
Research article | DOI: https://doi.org/10.31579/2642-973X/074
1 Neurosurgery Service of the Maciel Hospital, Montevideo, Uruguay.
2 Department of Anatomy, Faculty of Medicine, University ofthe Republic, Montevideo, Uruguay.
*Corresponding Author: Alejandra JAUME, Neurosurgery Service of the Maciel Hospital, Montevideo, Uruguay.
Citation: Alejandra Jaume, Matilde Lissarrague, (2023), Anatomical-Imagenological Correlation of the Insula. J. Brain and Neurological Disorders. 6(7): DOI:10.31579/2642-973X/074
Copyright: © 2023, Alejandra Jaume. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 September 2023 | Accepted: 25 September 2023 | Published: 05 October 2023
Keywords: lobe of the insula; sylvian fissure; trans-sylvian approach; temporal peduncle
Introduction: The Reil insula, located deep in the Sylvian fissure, has important relationships. It is proposed to perform an anatomical-imaging correlation of the morphological and topographic anatomy of the insula. the insula of Reil, at the depth of the crack Silviana has important relationships. It is proposed to make an anatomical imaging correlation of morphological and topographical anatomy of the insula. Methods: 16 adult cerebral hemispheres were dissected formed corpses, and coronal, horizontal and sagittal sections were performed. In 4 parts white matter was dissected by Klingler method. Then correlation was performed with 20 nuclear magnetic resonance tractography and 2 images.Results: The island grooves measured on average: SIS: 53mm; IBS: 47mm; SIA 24mm. SIC: 38mm. The most posterior topography of the SIC is up to the Rolandic sulcus.
Material and Method: 16 cerebral hemispheres were dissected from formed adult cadavers, and coronal, horizontal and sagittal cuts were made. The white matter was dissected into 4 pieces using the Klingler method. Correlation was then performed with 20 nuclear magnetic resonance images and 2 tractography images.
Results: The insular grooves measured on average: SIS: 53mm; IBS: 47mm; SIA 24mm. SIC: 38mm. The most posterior sector of the SIC is topography at the height of the Rolandic sulcus.
Conclusions: Correct knowledge of the morphological and topographic anatomy of the insula is essential for the correct interpretation of imaging studies and the basis for surgical approaches to this region. the right knowledge of morphological and topographical anatomy of the island, is essential for the correct interpretation of imaging studies and the basis for surgical approaches to this region. Keywords: insula lobe, sylvianfissure, trans-sylvian approach, temporal stem.
Reil's insula was described for the first time by Johann Christian Reil in 1809. It is a cortical region that derives from the mesocortex, being a transition between the neocortex and allocortex, which has important functional implications since it is a center of connection between the limbic system and the neocortex, participating in various functions such as: perception of taste and smell, visceral control and somatoperception, integration between emotional-perceptual information and empathy, among others [1,2].
The insula is topography at the bottom of the sylvian fissure, being framed in the depth of the frontal, parietal, and temporal lobes, acquiring transcendent relationships at that level [3].
It is important to know in detail the microsurgical anatomy and its imaging correlation, given the anatomical variants, since the insula can have between 4 and 7 turns, and depending on this variation the anatomy can change, which has implications for the surgical approach to this region. where innumerable pathologies settle [4]. We know that to approach the insula, a wide opening of the Sylvian fissure is required, which is more accessible in the anterior sector at the level of the pars triangularis, due to the anatomical arrangement of the insula [5]
This is a descriptive study that included16 cerebral hemispheres, 9 right and 7 left, from formed adult cadavers, without previous intracerebral pathology. The frontoparietal and temporal opercula were resected, exposing the insula. The length of the insular sulci was recorded: anterior (SIA), superior (SIS), inferior (SII) and central (SIC). The topography of the limen insulae, the apex of the insula, and the number of turns of the anterior and posterior lobes were then recorded. Subsequently, coronal, horizontal and sagittal cuts were made to correlate with the imaging. In 4 pieces of those previously included, the white matter was dissected using the Klingler method. The use of cadaveric material was carried out after donation, through written and signed informed consent. intrinsic condition for its use for academic purposes in the Department of Anatomy. The procedures carried out were in accordance with the tenets of the 1975 Helsinki Declaration and its subsequent amendments.
Then, 20 magnetic resonance images and 2 tractography images obtained from the Clinical Radiology Department of the Hospital de Clínicas were analyzed.
Subsequently, an extensive bibliographic review on insula was carried out in Pubmed as well as in high-impact neurosurgical and anatomical journals with the following keywords (lobe of the insula, sylvian fissure, trans-sylvian approach, temporal peduncle). Works published until 2020 that were written in both English and Spanish were selected.
