
Research Article | DOI: https://doi.org/10.31579/2690-8794/120
Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh.
*Corresponding Author: Richmond Ronald Gomes, Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka Bangladesh.
Citation: Richmond R Gomes (2022) An Unusual cause of Chest pain and Dyspnea in an Elderly: Giant Intrathoracic Haital Hernia J, Clinical Medical Reviews and Reports. 4(4); DOI: 10.31579/2690-8794/120
Copyright: © 2022, Richmond R Gomes, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 December 2021 | Accepted: 06 January 2022 | Published: 04 February 2022
Keywords: hiatal hernia, dyspnea, chest pain, retro cardiac air fluid level
Giant hiatal hernias, generally seen at advanced ages, can rarely cause cardiorespiratory symptoms such as dyspnea and chest pain. Here, we aimed to present a case with a large hiatal hernia that largely protruded to intrathoracic cavity and caused dyspnea, particularly at postprandial period.We report a case of a 74-year-old female who presented with one month history of progressive shortness of breath and left sided chest pain. Upon arrival, the patient was found to be hypoxic with oxygen saturation 90% on room air. Physical examination also showed decreased breath sounds on left mid to basal lung with shifting of trachea and apex beat to right side. Plain radiograph demonstrated an increased opacity at the left lower lobe with retro-cardiac air fluid level; Subsequent computerized tomography of the chest revealed a giant hiatal hernia, containing stomach, duodenum, colon and spleen. This case highlights the giant hiatal hernia as an unusual cause of shortness of breath and chest pain, especially in elderly patients.
Hiatal hernia is defined as abnormal protrusion of stomach with another intra-abdominal organ, in some cases, above diaphragm from esophageal hiatus. A giant hiatal hernia is defined by a hernia that consists of >30% of the stomach herniating through the diaphragmatic hiatus into the thorax1.Its prevalence has been reported as 0.8–2.9% in upper gastrointestinal endoscopy series. Here, we aimed to present a case with a hiatal hernia that largely protruded into thorax cavity, causing dyspnea and chest pain. Generally, patients with giant hiatal hernias often present with gastrointestinal symptoms such as dysphagia and heart burn, whereas cardio respiratory symptoms caused by hiatal hernias are extremely uncommon.1,2Hence, we report a case of a patient with a giant hiatal hernia who presented with progressive shortness of breath chest pain and hypoxia.
A 74-year-old woman, ex smoker presented to the outpatient clinic with increasing fatigue, shortness of breath with heaviness and pain in left side of chest over 1 month. She noted that her shortness of breath was aggravated with exertion and after the ingestion of food but there was no history of orthopnea or paroxysmal nocturnal dyspnea. The patient did not describe an underlying chronic disease such as hypertension, diabetes mellitus or coronary artery disease and denied use of any medication within the previous 6 months apart from occasional use of proton pump inhibitors and montelukast with minimal relief of her symptoms. She also had no history of fever, cough, hemoptysis, hematemesis, melana, loss of appetite, substantial loss of weight or other constitutional symptoms. She had history of blunt compressive trauma to the chest 15 days back. She also gave history of abdominal discomfort and heart burn after taking meal for last four years. Her bowel and bladder habit was normal. On the physical examination, vital signs was stable except respiratory rate 22 breath/min and pallor was observed at conjunctiva. Cardiovascular and abdominal examinations were non-conclusive apart from shifting of apex beat towards right. On respiratory system examination, patient is mildly dyspnoeic at rest with respiratory rate 20 breaths/min. Pulse oxymetry showed SaO2 90% in room air. Chest examination revealed restricted movement on the left side of the chest. Trachea is shifted to the right side. Chest expansibility is restricted over the left lower chest. Percussion note is dull in left 7th intercostal space downwards in scapular line. Breath sound and vocal resonance are diminished over the same area. In the laboratory evaluations, the following results were obtained: WBC, 7400/mm3; Hg%- 9.9 g/dL; MCV, 72.3 fL; MCH 22.2;Plt, 376.000/mm3
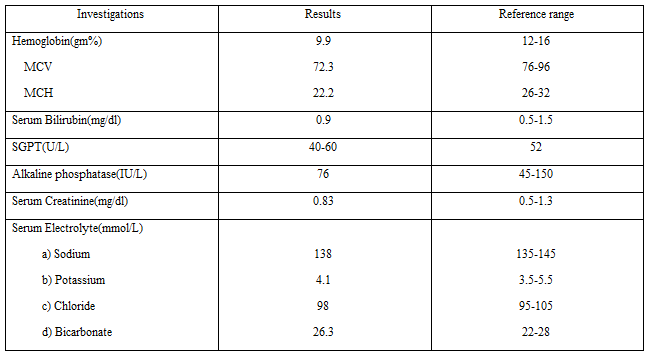
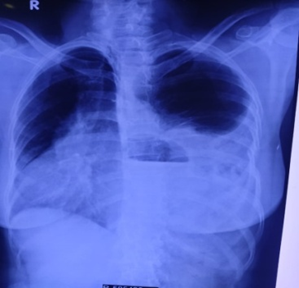
On chest radiograph posterior anterior view there was increased cardiothoracic index, enlarged mediastinum, and a mass appearance with an air-fluid level superposed with cardiac contours were observed (Figure 1).
