
Research Article | DOI: https://doi.org/10.31579/2692-9562/111
1 Otolaryngology Department, Hospital San Juan de Dios, Otolaryngology Department, Faculty of Medicine, Universidad de Chile.
2 Otolaryngology Department, Clínica Alemana de Santiago. Santiago, Chile.
3 Immunology and Allergies Department, Clínica Alemana de Santiago. Santiago, Chile.
4 Pathological Department, Clínica Alemana de Santiago. Santiago, Chile.
5 Otolaryngology Department, Hospital San José.
6 Otolaryngology Department, Clínica Las Condes, Santiago, Chile.
*Corresponding Author: Jose Miguel Contreras, Otolaryngology Department, Hospital San Juan de Dios, Otolaryngology Department, Faculty of Medicine, Universidad de Chile.
Citation: Jose M. Contreras, Sebastián Castro M., Patricia Roessler V., Alejandro Paredes W, Jeannie Slater, (2024), An Unusual Cause Of Laryngotracheal Airway Narrowing, Journal of Clinical Otorhinolaryngology, 6(2); DOI:10.31579/2692-9562/111
Copyright: © 2024, Jose Miguel Contreras. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 30 January 2024 | Accepted: 13 February 2024 | Published: 19 February 2024
Keywords: IgG4-related disease; head and neck; larynx; subglottic; head and neck; larynx; subglottic
Immunoglobulin (Ig) G4-related disease is a medical condition of recent knowledge that can compromise any organ, having preferences for certain regions of the body, where the head and neck region is one of the main affected points, being able to affect orbit, salivary glands, lacrimal glands, thyroid gland, paranasal cavities, temporal bone, pharynx, and larynx. The latter is infrequently compromised, with only 12 cases registered in the literature before the publication of this writing. We present a case of a 49-year-old woman with a history of exertional dyspnea, diagnosed with a sub-glottic stenosis which was managed surgically with laryngotracheal reconstruction. The histopathological study revealed histology compatible with IgG4-related disease, so medical treatment with oral corticosteroid therapy was started for 2 months in conjunction with immunology. After 4 years of follow-up, the patient has not presented relapses, maintaining an adequate subglottic lumen.
The authors declare that they do not have conflicts of interest.
Immunoglobulin-G4-related disease is an immune-mediated, inflammatory, fibrosclerotic, systemic disease, which is characterized by the formation of masses causing permanent organic damage and eventually death if it does not receive adequate treatment1,2.
The global incidence and prevalence of this disease are unknown and probably underestimated. It affects middle-aged and elderly people, with a male-to-female ratio of 1.6:1 in the head and neck region (4:1 in other regions). Currently, there are no recognized risk factors1.
Its clinical presentation can be classified into four phenotypes3: pancreatic-hepatobiliary disease (31%), retroperitoneal fibrosis with or without aortitis (24%), disease limited to the head and neck (24%), and Mikulicz syndrome with systemic disease (22%). Each of these groups presents distinctive clinical, epidemiological, and serological characteristics that can guide both diagnosis and therapy in the future2,3.
Here, we report a clinical case of laryngeal involvement associated with IgG4-related disease. This work was carried out with the patient's informed consent for publication of her story and photographs
49 years-old, female, with a history of asthma was treated with salbutamol SOS, without a history of trauma to the neck or recent surgery and arrived at the consultation in March 2017 due to a two-year history of slowly progressive respiratory obstruction, with dyspnea on exertion and a functional capacity grade II-III.
Flexible laryngoscopy revealed normal vocal folds with preserved mobility. Immediately below them, an oval-shaped narrowness with a smaller diameter laterally, without apparent inflammation or ulceration. She presented with two computed tomography (CT) scans of the neck from 2015 to 2016, in which progressive airway stenosis at the subglottic level, immediately under the vocal folds, was observed. The airway stenosis progressed from 9 mm to 8,5 mm on the anteroposterior (AP) diameter and from 4 to 3 mm on the lateral diameter (Figure 1 and 2).
