
Research article | DOI: https://doi.org/10.31579/2694-0248/031
1University General Hospital "Mártires Del 9 De abril". Sagua la Grande. Villa Clara Cuba.
*Corresponding Author: Lázaro Martín Martínez Estupiñan, University General Hospital
Citation: Leonardo M. Aparicio., Martínez Estupiñan LM., Lázaro M. Aparicio., Roberto M. Cuevas., Luis B. Espinosa. (2022). Analysis of Rehabilitation and Reentry to Sport in Child Athletes. J. Clinical Orthopedics and Trauma Care, 4(3); DOI:10.31579/2694-0248/031
Copyright: © 2022 Lázaro Martín Martínez Estupiñan, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 January 2022 | Accepted: 21 March 2022 | Published: 29 March 2022
Keywords: skeletal muscle; athlete child; rehabilitation; re-entry to sport
Introduction: The protection of the athlete's health is paramount, the decision to return to practice depends on each particular case, it is a process where there is a lack of consensus, and requests for priorities in the investigation.
Purpose. It is intended to analyze the results of rehabilitation and re-entry of injured child athletes.
Method: A longitudinal, prospective and quasi-experimental study was carried out. We carry out educational and medical intervention in the experimental group, which consists of the application of the system of actions for the prevention of sports injuries in the child athlete.
For the investigation, theoretical and empirical research methods were used, using two study groups. A systematic and detailed bibliographic review on the subject was carried out. In order to evaluate the rehabilitation and re-entry conditions of osteomyoarticular injuries in the child athlete.
Results: Child athletes are frequently injured around the age of 13 without significant differences with respect to the study groups, with males being more frequently injured, there are multiple actors in medical care regarding rehabilitation, and however, a large number of child athletes return to training sport.
Conclusions: The success of any academic program, including athletic training, depends on attracting and retaining quality students, rehabilitation is critical, and re-entry is part of it.
Sports coaches and teachers must create recruitment and retention strategies in child athlete preparation programs. The retention of students in athletic training is important for development and for this, three crucial factors associated with students in sports programs are suggested: firstly, student motivation, presence of adequate practice conditions and academic preparation of the teaching staff and thirdly, the presence of a support system for the care, monitoring and rehabilitation of the child athlete. [1] The decision to return to practice depends on each particular case, it is a process where there is a lack of consensus, and requests for priorities in the investigation. [2] The protection of the athlete's health is paramount; About 75% of professionals who work with children respond feeling prepared, or somewhat prepared, to provide immediate care to the injured, but additional research suggests, work is invoked to improve clinical perception in the care of sports injuries in childhood. The possibility of specialized care regarding SOMA sports injuries, within the sports school, as well as individualized monitoring, their rehabilitation and the progressive and adequate reincorporation to the sport, by the injured athlete, is identified as one of the actions of common prevention in management, this improves the health of the child athlete and responds to the difficulties with the care of this group of so vulnerable people. In some studies, it is observed when prioritizing management problems, such as difficulties with specialized care, insufficient knowledge about sports risk, and injury mechanisms; as well as the inadequacies in the
follow-up of child athletes with sports injuries and insufficient knowledge about mitigating damage in sports practice are important factors in the evolution of children with sports injuries in SOMA. The certification of coaches enables a better comprehensive care for the athlete; His knowledge about the mechanism of injury and risk factors and his knowledge and intelligence in modifying or mitigating them, allows a sporting activity, healthier and with less risk. [3] Data on behavior in the face of sports injuries and risk groups are rare, surrounded by emotional and social connotations; comparison is difficult, due to the differences in the characteristics and the way of reporting incidents; there are uncertainties about prevention, diagnosis, assistance, follow-up, rehabilitation and reintegration, [4-7] logical limitations for the health of the child athlete in this context.
