
Review Article | DOI: https://doi.org/10.31579/2693-7247/070
Department of Pharmacy, Negelle Health Science College, Guji, Ethiopia.
*Corresponding Author: Gudisa Bereda, Department of Pharmacy, Negelle Health Science College, Guji, Ethiopia
Citation: Gudisa Bereda, (2022) Anaemia and Antianaemic Medications. J. Pharmaceutics and Pharmacology Research. 5(4); DOI: 10.31579/2693-7247/070
Copyright: © 2022, Gudisa Bereda, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 February 2022 | Accepted: 20 February 2022 | Published: 08 April 2022
Keywords: anaemia; antianaemic; medications.
Anemia is a group of diseases described by decrease in hemoglobin or red blood cells, resulting in decreased oxygen-carrying capacity of blood. Iron deficiency is the most frequent nutritional deficiency, and the most routine cause of nutrition related anemia. Vitamin B12 deficiency is the sequence of impaired absorption (pernicious anemia are imperfect production of intrinsic factor compulsory for absorption of vitamin B 12). Without folic acid, deoxyribonucleic duplication and cell separation cannot continue. Colchicine, para-aminosalicylic acid and heavy alcohol intake for lengthy than 2 weeks perhaps generates malabsorption of vitamin B12. Iron combines with porphyrin and globin chains to figure hemoglobin, which is underpinning for oxygen release from the lungs to different tissues. Folic acid should not be given alone in patients with pernicioius anemia without knowing whether they also have a Vitamin B12 deficiency.
Anemia is a group of diseases defined by decreases in Hb or RBCs, resulting in decreased oxygen-carrying capacity of blood [1]. WHO defines anemia as Hgb < 13 xss=removed females=12.3>
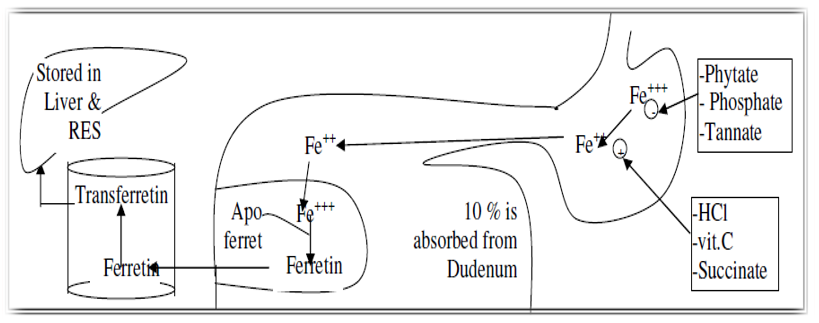
Iron deficiency:Fe deficiency is the most ubiquitous nutritional deficiency, and the most ubiquitous cause of nutrition related anemia [5]. Fe serves as indispensable to the work of hemoglobin, myoglobin (the oxygen-storing molecule of muscle), and a diversity of iron-bearing enzymes [6]. Daily requirement (demand) of Fe in male is 10mg and female 15 mg, iron seek is accelerates in cultivating children, pregnant and lactating women owing to their body increased demand for iron [7]. Dietary origins of Fe enclose foods specifically high in Fe involve liver, egg yolk, brewer's yeast, and wheat germ. Other: muscle meats, fish, fowl, cereal grains, beans, and green leafy vegetables [8].
Absorption: Fe is absorbed in duodenum and proximal jejunum [9]. A normal individual without Fe deficiency absorbs 5-10 % of daily inputs. Fe in the ferrous form (Fe++) is absorbed further preferably than iron in the ferric form Fe+++) [10].
Elimination: Little amount are excreted in stool by shed of intestinal mucosal cells and vestige amount are excreted in bile, urine and sweat with total daily excretion not greater than 1mg/day [11].