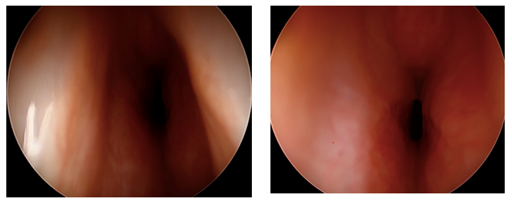
Figure 1and 2: Photographs obtained from the first airway revision (Pre-Operative).
Airway evaluation under general anesthesia was performed on May 3, 2017, where subglottic stenosis was confirmed with a diameter of 4 × 8 mm in the lateral and AP diameters, respectively. The measured longitude was 10 mm from the cranial to the caudal limits. The patient was diagnosed with suspected idiopathic subglottic stenosis. After team consultation, laryngo-tracheoplasty with anterior and posterior costal cartilage grafts supported by a Montgomery T tube was performed during the same procedure.
The definitive pathology of the diseased laryngeal tissue reported laryngeal mucosa with marked interstitial inflammatory infiltrates of predominantly lymphoplasmacytic infiltration with isolated foci of leukocyte exacerbation, edema, and interstitial fibrosis. The lymphoplasmacytic infiltrate was polytypic for Lambda and Kappa light chains without angiitis or granulomas. Immunohistochemistry revealed 86 IgG4-positive plasmacytes per high-power field (Figures 3, 4, and 5).
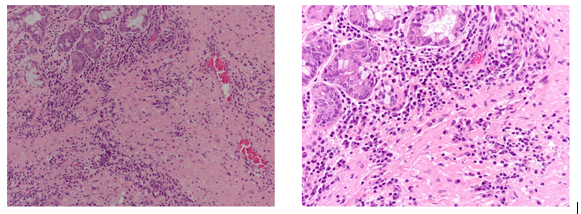
Figure 3 and 4: Microscopic images of histology obtained from the tissue biopsy, stained with hematoxylin-eosin at a magnification of 10x and 20x Images show fibrosis of the lamina propria and predominantly plasmacytic inflammatory infiltrate.
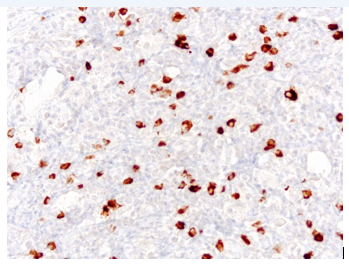
Figure 5: Microscopic histology image obtained from the tissue biopsy, stained with IgG4 at 20x magnification.
In these images, one month after the removal of the Montgomery T-tube, an adequate subglottic lumen is observed, thickening of the anterior commissure, an area of yellowish appearance in the anterior region corresponding to the integrated cartilage.
Immunology was consulted in May of 2017. Chest and abdominal computed tomography (CT) scans were performed, but no other alterations due to IgG4 were observed. In addition, levels of ANCA C and P, IgG, IgM, IgE, IgA, C3, and C4, IgG subclasses 1,2,3,4 in plasma were within normal limits.
A stenosis secondary to a lymphoplasmacytic lesion due to IgG4 was the definitive diagnosis, and treatment with prednisone was started for 2 months until July 2017 in conjunction with immunology.
The T tube was removed on June 13, 2017, in the operating room, observing good post-operative lumen. At follow-up 3 months after surgery, she had a normal voice, no dyspnea on exertion, and no stridor. Endoscopic examination revealed thick vocal folds, a slight whitish subglottic bulk located in the stenotic area repaired with cartilage, and a good diameter of > 1 cm (Figure 6 and 7).
Lymphocytes stained with marker for IgG4 in the tissue obtained.

Figure 6 and 7: Images obtained after removal of the Montgomery T-Tube after laryngotracheal reconstruction.
After one year of follow-up, she presented with immunoglobulin tests within normal limits and was discharged from the immunology department. Currently, in March 2023, she has remained without dyspnea, dysphonia, stridor, or neck pain.
The classic presentation of IgG4-related disease in the head and neck is characterized by a painless mass of progressive growth, with the main locations at the orbital level (>50%), salivary glands (20%), and thyroid (4%). This disease can be multifocal and involves virtually any organ in this region, with reported cases at the level of the paranasal sinuses, temporal bone, pharynx, and larynx. Over 90% of patients do not present with systemic symptoms, but up to 10% may present with an acute-onset disease associated with weight loss or fever7.