There is concern among health professionals about the increase in sports injuries, their causes and how to solve them. [8-13] there are difficulties and lack of relationship between the elements or components of the health care process (promotion, prevention, health education, diagnosis, treatment, follow-up, rehabilitation and reincorporation to sport), [10, 11, and 14] the child athlete with sports injuries from SOMA. Each professional who works with child athletes can, from their specialty, make necessary and convenient contributions for their development, but greater emphasis should be placed on the care, prevention and rehabilitation of the injury and attend the athlete, in an integral way. [15]
A longitudinal, prospective and quasi-experimental study was carried out, in the period between January 2018 and December 2020. We used child athletes from two sports schools in the center of the country, for the research theoretical and empirical research methods were used, using two study groups. We carry out educational and medical intervention in the experimental group, which consists of the application of the system of actions for the prevention of sports injuries in the child athlete. In order to evaluate the rehabilitation and the conditions of re-admission of musculoskeletal injuries in the child athlete, variables such as age, sex, the place where the rehabilitation is carried out and the return or not of the injured children to the athlete are used sport. A systematic and detailed bibliographic review on the subject was carried out. In the statistical analysis carried out, tests were used, in addition to the estimation of means and proportions, the Chi square to establish the relationship between independent qualitative variables and the McNemar test for paired data. The expert evaluations were processed by the PROCESA_CE software.
We worked on a Pentium Dual Core microcomputer in a Windows XP environment, the data file was prepared in Microsoft Excel 2007 and the statistical analysis was carried out in the SPSS program (Statistical Package for the Social Sciences), version 17.0 for Windows. The results were shown in tables that were made in Microsoft Excel and SPSS itself.
The series shows in Table 1 the distribution of some general characteristics of the child athletes; among them, the ages of the child athletes injured in sports schools were very similar, with a mean close to 13 years. In the experimental group 13.01 years, before the intervention, with a standard deviation of plus minus 1.75 years, very similar results were presented in the control group, where the mean age was 12.99 years, and deviation standard plus minus 1.83 years. Regarding sex, there were no significant differences, since 63.6% of affected male children were found in the experimental group, with very close percentage figures the affected children were found in the control group, 63.5%.
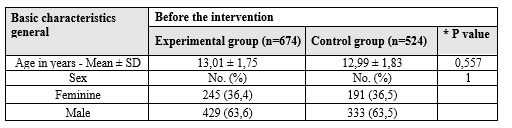
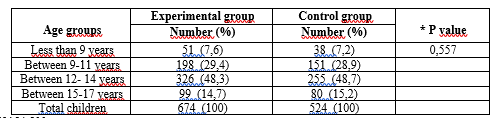
Table 2 shows the distribution of injured children according to age groups, the highest percentages are found in the 12-14 year group. It is observed how the ages of the athletes, before the intervention, are practically identical, each group presents an atypical value in 7 years and several boys or girls with 8 years in each group, so that the groups in terms of age do not they differ significantly (0.557).
Mann-Whitney U = 173154,500
Descriptive data referring to the age of the child athletes before the intervention.
Ø Mean- Experimental group = 13.01; Control group = 12.99
Ø Confidence interval for the mean at 95%
Lower limit- Experimental group = 12.88 and Control group = 12.84
Upper limit- Experimental group = 13.14 and Control group = 13.15
Ø Median- Experimental group = 13 and Control group = 13
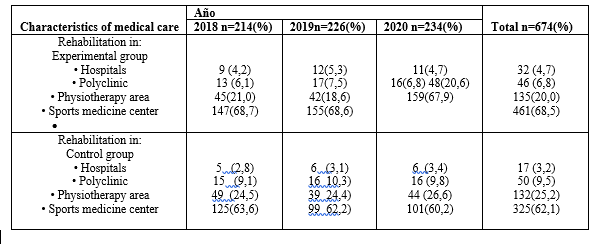
Table 3 considers the characteristics of medical care according to the place of rehabilitation (Hospital, polyclinics, physiotherapy areas or sports medicine center.
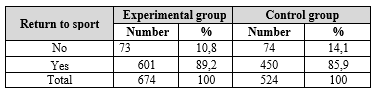
After the injury, in the experimental group 89.2% of the injured athletes returned to sports activity, very similar to what was seen in the control group (89.7%), as seen in Table 4, There are also no significant differences between the groups in this study variable, it is possible to appreciate the multiple actors who were in charge of the rehabilitation process and re-entry to sports activity.
X2 = 0.086
p = 0.778
Source: Observation Guide for Child Athletes. Prevention consultation.
* P values were calculated using the Chi-square test or Fisher's exact test.