Cause of Fe deficiency: Blood destruction (deep or superficial): Peptic ulcer diseases, diverticulosis, colon cancer, chronic nose bleeding, menorrhagia, occult GI bleeding, and worm infestation [12]. Fe absorption also decreased owing to achlorhydria, atrophic gastritis, and celiac disease [13]. Foods and medicines: phytate, calcium, soy protein, polyphenols decrease iron absorption [14]. Infrequent causes: intravascular hemolysis, pulmonary hemosiderosis, EPO, gastric bypasses [15]. Decreased input (rare) [16]
EPO production inadequate for the degree of anemia observed or erythroid marrow responds inadequately to stimulation [17]
Causes: Inflammation, infection, tissue detriment, cancer, chronic kidney disease [18]

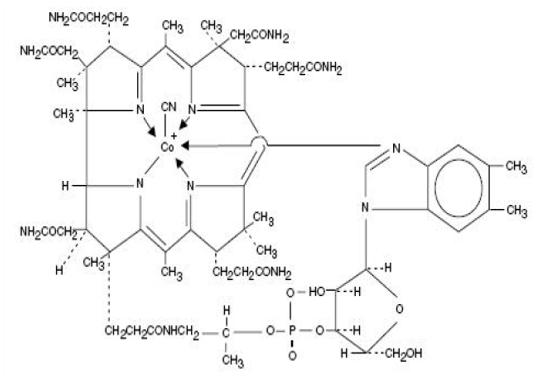
Vit B12 is made up of a porphyrin-like ring with a central cobalt atom connected to a nucleotide [19]. Cyanocobalamin is a synthetic figure of vit B12 with equivalent vit B12 activity [20]. The chemical name is 5, 6-dimethyl-benzimidazolyl cyanocobamide. The cobalt content is 4.35%. The molecular formula is C63H88CoN14O14P, which comparable to a molecular weight of 1355.38 [21] and the following structural formula:
Vit B12 is indispensable for growth, cell duplication, hematopoiesis, and nucleoprotein and myelin production. Cells described by hasty separation (e.g., epithelial cells, bone marrow, myeloid cells) seem to have the highest demand for vit B12 [22-24]. Cyanocobalamin is the most stable and broadly used form of vit B12, and has hematopoietic activity seemingly similar to that of the antianemia agent in purified liver extraction. Daily vit B12 requirement is 2-5 mg [25, 26]. Vit B12 is serves as indispensable for generation of DNA, and thus is necessitated for the cultivation and separation of practically all cells [27]. Helps catalyze the transformation of folic acid to its active form [28]. Active folic acid then partakes in copious responses indispensable for DNA generation [29]. Dietary origins: Paramount origin of vit B12 is from microbial synthesis. Previously, humans must acquire the preponderance of their Vit B12 by consuming animal products. Liver and dairy products are particularly reasonable origins. Between 10% & 30% of adults above age 50 are incapable to absorb vit B12 found innately in foods. Coinciding, these people should encounter their requirement by consuming B12-fortified foods [30-32].
In the majority of cases, vit B12 deficiency is the result of defective absorption (pernicious anemia are impaired production of intrinsic factor mandatory for absorption of vit B 12). Inadequate Vit B12 in the diet is a rare cause of deficiencies. Potential causes of poor absorption involve (1) regional enteritis, (2) celiac disease (a malabsorption syndrome (e.g inflammatory bowel disease, small bowel resection etc) including anomalies in the intestinal villi), and (3) development of antibodies instructed fight the vit B12 intrinsic and diseases that influence distal ileum [33-35]
Absorption: Effective absorption of Vit B12 requires intrinsic factor, a compound generated by parietal cells of the stomach. In the absence of intrinsic factor, absorption of vit B12 is highly decreased. Although, about 1% of the amount available can quiet be absorbed by passive diffusion [36, 37].
Distribution: In the blood, Vit B12 is bound to transcobalamin II, a particular B-globulin carrier protein, and is distributed and stored firstly in the liver and bone marrow [38, 39].