With respect to laryngeal involvement, it is very rare, and its incidence is unknown. Currently, only 12 cases have been reported in the literature, which are described in Table 1 8-17.
| Author and Year of Publication | Patients | Age | Gender | Symptoms | Clinical Findings | IgG4 serum levels | Treatment | Follow-up |
| Volker et al. 2009 | 1 | 56 | Male | 6 months of dysphonia | Increased supraglottic volume in the left ventricular band with destruction of ipsilateral thyroid cartilage and cervical lymphadenopathy | N/E | Steroids therapy for 24 months | - |
| Shaib et al. 2013 | 2 | 56
57 | Male
Male | 12 years of evolution of dysphonia associated with dyspnea on exertion 16 years of evolution of chronic laryngitis and aphthous stomatitis, along with genital ulcers | Stenosis in the anterior subglottic region and bilateral vocal fold immobility. Lung and prostate involvement.
Signs of chronic laryngitis | Increased IgG4 serum levels
Increased IgG4 serum levels
| Tracheostomy + Steroids therapy (Prednisone)
Steroids therapy (Prednisone) | |
| Khoo et al. 2014 | 1 | 62 | Male | Chronic cough with brownish sputum, associated with odynophagia and sensation of pharyngeal globus | Papillomatous tumor that involved both aryepiglottic folds, with involvement of the left piriformis sinus | Normal serum levels | High-dose steroid therapy (Prednisone) for 12 weeks. Low dose prednisone (5mg) for 2 years. | |
Reder et al. 2015
| 2 | 58
62 | Male
Male | 4 years of pharyngeal globus sensation on the right side and dysphonia Chronic cough associated with throat clearing, dysphagia and dysphonia | Increase in granular volume at the base of the tongue and left aryepiglottic fold, left piriformis sinus and exophytic tumor in the right vocal process Granular edema at the base of the tongue and epiglottis, with keratosis at the level of the ventricular bands and vocal cords. | Increased IgG4 serum levels Increased IgG4 serum levels
| Steroid therapy (intravenous methylprednisolone 100 mg/day) + Rituximab (2 doses of 1 gram separated by 15 days) Steroid therapy (intravenous methylprednisolone 100 mg/day) + Rituximab (2 doses of 1 gram separated by 15 days) | 2 years, without relapse. 1 year, with a relapse managed with Rituximab |
| Hamadani 2018 | 1 | 54 | Female | 6 months of evolution of dysphagia, weight loss, odynophagia and dysphonia | Signs of chronic laryngitis at the supraglottic level, along with an ulcerated lesion at the retrocricoid level | Increased IgG4 serum levels
| N/E | N/E |
| Hill et al 2020 | 1 | 29 | Male | Dysphonia, odynophagia and dysphagia to solids and liquids of 6 months of evolution | Supraglottic edema especially in the right arytenoids | Increased IgG4 serum levels
| Oral corticosteroid therapy (Prednisone) + Mycophenolate Mofetil | |
| Matsushima et al. 2020 | 1 | 50 | Male | Dyspnea | Supraglottic mass dependent on the left arytenoid region | Surgical debulking + Steroid therapy | ||
| Syed et al. 2020 | 1 | 64 | Male | Dysphonia, dyspnea and persistent non-productive cough | Signs of chronic laryngitis | Rituximab | ||
| Suárez-Diaz et al. 2020 | 1 | 37 | Female | Dysphonia of 3 years of evolution, associated with outbreaks of recurrent painful ulcers | Signs of chronic laryngitis | Increased IgG4 serum levels | Corticosteroid therapy (IV induction Methylprednisolone and then maintenance Prednisone) + Azathioprine | |
| Atienza-Mateo et al. 2021 | 1 | 30 | Female | 4 months of evolution of dyspnea during exercise | Subglottic stenosis involving 50% of the lumen, membranous | Normal IgG4 serum levels
| Surgical management: Endoscopic + Cricotracheal resection. Medical management: Steroid therapy + Rituximab | No relapse at 4 years of follow-up |
| Contreras et al. 2023 | 1 | 49 | Female | 2 years of evolution of progressive exertional dyspnea | Subglottic stenosis of 8.5 x 3 mm in diameter | Normal IgG4 serum levels
| Surgical management: Laryngotracheal reconstruction with anterior and posterior graft Medical management: Oral corticosteroid therapy | No relapse after 3 years of follow-up |
Table 1: Cases reported in the literature of laryngeal involvement due to IgG4-related disease.