Regarding the characterization of care in injuries, their diagnosis, treatment, follow-up and rehabilitation, Aitken SA et al. [16] report that the diagnosis, in 80%, is made clinically, with important use of diagnostic imaging, [17] and vital role for the medical team. [18] The decision to return to practice depends on each particular case, it is a process where there is a lack of consensus, [19] and requests for priorities in the investigation. [20, 21] There are statistics where authors report that between 85% and 87% return to sport, [22] while others report losses close to 8% [23] Increasing participation in physical activities significantly improves health, but there are no guidelines to help professionals decide when it is safe to return to sport for a patient after an injury, much less in child athletes. Treatment must be individualized. The authors consider that the characterization of sports injuries, from the clinical and epidemiological point of view, makes it possible to recognize the health conditions of the child who participates in sports activities, an aspect that has not been previously carried out with these variables in sports initiation schools, from the country. Regulating rehabilitation guidelines for child athletes within sports schools and agreeing criteria for re-entry into sports for the injured child are elementary issues within a sports injury prevention system for the muculoskeletal system in child athletes. Being able to determine the necessary multidisciplinary strategies and actions to be carried out by professionals who work with child athletes, and to reduce the number of injuries and their intensity through preventive work, is hard and constant work. The problem posed by injuries is notable in the training-competition process, since it implies their modification or interruption. Any injury incidence alters training plans and is an important factor in training control. The most common intervention within the sports field focuses on the recovery of injuries to return to the previous level of sports performance, and this is a costly process from an economic and sports point of view. However, in recent times the interests have been oriented towards the development of strategies and multidisciplinary intervention proposals related to the prevention and rehabilitation of sports injuries and the athlete. We must consider prevention as the most important practice and one of the priority objectives in the world of sport and especially in the area of health. There are statistics where authors report that between 85% and 87% return to sport, while others report losses close to 8%. [10, 11] The paths to an effective rehabilitation should begin with effective social support of all factors, an adequate medical diagnosis, acceptance of the injury by the child athlete and his family, avoiding the feeling of guilt, working on the control of expectations and anxiety, maintaining an adequate evaluation and control of pain, maintaining interdisciplinary work so that exercises are assumed responsibly, with short-term goals. Work on a daily basis so as not to lose the activity of the child athlete with the group, increase motivation and self-confidence through rehabilitation, use relaxation techniques and practice in imagination, evacuating fear. The decisive criteria to achieve an adequate return must be treated with caution, taking into account the athlete and the situation at the time. The non-existence of a consensual opinion regarding the time necessary for a safe return to sport means that in most cases there are no specific criteria for an injured athlete to return to the group. A rehabilitation program involving intense, sub-intense, and delayed stages, and return to sports must surely be designed to improve motor skills, performance, and sport-specific skills.
Organized rehabilitation must have 4 principles:
- The type of injury.
-The preparation
- Accurate and complete diagnosis
- Treatment plan and reentry to sport.
There are guidelines for rehabilitation, including the objective of the sports injury rehabilitation process to minimize tissue damage and allow a safe return to activity, it is based on the science of tissue healing, on the knowledge of the joint biomechanics, in the physiology of muscular strength and endurance, and in the neurophysiological basis of motor and technical retraining. Successful programs are based on an awareness of these commitments, which, when performed correctly, allow progressive activity of the joints and muscles. For Garrido Chamorro RP and collaborators, in the Emergency Service of the General University Hospital of Alicante, [24] more than 22% of young people between 8 and 17 years old suffer a sports injury; however, Gandia J, at the University of Murcia, found that the incidence of injuries was 9.4% per year. [25] Street EJ and Jacobsen KH, [26] state in their study of 25 countries, that the rates are highly variable, according to sport and age, Malisoux et al. [27] report rates lower than 5 per 100 children in 1000 hours, other authors obtain figures between 10.5 and 22.4 per 1000 hours of sports activity. [28] The authors consider that rehabilitation is the key to full recovery after injury, its fundamental objective is the recovery of maximum function as soon as possible, the principle of restoring full function is to regain range of motion, strength and coordination. For this, the elongation and resistance strengthening exercises should be started with light resistance and higher repetitions. As strength recovers, add coordination and functional activities, sports or related activities, and incorporate more advanced strengthening and range-of-motion exercises. An excessively aggressive therapy can