained with haematoxylin and eosin (H&E).
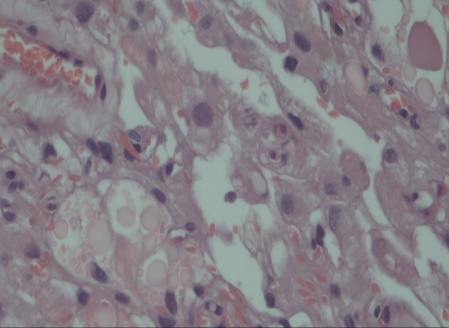
Microscopic examination showed a tumor composed of meningiothelial cells and numerous vascular spaces (Figure 1).

Meningiomas constitute 20% of all intracranial neoplasms. Almost 90% of meningiomas are benign.3 The WHO classify grade I meningiomas as the most frequent subtype. Atypical meningiomas (WHO grade II) and anaplastic meningiomas (WHO grade III) are infrequent, aggressive and have a significantly higher recurrence rate following therapy [4]. Angiomatous meningiomas are meningiomas with vascular component exceeding 50% of the tumor area. This subtype constitutes only 2.1% of all meningiomas [5]. This subtype of meningioma have similar clinical features as of benign meningiomas. The mean age of onset been 51.8 years old and occurrence higher in males. Anatomically, angiomatous meningioma is located most commonly over cerebral convexity and are dural based lesions [6]. Headache and dizziness are the most common presenting symptoms as in our case followed by temporary loss of consciousness, epilepsy, nausea and vomiting. Headaches are not a specific symptom of meningioma, hence imaging modalities are important for evaluating such patients. MRI and CT are most frequently used imaging modalities. Typical meningiomas show a characteristic dural tail and mottling indicating high vascularity of the tumor [7, 8]. Angiography can be done to exclude other vascular conditions such as aneurysm and other cerebrovascular diseases [9]. Radiologically, meningiomas show no additional characteristic features for its subtyping however, angiomatous meningiomas show perilesional edema. This is attributed to increased capillary permeability and VEGF secretion by the hyper vascular tumor [10].
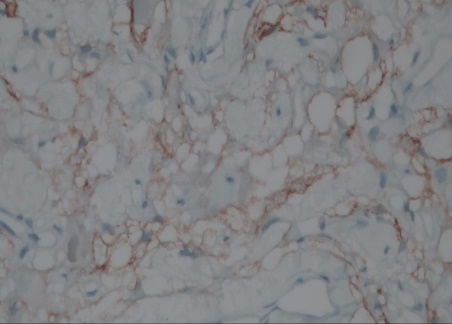
Due to the limitations in only imaging studies, subtyping of meningiomas mainly relies on its histopathologic features including immunohistochemistry and electron microscopy [11]. Meningiomas with high vascularity should be evaluated for angiomatous meningioma, hemangioblastoma and hemangiopericytomas [12]. Martin et al. classified angiomatous meningiomas based on diameter of vascular channels into two subtypes, namely macrovascular with >50% of vessels having larger than 30µm in diameter and microvascular subtype in which >50% of vessels were smaller than 30µm in diameter [13]. Microvascular subtype of angiomatous meningiomas and hemangioblastomas are difficult to differentiate hence needing IHC and EM for confirmatory diagnosis. Angiomatous meningiomas are immunoreactive to EMA, vimentin, S100 and PR. In our case EMA was positive [14]. Treatment wise total excision of the tumor remains the choice as followed in our case [2].
Angiomatous meningiomas are rare variant of WHO grade I meningiomas with few distinct clinical, radiological, histopathological and immunohistochemical features. A complete evaluation and multidisciplinary approach is required to distinguish this subtype of meningiomas from other vascular lesions in the CNS.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