Elimination: Around 3-8 mcg of Vit B12 is generated into the GI tract daily via the bile; in health subjects with adequate intrinsic factor, all but around 1 mcg is re-absorbed. Excretion of vit B12 takes place extreme sluggishly: Daily destructions are around 0.1% of total body stores. Because Vit B12 is excreted so sluggishly, years are needed for Vit B12 deficiency to advance even with no replacement of missing Vit B12 taking place [40-42]
Folate serves as an indispensable factor for DNA generation. Without folic acid, DNA duplication and cell separation cannot continue [43, 44]

Absorption: Unaltered folic acid is preferably and out rightly absorbed in the proximal jejunum. 5 -20 mg of folate are stored in the liver and other tissues [46].
Elimination: Folates are excreted in the urine and stool [47].
Dietary origins: A reasonable origin encloses liver, peas, oranges, whole-wheat products, asparagus, beets, broccoli, and spinach and also involves yeast, kidney and green vegetables [48, 49].
Two most causes: Poor diet (specifically seen in alcoholics), and malabsorption secondary to intestinal diseases. Also, some medicines such as phenytoin, oral contraceptive, isoniazid, methotrexate etc are cause of folic acid deficiencies. Either acute or chronic alcoholism, perhaps the most ubiquitously cause of folate deficiency [50, 51]
Causes of aplastic anaemia: Medicines such as analgesic (pyrazolone eg: (dipyrone)), antithyroid (thiouracil), antibacterial (chloramphenicol and sulphonamide), antiepileptic (rimethadione), antineoplastic medications (cytotoxic medications) [52]
Antianaemic medications
The goal of anemia therapy are: To correct the underlying etiology (eg, restore substrates needed for RBC production), replace body stores to improve red cell oxygen-carrying capacity To alleviate signs and symptoms return of normal function and quality of life, and prevention or reversal of long-term complications such as neurologic complications of vitamin B12 deficiency.
Cyanocobalamine (Vit B12): Preparations [53, 54] are listed beneath: (1) Cyanocobalamine: I.M. for life 1 mg (2) Hydroxocobalamine I.M. for pernicious anemia and cyanide poisoning
Indications and usage: Dietary deficiency of vit B12 happening in only vegetarians (isolated vit B12 deficiencies is very rare) [55]. Malabsorption of vit B12 results from structural or functional detriment to the stomach, where intrinsic factor is generated, or to the ileum, where intrinsic factor facilitates vit B12 absorption. Parenteral (intramuscular) administration of vit B12 comprehensively reverses the megaloblastic anemia and GI symptoms of vit B12 deficiency; the grade of advancement in neurologic symptoms based on the continuance and severe of the injuries, however development of the injuries is instantaneously arrested [56-58]. For pernicious anemia and macrocytic anemia [59], neuropathies [60], hepatitis [61], and against catabolic action of cortisone [62]
Side effects: Cyanocobalamin is universally void of severe adverse effects. One potential response, hypokalemia, perhaps happens as a natural outcome of increased erythrocyte generation [63, 64].
Contraindications: Sensitiveness to cobalt and/or vitamin B12 or each constituent of the medicine is a contraindication [65].
Drug interactions: Colchicine, para-aminosalicylic acid and heavy alcohol input for lengthy than 2 weeks perhaps generate malabsorption of vitamin B12 [66].
Dosage and administration: The recommended initial dose of nascobal nasal spray is one spray (500 mcg) administered in one nostril once weekly. Nascobal nasal spray should be administered at least one hour before or one hour after ingestion of hot foods or liquids. Periodic monitoring of serum B12 levels should be acquired to settle sufficiency of therapy [67].
Mechanism of action: Iron figures the nucleus of the iron porphyrin heme ring, which coincidentally with globin chains figures hemoglobin that reversibly binds oxygen and provides the hypercritical mechanism for oxygen quittance from lungs to different tissues [68, 69].