Although this disease does not present a defined pattern in the larynx, one of the most frequent manifestations is laryngitis, characterized by edema and erythema at the supraglottic level, whether generalized or localized, along with fibrotic lesions at the supraglottic, glottic, or subglottic level. We recommend having this diagnosis in our differentials when faced with a lesion or an inflammatory mass of the larynx with a non-specific appearance.
Complementary and Diagnostic Studies
Laboratory tests were nonspecific. The erythrocyte sedimentation rate and C-reactive protein level may be slightly elevated or normal2. These patients frequently present with elevation of the different IgG subclasses (IgG1, 2, and 3), but not in the same proportion as IgG4. Furthermore, plasma levels of complement molecules (C4-C3) may decrease, reflecting probable kidney disease18.
IgG4 immunoglobulin levels are elevated in 55 – 97% of cases, correlating with the number of organs involved. Considering a cut-off value of 1.35 to 1.44 g/L, the sensitivity and specificity for this test were 87.2 and 82.6%,
respectively. Currently, this test is considered as a screening tool, with poor diagnostic utility, because up to 30 - 50% of patients with this disease have normal serum levels2,5,19.
Regarding the imaging study, both CT and MRI are used to rule out systemic involvement of the disease. On the other hand, it was proposed that PET-CT can help both identify asymptomatic disseminated disease, allow directed histological study, and monitor the response to treatment; however, more studies are needed2.
Currently, histological examination is the gold standard for the diagnosis of this disease18. Nonetheless, the diagnosis is currently based on the classification criteria published in 2019 by the American College of Rheumatologist/European Alliance of Associations for Rheumatology (ACR/EULAR), described in Table 2 20.
| Steps | Categorical evaluation or numerical assessment |
Step 1: Inclusion Criteria Characteristic* clinical or radiological involvement of a typical organ (e.g., pancreas, salivary glands, bile ducts, orbits, kidney, lung, aorta, retroperitoneum, pachymeninges, or thyroid gland [Riedel thyroiditis]) Or pathological evidence of an inflammatory process accompanied by a lymphoplasmacytic infiltrate of uncertain etiology in one of these same organs | Yes or No |
Step 2: Exclusion Criteria Clinical Fever No objective response to glucocorticoids
Serological Unexplained leukopenia and thrombocytopenia Peripheral eosinophilia Positive antineutrophil cytoplasmic antibody (specifically against proteinase 3 or myeloperoxidase) Positive SSA/Ro or SSB/La antibody Positive double-stranded DNA, RNP or Sm antibody Another disease-specific autoantibody Cryoglobulinemia
Radiologic Known radiological findings suspected of malignancy or infection that have not been sufficiently investigated Rapid radiological progression Long bone anomalies consistent with Erdheim-Chester disease Splenomegaly
Pathological Cellular infiltrates suggestive of malignancy that have not been sufficiently evaluated Markers compatible with inflammatory myofibroblastic tumor Prominent neutrophilic inflammation Necrotizing vasculitis Prominent necrosis Mainly granulomatous inflammation Pathological features of macrophage/histiocytic disorder
Known diagnosis of the following: Multicentric Castleman disease Crohn's disease or ulcerative colitis (only if pancreatobiliary disease is present) Hashimoto's thyroiditis (only if the thyroid is affected) | Yes or No |
If the case meets the inclusion criteria and does not meet any exclusion criteria, continue with step 3 | |
Step 3: Inclusion Criteria: Domains and Items
Histopathology Non-informative biopsy Dense lymphocytic infiltrate Dense lymphocytic infiltrate and obliterative phlebitis Dense lymphocytic infiltrate and storiform fibrosis with or without obliterans phlebitis
Immunohistochemistry
Serum IgG4 concentration Normal or unmarked 0 > Normal but <2> 2-5 × upper limit of normal > 5 × upper limit of normal
Bilateral lacrimal, parotid, sublingual and submandibular glands No set of glands involved A set of glands involved Two or more sets of glands involved
Chest None of the items listed are present Peribronchovascular and septal thickening Band-shaped vertebral soft tissue in the chest
