
Review Article | DOI: https://doi.org/10.31579/2641-0419/370
Riojan Health Service, Emergency Service 061, Piqueras 98, 26006, Logroño, La Rioja, Spain.
*Corresponding Author: Alejandro Jesús Bermejo Valdés, Riojan Health Service, Emergency Service 061, Piqueras 98, 26006, Logroño, La Rioja, Spain.
Citation: Bermejo Valdés AJ, (2024), Analysing Wilson’s and Goldberger’s Central Terminals: Theoretical Redesign of a Novel Central Terminal for Precordial Leads, J Clinical Cardiology and Cardiovascular Interventions, 7(4); DOI: 10.31579/2641-0419/370
Copyright: © 2024, Alejandro Jesús Bermejo Valdés. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 April 2024 | Accepted: 01 May 2024 | Published: 27 May 2024
Keywords: electrocardiography; einthoven’s triangle; wilson’s central terminal
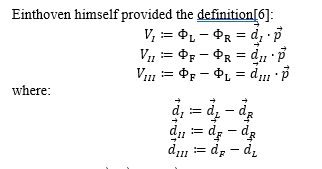
This study delves into the foundational aspects of electrocardiographic (ECG) lead systems, specifically focusing on Einthoven’s Triangle and Wilson’s Central Terminal. We introduce the innovative concept of a Precordial Central Terminal, a strategic arrangement of thoracic electrodes that establishes two Einthoven’s triangles within the horizontal plane, in accordance with physical-mathematical principles. Furthermore, we meticulously scrutinize Goldberger’s contributions to the field of ECG, particularly augmented leads, which shed light on the development of our theory. Additionally, we propose the implementation of a novel standardized electrocardiograph, characterized by its use of exclusively “precordial” electrodes, yet capable of providing a comprehensive three-dimensional perspective of cardiac electrical activity. By amalgamating theoretical underpinnings with empirical experimentation, our study lays the groundwork for future investigations, including the experimental validation of our innovative Precordial Terminal. This validation holds the promise of yielding substantial advancements in the realm of clinical electrocardiography.
The generation of electrocardiographic (ECG) records is grounded in models that capture the complexity of cardiac electrical signals. An indispensable cornerstone of this field is the iconic Einthoven’s Triangle, an equilateral triangle establishing the foundation for cardinal and augmented leads on the ECG. It also serves as the basis for defining Wilson’s Central Terminal (WCT)[1]. Yet, despite its prominence in clinical practice, profound questions persist concerning the underlying theory and precise interpretation of both leads and the WCT.
A meticulous examination is carried out on Goldberger’s contribution to ECG theory, particularly in the context of augmented leads.
At the heart of our analysis lies the WCT, a concept that has intrigued researchers for decades. Our discussion revolves around the historical interpretations of this terminal and its connection to the cardinal and augmented leads. Through meticulous exploration, we reveal the evolution of the interpretation of WCT, along with the persisting limitations and challenges in its precise measurement.
This article presents a thorough examination of the fundamental principles of cardinal leads within the framework of Einthoven’s Triangle. We explore the concept of the bipolar lead vector, which defines the electrical potential difference between two points on the conductor surface. By understanding these vectors, we clarify the mathematical and geometric relationships that form the basis of the classic cardinal leads: DI, DII, and DIII. We explore the discrepancies between traditional theories and modern observations, highlighting the need for a solid integration of theoretical concepts and experimental practices. In this context, we propose a new theory that unifies these aspects in a more coherent approach.
II.1. Reference electrode
The standard electrocardiogram (ECG) employs 12 leads and includes a reference electrode positioned on the Right Leg (RL), resulting in a total of 9 electrodes[2] responsible for its generation:
The three limb electrodes give rise to the three vertices of Einthoven’s Triangle[2]. These vertices are separated from each other by an angle of 120º, considering the lines originating from the centroid.
Based on this, we can define:

where  represents the cardiac electrical potential measured by an
represents the cardiac electrical potential measured by an  electrode on the limb or, equivalently, at a vertex point of Einthoven’s Triangle[2,5,6].
electrode on the limb or, equivalently, at a vertex point of Einthoven’s Triangle[2,5,6].
Eq.1 signifies that the values of various potentials are inherently linked to the potential of the right leg,  . Assuming that
. Assuming that  is measured concerning a neutral potential (e.g., earth ground)[2], any potential difference measurement should inherently refer to
is measured concerning a neutral potential (e.g., earth ground)[2], any potential difference measurement should inherently refer to  . For instance:
. For instance:  .
.
Similarly, the augmented leads introduced by Goldberger are calculated as the difference between one of the limb potentials ( ,
,  , and
, and  ) and the average of the remaining two[5]. For instance:
) and the average of the remaining two[5]. For instance:

This action amplifies the signal by 50 % if the reference were established using the WCT (non-augmented leads: VR, VL, and VF):

where  is the potential of the WCT, which historically has been defined as[2,5,6]:
is the potential of the WCT, which historically has been defined as[2,5,6]:

II.2. Wilson’s Central Terminal
As evident in Eq.2, the calculation of WCT involves taking the average of potentials recorded by the cardinal leads of Einthoven’s Triangle. However, an additional aspect needs consideration: a high-value resistance (≥ 5 kΩ) is added to those connected to each of the electrodes. These three corresponding electrodes are positioned to converge at a common point, where the theoretical placement of the WTC is posited: at the centroid of Einthoven’s Triangle[2,6] (Figure.1).
Clearly represented in Eq.2, WCT is calculated as the average of the potentials registered by the cardinal leads of the Einthoven’s Triangle; but we must add one aspect: from those that are connected to each of the electrodes a resistance of high value (≥ 5 kΩ). The three corresponding electrodes are made to coincide at a common point, which is where the theoretical location of the WTC is assumed: the centroid of the Einthoven’s Triangle[2,6] (Figure.1).

Figure 1: Theoretical placement of Wilson’s Central Terminal within Einthoven’s Triangle. This position is assumed to be at the centroid of the triangle. The vertices are positioned at intervals of 120º from one another, with consideration given to the lines originating from the origin at the centroid.
The WCT serves as a neutral reference point for the precordial leads within the 12-lead ECG. As demonstrated in Eq.2, its influence is rooted in the three cardinal electrodes, implying that its value hinges on the positioning of the limb electrodes. However, recent observations have unveiled fluctuations in the WCT throughout the cardiac cycle, resembling behaviour akin to a lead[2,7,8]. There has even been suggesting its potential existence beyond the geometric plane defined by the cardinal leads[2], in essence, beyond the plane encompassing Einthoven’s Triangle.
Despite a few investigations[2,7,8], research on the WCT has been relatively limited in recent years, perhaps attributed to the arduous methods necessitated by experimental studies attempting its measurement, such as the immersion of study subjects in water after their confinement within a metallic structure[7].
In the 1950s, Ernest Frank[9], in his influential work “General theory of heat-vector projection”, was the pioneer in raising concerns about fluctuations in the WCT during the cardiac cycle, an observation that has since been validated. This validation is exemplified by recent measurements, such as the quantification of the WCT amplitude relative to the DII amplitude, yielding a value of 51.2 % (with a reported standard deviation of 27.4 %) and even reaching peaks exceeding 100 %[8].
The comprehensive investigation conducted by Gargiulo et al. in 2016[8] substantiates considering the WCT as an additional reference. However, the persistence of a theoretical discrepancy between Wilson’s original work and present-day observations raises questions.
As of today, ongoing experiments continue to probe the significance of the WCT and its spatial location. Nonetheless, it remains imperative to synthesize the historical theoretical groundwork with the findings of contemporary empirical studies.
The generation of an ECG recording is predicated on a model wherein the limb (or cardinal) leads constitute Einthoven’s Triangle. Within this triangle’s centroid, a dipole moment vector is postulated to be anchored at its origin, functioning as an analogy of cardiac electrical activity. Throughout the cardiac cycle, it rotates as a temporal function[2]. We establish the concept of an arbitrary electric dipole consistent with theoretical principles[6], represented as  , relative to the canonical basis
, relative to the canonical basis  of the Cartesian Coordinate System. This dipole is affixed at the origin and is defined as follows:
of the Cartesian Coordinate System. This dipole is affixed at the origin and is defined as follows:

where  ,
,  , and
, and  denote the components of
denote the components of  along the
along the  ,
,  , and
, and  axes, respectively.
axes, respectively.
Consider an arbitrary point  located on the surface of any conductor. We establish the potential
located on the surface of any conductor. We establish the potential  due to the presence of the dipole
due to the presence of the dipole  at point
at point  as follows:
as follows:
where  is a vector whose components,
is a vector whose components,  ,
,  , and
, and  , correspond to the values of the measurement
, correspond to the values of the measurement  under the assumption that the electric dipole is represented by the basis vectors themselves. The operation
under the assumption that the electric dipole is represented by the basis vectors themselves. The operation  denotes the dot product. This vector,
denotes the dot product. This vector,  , is identified as the lead vector. In this context, the reference point for potential measurements at point
, is identified as the lead vector. In this context, the reference point for potential measurements at point  is regarded as arbitrary[6].
is regarded as arbitrary[6].
When we take into account an infinite number of points,  , distributed across the surface of the conductor and assume a constant dipole, we can express:
, distributed across the surface of the conductor and assume a constant dipole, we can express:
where  denotes the electric potential difference between points
denotes the electric potential difference between points  and
and  . We refer to these points as “leads”, and they are the locations on the conductor’s surface where the electrodes are positioned[6] (Figure.2).
. We refer to these points as “leads”, and they are the locations on the conductor’s surface where the electrodes are positioned[6] (Figure.2).

Figure 2: Cartesian coordinates of the electric dipole vector and the positions of points (leads) designated for measuring electric potential on the surface of a conductor (depicted as yellow tissue).
where  , and this difference is referred to as the “bipolar lead vector” since it involves two measurement points (leads).
, and this difference is referred to as the “bipolar lead vector” since it involves two measurement points (leads).
Within Einthoven’s Triangle, the lead vectors  ,
,  and
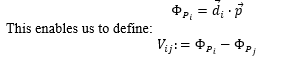
and  are characterized as vectors originating from the centroid of the triangle and extending to the vertices R, L, and F (signifying the right arm, left arm, and left leg electrodes, respectively) (Fig.3). Consequently, the potentials at the vertices can be established for an arbitrary constant dipole
are characterized as vectors originating from the centroid of the triangle and extending to the vertices R, L, and F (signifying the right arm, left arm, and left leg electrodes, respectively) (Fig.3). Consequently, the potentials at the vertices can be established for an arbitrary constant dipole  as follows:
as follows:

Figure 3. Spatial arrangement of the vectors  ,
,  and
and  within Einthoven’s Triangle.
within Einthoven’s Triangle.
These vectors ( ,
,  and
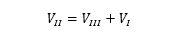
and  ) originate and terminate at the vertices of Einthoven’s Triangle. They are the vectors recognized in clinical practice, as they define the orientations of the axes DI, DII, and DIII within the Bailey Hexaxial System [2,5,6].
) originate and terminate at the vertices of Einthoven’s Triangle. They are the vectors recognized in clinical practice, as they define the orientations of the axes DI, DII, and DIII within the Bailey Hexaxial System [2,5,6].
The notations DI, DII, and DIII essentially represent the “standard leads of the members”. In other words, they denote the notations employed for the scalar magnitudes of potential differences  ,
,  and
and  .
.
The magnitudes of the potential differences  ,
,  and
and  in the directions
in the directions  ,
,  and
and  , respectively, they are not independent; rather, they adhere to Kirchhoff’s Law[6]:
, respectively, they are not independent; rather, they adhere to Kirchhoff’s Law[6]:
To accurately define the spatial orientation of Einthoven’s Triangle, it is imperative to adopt a coordinate system that eliminates any ambiguity or confusion in the interpretation of magnitudes involved in our analysis.
For the purposes of this paper, we will establish a reference coordinate system in which the positive directions of the  ,
,  , and
, and  axes correspond to the front, right (from the observer’s perspective), and top directions, respectively. With this setup, assuming α represents the angle between the vector
axes correspond to the front, right (from the observer’s perspective), and top directions, respectively. With this setup, assuming α represents the angle between the vector  , fixed at the centroid of Einthoven’s Triangle, and the horizontal axis, we can express this relationship as follows [6]:
, fixed at the centroid of Einthoven’s Triangle, and the horizontal axis, we can express this relationship as follows [6]:
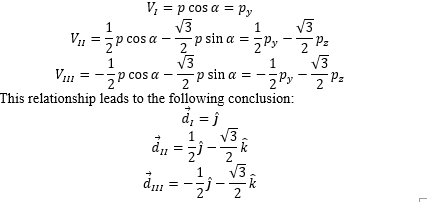
It's noteworthy that these three vector equations involve the component  . In other words, the plane’s description disregards the
. In other words, the plane’s description disregards the  -coordinate of our chosen coordinate system (Figure.4).
-coordinate of our chosen coordinate system (Figure.4).
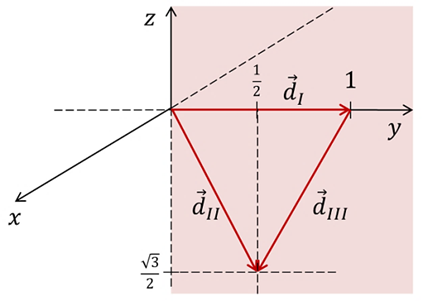
Figure 4: Spatial arrangement of the vectors  ,
,  and
and  within Einthoven’s Triangle.
within Einthoven’s Triangle.
Based on the accumulated theory, let’s delve into the workings “inside” the definition of the WCT[2,5,6]. According to Eq.2:

The sum  invariably results in the additive identity of vector summation due to the additive inverse nature of vector operations. Additionally, the outcome of Eq.3 yields a scalar value of zero, stemming from the dot product of a vector
invariably results in the additive identity of vector summation due to the additive inverse nature of vector operations. Additionally, the outcome of Eq.3 yields a scalar value of zero, stemming from the dot product of a vector  , where its components
, where its components  ,
, and
and  are all null.
are all null.
If Eq.3 were valid, the introduction of  resistors to establish a neutral reference would not have been essential; indeed, the reference potential of WCT would have been precisely zero.
resistors to establish a neutral reference would not have been essential; indeed, the reference potential of WCT would have been precisely zero.
Conversely, in augmented leads, a similar strategy with resistors is adopted. Here, two resistances of  are integrated from the leads designated as reference points. These leads are connected and converge at a common point known as Goldberger’s Central Terminal (GCT). Intriguingly, the orientation of the augmented lead vectors, namely aVR, aVL, and aVF, corresponds to that of the vectors
are integrated from the leads designated as reference points. These leads are connected and converge at a common point known as Goldberger’s Central Terminal (GCT). Intriguingly, the orientation of the augmented lead vectors, namely aVR, aVL, and aVF, corresponds to that of the vectors  ,
,  and
and  , respectively. This alignment signifies a clear and distinctive functional relationship between Einthoven’s and Goldberger’s leads:
, respectively. This alignment signifies a clear and distinctive functional relationship between Einthoven’s and Goldberger’s leads:

As per Eq.4, it becomes necessary to suggest the positioning of three GCT at the midpoint of each side of Einthoven’s Triangle. Consequently, the orientation of augmented leads aligns with the medians of Einthoven’s Triangle, consistent with the respective vertices they are denoted by.
Interestingly, the parallels between the behaviour of GCT and WCT appear to diverge. The author’s literature review did not yield significant data that reproduces the phenomena observed with WCT.
Building on Goldberger’s concept of enhancing the signal from leads VR, VL, and VF by altering WCT to GCT, a notion arises to extract the potential from the specific electrode in question.
Given the intrinsic relationship between augmented leads and the cardinal leads, we can infer the subsequent equations[5]:
While Goldberger’s concept was indeed ingenious, it’s noteworthy that the precordial leads continue to reference the WCT. Notably, no inherent issue arises from this arrangement, as none of the precordial leads are encompassed within the WCT framework.
The rationale behind augmenting the signal was particularly pertinent during an era when ECG traces were characterized by their high thickness and low amplitude [10].
It is possible to formulate a Central Terminal for the precordial leads using reasoning akin to Goldberger’s approach. Goldberger extracted the electrode potentials from an existing Central Terminal (Wilson’s), while keeping the remaining two as references. However, in the case of precordial leads, they refer to a Central Terminal that doesn’t inherently include the precordial electrodes.
It suggests the possibility of devising a Central Terminal solely using precordial leads that could function as a reference point. If such a formulation were attainable, the terminal’s fluctuations might parallel the behaviour observed in GCT fluctuations within augmented leads, which demonstrate consistent comportment.
A study conducted by Medias et al.[10] presents intriguing insights. They suggested a shift from the 12-lead ECG to a 9-lead ECG comprising the 3 non-augmented leads (VR, VL, VF) and the 6 precordial leads. They proposed using VR, VL, and VF leads by placing the initial three precordial electrodes on the right arm, left arm, and left leg, respectively[10]. This generated three signals that, while slightly reduced in amplitude compared to their magnified counterparts, maintained sufficient visual quality for clinical diagnosis.
Moreover, an alternate 9-lead ECG model has been employed, maintaining the concept of a reliable reference. For example, a model retained the limb leads (both Goldberger’s and Einthoven’s) but excluded V2, V4, and V5. Although this model still used 12 electrodes, it incorporated 6 distinct reference electrodes positioned on the right leg[11].
After thoroughly examining prior research and aligning it with the theoretical framework[2-10], we were initially inclined to propose the following definition:
This concept aimed to establish a precordial lead in relation to the average of the other five leads, distributing electrodes equally around the thorax. However, upon more in-depth analysis, we realized that this formulation would not harmonize with the vector theory we have developed, as the lead vectors would lack a coherent arrangement.
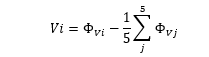
Upon further scrutiny, and consistent with the current theory, we arrive at the following proposition as a potential solution to the issue of precordial reference electrodes:

In this context,  indicates that the other two leads being considered must be separated by an angle of 120º.
indicates that the other two leads being considered must be separated by an angle of 120º.
To achieve the desired spatial distribution of the 6 precordial electrodes, it is necessary to position the electrodes around the thoracic circumference at intervals of 60º, as 360º/6 = 60º (Figure.5).
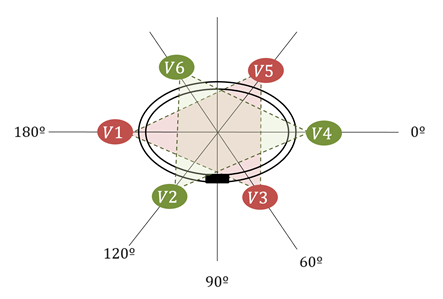
Figure 5: Cross-sectional view of the thorax depicting the arrangement of precordial electrodes in the revised configuration for calculating a precordial Central Terminal. The leads under consideration are positioned at intervals of 120º from one another and are separated by 120º angles. Two groups of three leads each form two equilateral triangles, analogous to Einthoven’s Triangle. The sternum is indicated by a black rectangle.
As illustrated in Fig.5, we can create a configuration resembling two “Einthoven’s Triangles” arranged horizontally, forming what we can refer to as a “six pointed star”. Drawing from the earlier vector analysis, the distinct Central Terminals will be situated at the midpoint of the opposing side of each precordial lead, with both triangles sharing the same centroids. Furthermore, the arrangement of the bipolar lead vectors reproduces that of Einthoven’s Triangle with a frontal orientation. This signifies that we can establish lead vectors within our horizontal triangles much like we described for Einthoven’s Triangle.
By placing the origin of our coordinate system at the intersection point of all the medians from both triangles, we acquire a coordinate framework
in which we can accommodate the frontal Einthoven’s Triangle and the two Einthoven’s Triangles.
In light of this, we can conceive a “novel electrocardiograph” that is entirely standardized in terms of its Central Terminals and leads, exclusively utilizing “precordial” electrodes. Consequently, “non-augmented” frontal plane leads could be derived from the same precordial leads, as proposed by Medias et al.[10]. This approach, considering the insights presented by Cho et al.[11], suggests that even the reference to the right leg might not be dispensable.
Traditional electrocardiographs are structured with three main components: Einthoven’s leads, Goldberger’s leads, and precordial leads. The first two exhibit clear functional relationships, while the third, seemingly isolated, holds inherent potential to generate three frontal plane leads of adequate quality. In the contemporary context, it appears essential to standardize conventional electrocardiography, despite the historical concepts tailored to our clinical convenience.
We have conducted an exhaustive review of the theoretical and conceptual foundations supporting ECG leads and central leads in the context of Einthoven’s Triangle. We investigated the evolution of the Wilson Central Terminal and its need for a more robust physical-mathematical definition. We proposed an innovative Central Terminal for the precordial leads, based on the spatial arrangement of the electrodes around the thorax and related to the formulation of two Einthoven’s triangles on the horizontal plane, which could standardize the non-augmented frontal plane leads in conventional electrocardiography.
Therefore, we emphasize the importance of combining theoretical foundations with practical experimentation and suggest experimentally validating the new Central Terminal proposal and exploring its applicability in clinical diagnosis to improve current practices.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