Oral preparation: Ferrous sulphate - Ferrous gluconate - Ferrous fumarate - Iron choline citrate [70]
Parenteral preparation: Iron Dextran I.M, I.V and iron sorbitol citric acid complex I.M, only [71]
Dosage forms: Oral delay release tablet (324 mg; 325 mg); oral elixir (220 mg/5 mL); oral liquid ((as elemental iron) 15 mg/mL; 300 mg/5 mL); oral tablet (200 mg; 325 mg); oral tablet, prolonged release ((as elemental iron) 45 mg; 160 mg) [72, 73]
Mechanism of Action: : Iron combines with porphyrin and globin chains to figure hemoglobin, which is hypercritical for oxygen release from the lungs to different tissues. Iron deficiency causes a microcytic anemia owing to the formation of least erythrocytes with inadequate hemoglobin [74-76]. The recommended dose is one capsule (30 mg) taken twice a day, morning and evening. Take this medication on an empty stomach with half a glass of water (one hour before a meal, or at least 2 hours after a meal) [77, 78].
Indications: Iron deficiency anemia, blood destruction related to pregnancy or GI bleeding (NSAIDs), hookworm infestation, or surplus coffee [79]
Contraindications: Patients with hemochromatosis, hemosiderosis or hemolytic anemia [80]
Side Effects of oral Fe preparation: Therapeutic doses; dose related nausea, upper abdominal pain, constipation or diarrhea. Iron overdose (1-2 g) can lead to circulatory collapse and death. Non-intentional iron overdose has been a leading cause of fatal poisoning in children <6>
Drug interactions of FESO4: FESO4 perhaps decrease the absorption of different medicines, and take FESO4 dose 2 to 6 hours before or after taking each of the following an antacid; an antibiotic; or a laxative [82, 83]
Mechanism of Action: Identical as ferrous sulfate (but has a different’ route of administration) [84]
Indications: Rare used currently (fresh orally effective agents involving iron sucrose & ferric gluconate complex are most ubiquitously used) [85]. Kept for patients with iron deficiencies who are incapable to tolerate oral iron cannot absorb oral iron (e.g. due to inflammatory bowel diseases influencing the proximal small bowel, post-gastrectomy conditions, or subsequent small bowel resection) [86]. Ferric gluconate & iron sucrose are two optional parenteral forms of iron that can be given i.v., but should not be given intramuscularly [87].
Iron dextran is bestowed by deep i.m. injection or i. v [88]. Most adults with iron deficiency necessitate 1-2 g of replenishment iron, or 20-40 ml. The suitable route of administration is i.v. infusion in several hundred mls of normal saline over 1-2 hrs [89].
Side Effects: Further dose-dependent side effects analogized to administering oral iron addendums, which limits the dose that can be given. Side effects involve: Local toxic effect: Local pain & tissue staining (brown discoloration) [90]. Systemic toxic effect (chronic toxicity = Haemosidrosis): headache, light-headedness, fever, nausea, convulsions, tachycardia & hypotension, muscle and joint pains, haemolysis, flushing, urticaria, bronchospasm, and rare anaphylaxis & death [91].
Drug interactions of iron: Absorption of oral iron perhaps decreased by calcium and magnesium salts (such as magnesium trisilicate). Administration of iron preparations with such compounds should be divided by at least 2 hours [92]. Oral iron is understood to decrease the absorption of penicillamine, bisphosphonates, ciprofloxacin, entacapone, levodopa, levofloxacin, levothyroxine (thyroxine) moxifloxacin, mycophenolate, norfloxacin and ofloxacin. These medications should be given at least 2 hours separate from oral iron medicines such as ferrous sulphate; ferrous gluconate; ferrous fumarate and iron choline citrate [93, 94]. Absorption of both iron and antibiotic perhaps decreased if oral iron is given with tetracycline [95]. Administration of iron preparations and tetracyclines should be divided by 2 to 3 hours [96]. Coincident usage of iron and dimercaprol is nephrotoxic [97]. Coincident usage of chloramphenicol will delay plasma iron clearance, integration of iron into red blood cells and interpose with erythropoiesis [98]. Coincident usage of iron with methyldopa perhaps antagonizes the hypotensive consequence of methyldopa [99].