The insula is located deep to the frontoparietal and temporal opercula. If the lateral face of the hemisphere is observed, said cortical region is not visible on its surface, but at the moment in which the opening of the sylvian fissure occurs, the lobe of the insula begins to be observed, called the apex of the insula, when most superficial sector of this lobe (figure 1)3.
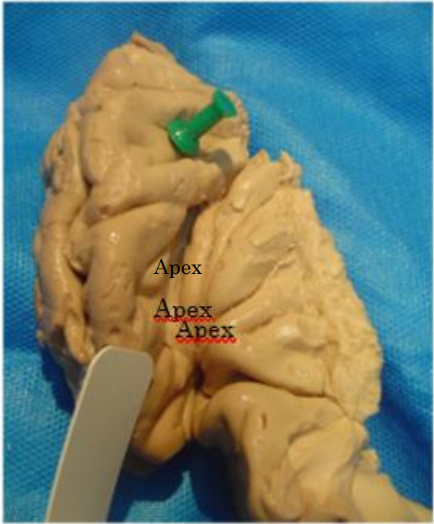
Figure 1: inferior view of the lateral aspect of the hemisphere, apex of the insula.
Usually the insula is triangular in shape with an anterior base. It is limited by three sulcus: the anterior insular sulcus (AIS), the superior insular sulcus (SIS), and the inferior insular sulcus (SII)1.
The SIA measured an average of 24mm, the SIS had an average of 52mm, and the SII measured an average of 47mm (Figure 2 and 3).
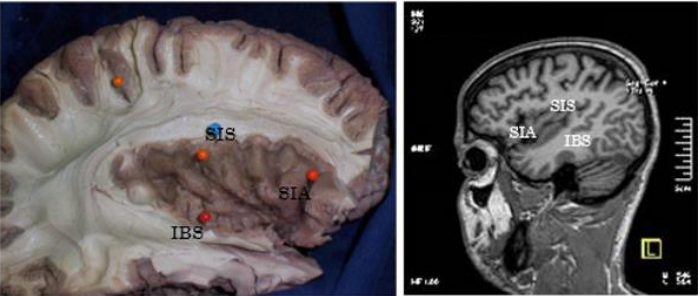
Figure 2 and 3: vision in anatomical preparation and in MRI of the insula, with its SIA, SIS, and SII.
The insula contains a central insular sulcus (CIS), which divides it into two lobes: an anterior lobe (LAI), and a posterior lobe (LPI)1.
The SIC presented an average of 38mm in length, and its posterior sector was superficially topography at the level of the central or Rolandic sulcus.
The number of island gyres is variable, with a total of between 4 and 7 gyres. In our pieces we found: between 3 and 5 turns in the LAI (3-turn mode, in 12 cases); and between 1 and 3 turns in LPI (2-turn mode, in 12 cases) (figures 4 and 5).
Figure 4 and 5: anatomical preparation and MRI showing the SIC and insular gyri.
The deep topography of the insula, surrounded and hidden by the frontoparietal and temporal opercula, makes its approach complex, being the seat of multiple vascular and tumor pathologies3. In turn, the sylvian fissure is a widely used neurosurgical corridor. For all this, we believe that it is essential to have a solid knowledge of the surgical and imaging anatomy of the insula for neurosurgeons, neurologists, neuroimaging scientists and doctors in general.
To organize the discussion we will follow the following order: 1) limit of the insula and its limiting sulci; and, 2) intrinsic structures of the insula: central sulcus, and insular gyri, highlighting that all measurements and results obtained in the present work were comparable with the published international literature.

Figure 6and 7: anatomical preparation, axial section and its imaging correlation.
The PIAS corresponds to the union of the SIA with the SIS. At this level the frontal horn of the lateral ventricle projects in depth6. The ventricular system is not usually addressed at this point, however it must be taken into account and known. In some surgical procedures, such as functional hemispherotomies, it is used to perform hemispheric deafferentation, severing the connecting fibers of the basal ganglia7.
The PIAI is the union of the SIA with the SII, and at this level the limen insulae is topography. The limen insulae is a sector of cortex that separates the insula from the anterior perforated space, or vallecula sylviana. In turn, it corresponds to the limit between the sphenoidal sector and the operculo-insular sector of the sylvian fissure. Here we must highlight two important relationships: the uncinate fasciculus, and the middle cerebral artery (MCA)8,9.
The uncinate fasciculus joins the orbitofrontal cortex with the temporal uncus, mainly with the amygdala, forming part of the limbic system (figure 8).