Pancreas and biliary tree None of the items listed are present Diffuse enlargement of the pancreas (loss of lobulations) Diffuse enlargement of the pancreas, with a capsule-shaped border and decreased contrast. Involvement of the pancreas (any of the above) and the biliary tree
Kidney None of the items listed are present Hypocomplementemia Renal pelvis/soft tissue thickening Low density areas in bilateral renal cortex
Retroperitoneum None of the items listed are present Diffuse thickening of the abdominal aortic wall Circumferential or anterolateral soft tissue around infrarenal aorta or iliac arteries |
0 + 4 + 6
+ 13
0-16, as follows: - The score assigned is 0 if the IgG4+:IgG+ ratio is 0-40% or indeterminate and the number of IgG4+ cells/highest power field (cma) is 0 to 9. - The assigned weight is 7 if 1) the IgG4+:IgG+ ratio is ≥41% and the number of IgG4+ cells/cma is 0-9 or indeterminate; or 2) the IgG4+:IgG+ ratio is 0-40% or indeterminate and the number of IgG4+ cells/cma is ≥10 or indeterminate. - The assigned weight is 14 if 1) the IgG4+:IgG+ ratio is 41-70% and the number of IgG4+ cells/cma is ≥10; or 2) the IgG4+:IgG+ ratio is ≥71% and the number of IgG4+ cells/cma is 10–50. - The assigned weight is 16 if the IgG4+:IgG+ ratio is ≥71% and the number of IgG4+ cells/cma is ≥51.
0 + 4 + 6 + 11
0 + 6 + 14
0 + 4 + 10
0
+ 8
+ 11
+ 19
0 + 6 + 8 + 10 0 + 4 + 8 |
Step 4: Total inclusion points
A case meets the classification criteria for IgG4-RD if the inclusion criteria are met, the exclusion criteria do not apply, and the total points are ≥20. | |
Table 2: Classification criteria for IgG4-related disease by ACR/EULAR 2019.
Treatment
The treatment of IgG4-related diseases limited to the head and neck, based on expert opinion and retrospective studies, is based on three strategies:
1. Conservative management: Clinical observation is recommended in cases of increased growth of the submandibular gland and/or an asymptomatic increase in the size of neck lymphadenopathy, without evidence of progression or associated organ dysfunction [1].
2. Surgical management: This plays a key role in obtaining biopsies for histological diagnosis. However, it may be an option for the management of patients in the “fibrotic phase” of the disease [1,6].
3. Medical management: management of choice for all patients with this disease. It is divided into two parts: induction and maintenance therapies. This treatment is most effective during the “inflammatory phase” of the disease; therefore, early diagnosis and management are essential to achieve the best outcomes1.
Induction therapy, the use of systemic steroids, is recommended as first-line therapy, at a dose of 0.6-1 mg/kg/day of prednisone or another equivalent dose for 2-4 weeks and with gradual tapering over a period of time between 3 and 6 months, reporting a response rate of up to 93%[2,21]. The use of biological therapy, specifically rituximab (anti-CD20 monoclonal antibody), to achieve remission of this disease is in development, with a remission rate of 67–83% of cases, allowing steroids to be discontinued early [2,21]. However, 46–90% of patients treated with steroids relapse within the first 3
years from diagnosis, either in the same affected organ or at a different site[2].
Maintenance therapy is recommended for patients who present a high risk of relapses, including multi-organ disease, elevated IgG4 and IgE levels, and/or peripheral eosinophilia, and in patients with presentations with severe organ damage. This therapy is based on low-dose corticosteroids or any disease-modifying or biological drugs. In general, therapy is maintained for an average of 3 years with clinical, biochemical, and radiological follow-up until complete remission of the pathological findings[2,21].
IgG4 related disease is an emerging disease, and disease limited to the head and neck is the second most frequent manifestation.
There are few reports of laryngeal involvement, with only 2 cases of subglottic stenosis published prior to our study. Although medical management is the cornerstone for definitive treatment of the disease, surgical management can be an alternative to the “fibrotic” phase of this disease. However, more studies are needed to determine the most appropriate behavior in these situations.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