Deferoxamine: Iron overdose can be treated by gastric lavage with a phosphate solution and deferoxamine (iron chelator) [100].
Mechanism of Action:Binds iron acquisitive, but poorly binds to different indispensable trace metals [101]. It contests in binding loosely bound iron, but fails to bind iron that is biologically chelated, such as in microsomal and mitrochondrial cytochromes and hemoproteins [102]
Indications: Iron poisoning. Used for treating both acute iron intoxication and in patients with secondary iron excessive from multiple transfusions [103]. Deferoxamine plus hemodialysis perhaps also be actionable in treatment of aluminum toxicity in renal failure. (It is not indicated for the treatment of primary hemochromatosis, since phlebotomy is the method of preference for removing overload iron in this disorder) [104]
Pharmacokinetics: Given parentally (i.m take your ferrous sulfate dose 2 to 6 hours before or after taking any of the following: an antacid; an antibiotic; or a laxative., s.c. or i.v.) [105]. It is poorly absorbed if taken orally, and perhaps frankly accelerates iron absorption if given orally. Iron-chelator complexes are excreted in the urine, frequent turning the urine an orange-red color [105]
Contraindications: Patients with severe renal disease or anuria, since the medicine and the iron chelate are excreted firstly by the kidney [107]
Side Effects: Fast i.v. administration perhaps cause hypotension. Idiosyncratic feedbacks such as
Two figures inactive active to launch with the inactive figure is referred to as folacin, folate, or folic acid; the active figure is referred to as leucovorin calcium, folinic acid, or citrovorum factor. The inactive figure is by widely the most ubiquitously used preparation [109].
Mechanism of Action: Indispensable cofactor for production of amino acids, purines and DNA [110]
Routes of Administration and dosage: Folic acid is applicable in tablets (0.4, 0.8, and 1 mg) for oral use and in a 5-mg/mL solution [Folvite] for IM, IV, or subcutaneous injection [111]. For treatment of folate- deficiency megaloblastic anemia in adults, the ordinary oral dosage is 1000-2000 mcg/day. Once symptoms have determined, the maintenance dosage is 400mcg/day. For prophylaxis during pregnancy and lactation, doses up to 1000 mcg/day perhaps used [112].
Indications:Treatment of megaloblastic anemia’s owing to a deficiency of folic acid as perhaps seen in equatorial or non- equatorial sprue, in anemia of nutritional origin, pregnancy, infancy, or childhood [113]. A decreased figure of folic acid known as citrovorum factor (or leucovorin) is given to replace endogenous folic acid in patients on methotrexate (which suppresses dihydrofolate reductase). Citrovorin (leucovorin) is better absorbed analogized to folic acid [114], for malabsorption syndrome [115], with anticonvulsant medications as phenobarbitone, primidone or phenytoin to counteract associated macrocytic anaemia [116].
Contraindications: Folic acid should not be given alone in patients with pernicioius anemia without knowing whether they also have Vit B12 deficiency [117]. The jeopardy is that folic acid addendums can disguise the signs of Vit B 12 deficiency, yet not inhibit the advancement of irreversible neurological damage owing to Vit B12 deficiency [118]. The Shilling test can be used to test for abnormalities in Vit B12 absorption [119].
Pharmacokinetics: 1 mg of folic acid orally quotidian is usually adequate to reverse megaloblastic anemia & renew normal folate levels [120].
Side Effects: Allergic sensitization [121, 122]
Developed using recombinant DNA technique and includes [123]
Erythropoietin: EP synthesized firstly by renal cortex, used chiefly in treatment ofanemia owing to chronic renal failure. But can be used also in AIDS and in anemia of cancer therapy [124].