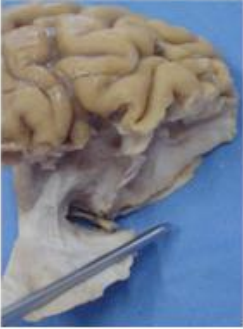
Figure 8: anatomical preparation of the uncinate fasciculus.
The MCA at this level presents its first genu or knee that marks the limit between M1 (sphenoidal sector) and M2 (opercular sector) (figures 9 and 10). The AIS has as its main relationships: the orbito-frontal cortex, the ventricular system, the basal ganglia, and the uncinate fasciculus.
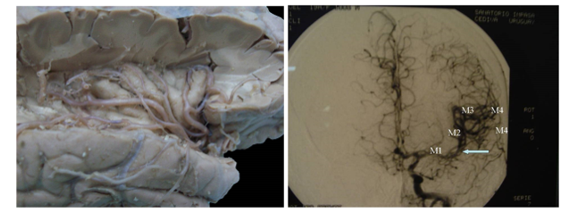
Figure 9 and 10: anatomical preparation and arteriography frontal projection pointing with an arrow to the limen insulae, and its correlation with the 4 segments of the MCA.
2. Superior insular sulcus: separates the insula from the fronto-parietal cortex, and its main relationships are: the ventricular system, the basal ganglia and the corona radiata with its projection fibers10. As mentioned previously, this sulcus is used as a reference to perform hemispheric deafferentation in hemispherotomies for the treatment of epilepsy. In these procedures, the surgeon moves towards the ventricular system following the superior sulcus, thereby severing the fibers of the corona radiata11. Thus, the relationship of this sulcus can be seen with conventional MRI images1 and with tractography11 (Figure 11 and 12).

Figure 11: anatomical preparation, sagittal section.

Figure 12: MRI tractography, descending fibers.
3. Inferior Insular Sulcus: It is the boundary between the insula and the temporal lobe. The relationship of the insula is mainly with the superior aspect of the temporal lobe, which consists of three sectors: the polar planum (PP), Heschl's gyrus (HG), and the temporal planum (PT). At the same time, we must highlight the relationship that this inferior insular sulcus has with the temporal peduncle (PedT). The temporal peduncle is a set of white matter fibers that communicate with the temporal lobe and include temporo-pontine and temporo-thalamic fibers, as well as auditory fibers, optic radiation, uncinate fasciculus, and anterior white commissure6, 7 (Figure 13 and 14).
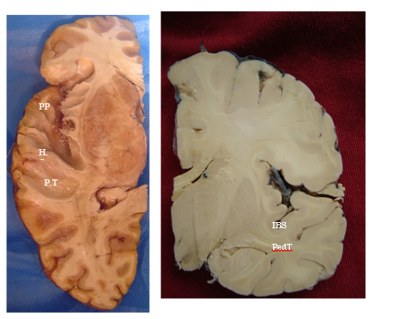
Figure 13 and 14: anatomical preparation, axial and coronal section.
At the level of the SII, two important points are also topography: the postero-superior insular point (PIPS), and the postero-inferior insular point (PIPI)1.
The PIPS is the union of the SIS and the SII, and this level corresponds to the ventricular atrium. Several authors have pointed out this point as an
area of approach to the ventricular atrium, putting it as an alternative to parietal approaches. Given the relationships of this sector, the potential sequelae of the approach through this point is injury from optic radiation.
The PIPI is located at the intersection of the SII and the HG, and at this level the optical radiation is topographic4 (Figure 15).
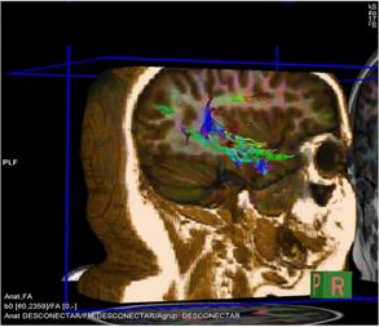
Figure 15: Tractography, sagittal section of optical radiation.
In the remaining 25%, 2 inconstant gyres were found, called accessory insular gyrus; and transverse insular gyrus. Both are located near the limen insulae.
From a functional point of view, the insula is part of the limbic system and has been associated with multiple functions such as: gustatory sensations, pleasurable sensations when faced with visual and gustatory stimuli, and cardiovascular reflexes. Usually, a function related to motor modalities is assigned to the anterior lobe of the insula, and to the posterior lobe with sensory modalities.
Based on everything analyzed, we can conclude that the insula is a complex lobe, whose topographic and functional importance makes it necessary to delve into its correct anatomy and imaging correlation, to achieve good management of the pathologies that occur in said region.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