cause more harm than good, examples of which are: tendinitis, tendon rupture, fracture or dehiscence of the surgical wound with the consequent failure of medical or surgical treatment. Cryotherapy reduces inflammation, but should be avoided in areas of compromised circulation and in patients sensitive to cold, it is a very valuable adjunct to treatment, the same happens with thermotherapy which is used to increase blood flow in the injured area, it promotes muscle consolidation and relaxation, but should not be used in acute and sub-acute injuries due to the risk of increased bleeding or swelling. Within the recommendations for rehabilitation, the stretching should be performed slowly and maintained without rebounding, regarding the range of active movement the patient can perform the joint exercise, muscle tonicity and proprioception, but the range of passive movement the therapist can perform the external force to stretch or move the joint. Regarding the elongation, it should be done with a slow and controlled speed through safe parameters of the range of movement of the child athlete. Other procedures such as ultrasound can be used in chronic inflammations and to increase the mobility of the joints, it should not be on the physeal areas. Also electric current (electrotherapy) can be used to reduce pain and edema, gain strength and prevent atrophy, but should not be used on damaged skin. The return to sport should be viewed as a continuous process with three elements, return to participation, return to sport, and return to peak performance. The return to sport goes hand in hand with recovery and rehabilitation, it is not a decision taken in isolation at the end of recovery and the rehabilitation process must be a collegiate decision. Four key issues are identified in the return to sport, firstly defining the relationship to return to practice and the sports context of participation, secondly the models to help understand and guide the return process, the test by putting return and the decision to get fit and finally the priorities for future research. Most of the available research focuses on the risk for re-injury after returning to sport. The future research should focus on developing standardized advances in defining, measuring, and reporting return to sport, and identifying valuable predictors for returning to sport. Currently, there is no consensus within the literature on when to return to sport given the lack of standardization and objective criteria on the subject. Recommendations are often vague, stating that athletes can return once strength recovers, and functional skills (jumping, running, and turning) can be performed without complaints of pain or symptoms. The clinical examination should not reveal signs of a remaining lesion. The Department of Family Medicine, Center for Epidemiological Studies at Mc Gill University, in Canada, examined specific criteria that medical experts use for return to activity in children with SOMA lesions; regarding the importance of specific signs for returning to activity, all professionals had similar responses: absence of pain. [29] The success of any academic program, including athletic training, depends on attracting and retaining quality students, so knowing the number of child athletes who train and persist, those who leave and do not return, it is important to note that so far the vast majority of the Sports injuries have been addressed from the point of view of treatment and rehabilitation, not internalizing preventive aspects, which has not only increased the number of injuries, but also increased their severity. To get back into sports, it all depends on the specific injury suffered. There are processes that can be done to maintain shape while recovering from the injury without aggravating it, these activities are known as combination or mixed training and include stationary cycling, hydrotherapy, and rowing machines. The rehab program will also help you stay in shape while you recover. It can be part of a treatment program and can include exercises, manipulations performed by a physical therapist, and technological devices, such as ultrasounds. Safety in sports practice is vital for sports life, fundamentally in the education of sports talent, it is recommended that you use the protective equipment that your sport carries; to avoid re-injury, you must ensure that your child athlete warms up properly before training sessions and games. You should go calmly, gradually increasing the intensity of your workouts until you reach the level you had before you injured yourself. Knowing the limits of child athletes leads to a better understanding of their abilities. Pain is the body's way of saying something is wrong. It is necessary to learn from experience and do things that can help prevent injury to the child athlete. The intervention regarding the prevention of injuries is not merely an educational intervention, it is more than that, it implies the use of epidemiology and the clinic in the solution of a scientific problem that affects the development of the sports life of our child athletes. It consists fundamentally in raising the knowledge of managers, sports coach’s teachers, child athletes and health personnel who work in the care of this specific group of the population.
Conflict of interests
The authors of this article declare that they have no conflict of interest whatsoever with the objectives of the research.
Declaration of the personal contribution of each author to the research.
The authors of this article participated in the diagnosis, treatment, study design, and writing of the first version, as well as the final version of the manuscript in equal parts.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