Mechanism of Action: Has glycoprotein that stimulates red blood cell generation. Epoetin alfa is a 165 amino acid glycoprotein developed by recombinant DNA technology, and has the identical biological outcomes as endogenous erythropoietin [125]. Hypoxia is the dominant physiological encourage for erythropoietin generation in the body [126]
Indications: For therapy of anemia in chronic renal failure patients [127], for Zidovudine-treated HIV-infected patients, cancer patients on chemotherapy decreasing of syngeneic blood transfusion in surgery patients. Erythropoietin deficiency can sequence from compromised renal function (its primitive site of synthesis). Erythropoietin paucity results in a normocytic anemia [128, 129].
Contraindications: Uncontrolled hypertension or known hypersensitivity to either mammalian cell-derived products or to human albumin [130].
Pharmacokinetics: Given i.v. or s. c. Half-life of EP alfa is 4-13 hrs in patients with chronic renal failure. It is calculated in international units (IU) [131].
Side Effects: A fast accelerates in hematocrit & hemoglobin perhaps causes hypertension & thrombotic complications. These can be minimized by enhancing the hematocrit sluggishly and treating the hypertension [132].
2. Thrombopoietin is a cytokine that elevates platelet count when combined with different cultivation factors [133]. The cue cytokine is thrombopoietin (TPO). It regulates multiplication and development of megakaryocytes as well as platelet generation. TPO is generated in the liver. Full-length recombinant, eminently glycosylated human TPO (rhTPO) was produced in Chinese hamster ovary cells. Non-glycosylated figure of TPO produced in Escherichia coli.
3. Granulocyte / marcrophage colony- stimulating factor (GM-CSF): used to stimulate myelopoiesis in AIDS, aplastic anemia and cancer chemotherapy [134].
4. Granulocyte colony- stimulating factor (G-CSF) is used to treat severe neutropenia following bone marrow transplantation or cancer chemotherapy [135]. Granulocyte colony-stimulating factor (G-CSF) and granulocyte-macrophage colony-stimulating factor (GM-CSF) accelerate the antimicrobial works of mature neutrophils. G-CSF others from GM-CSF in its particularity of action on advancing and mature neutrophils, its effects on neutrophil kinetics, and its toxicity profile.
5. Interleukins (IL 1, 3, 5, 6, 9, 11) act synergistically with stem cell agent (SCF), GM-CSF, G-CSF and erythropoietin [136].
Anemia is a group of infirmities delineated by de-escalate in Hb or RBCs, sequencing in downgraded oxygen-carrying capacity of blood. Quotidian demand of Fe in male is 10mg and female 15 mg, iron seek is escalates in growing children, pregnant and lactating women owing to their body escalated demand for iron. Vit B12 is made up of a porphyrin-like ring with a central cobalt atom bind to a nucleotide. Ferrous sulfate perhaps de-escalates the absorption of distinctive medicines, and take ferrous sulfate dose 2 to 6 hours before or after taking any of the following: an antacid; an antibiotic; or a laxative. Folic acid is applicable in tablets (0.4, 0.8, and 1 mg) for oral use and in a 5-mg/mL solution [Folvite] for IM, IV, or subQ injection.
Anemia is a group of diseases defined by decrease in Hb or RBCs, resulting in decreased oxygen-carrying capacity of blood. Daily requirement of Fe in male is 10mg and female 15 mg, iron need is accelerating in growing children, pregnant and nursing women owing to their body enhanced demand for iron. Vit B12 is made up of a porphyrin-like ring with a central cobalt atom bind to a nucleotide. Ferrous sulfate perhaps decreases the absorption of different medicines, and take ferrous sulfate dose 2 to 6 hours before or after taking any of the following: an antacid; an antibiotic; or a laxative. Folic acid is applicable in tablets (0.4, 0.8, and 1 mg) for oral use and in a 5-mg/mL solution [Folvite] for IM, IV, or subQ injection
that increase the quality of this manuscript.
Data Sources: Sources searched include Google Scholar, Research Gate, PubMed, NCBI, NDSS, PMID, Scopus database; Lancet; Science direct; PMCID, and Cochrane database. Search terms included: antianaemic medications
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