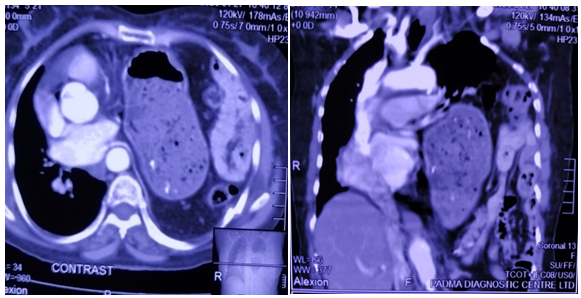
A thoracic CT scan including sagittal and coronal sections was performed in the patient because of the suspicion of a large hiatal hernia with available image. It was found that the stomach, spleen, part of both small and large gut was herniated into mediastinum without any finding of incarceration and gastrointestinal obstruction (Figure 2, 3).
On the upper gastrointestinal endoscopy, there were linear erosions at esophagogastric junction where hiatal hernia and diaphragmatic compression occurred. Active gastrointestinal bleeding was not observed (figure 4).

ECG, color doppler echocardiography showed no evidence of cardiac disease but there was significant compression of left atrium by large hiatal hernia.
Surgery and cardiology were consulted for surgical repair and pre-operative evaluation of the hernia. However, the patient refused surgery because of the high surgical risk due to advance age. The patient was discharged with frequent follow-up at the medicine clinic with life style medication advices, proton pump inhibitor and motility regulator therapy. Nutritional recommendations were also given.
Hiatal hernia is defined as abnormal protrusion of stomach with another intra-abdominal organ, in some cases, above diaphragm from esophageal hiatus3. Giant hiatal hernia is responsible for 0.3 to 15% of all hiatal hernias1.Type I hiatal hernia (sliding type) is the most commonly observed type in which gastroesophageal junction slides together with a part of the stomach4. Although the cause for the development of hiatal hernia is unknown, its incidence increases by advancing age5. It is accepted that relaxation at diaphragmatic crura resulting from aging process is the cause for the observation of more frequent and larger hiatal hernias in elder population6. Symptoms are often related to gastroesophageal reflux disease in hiatal hernias which is usually asymptomatic. Generally, older people are unable to describe typical reflux symptoms such as burning at chest, acid regurgitation, and epigastric pain. Gastrointestinal bleeding related to ulcer or erosion, iron deficiency anemia, mucosal prolapse, incarceration, and volvulus are the main complications of hiatal hernia. Particularly, the most frightening complications are the development of incarceration or volvulus4. Cardiorespiratory symptoms are considered a very uncommon clinical presentation.
In 2011, Alviaret al7reported a case of bilateral Bochdalek hernias presenting with respiratory failure that required noninvasive ventilator support. Later, in 2013, Torres et al8illustrated a case of an 82-year-old female who presented with dyspnea and oxygen desaturation and was found to have hiatal herniation of the stomach and pancreas. In 2014, Chou and Su9reported a case of an 86-year-old female who also presented with shortness of breath caused by giant hiatal hernia followed by Takotsubo cardiomyopathy.Siu et al. reported that a large hiatal hernia caused cardiac failure by the compression to the left atrium in a case presenting with recurrent acute cardiac failure attacks14.Interestingly, all reported cases were female over the age of 80 years with multiple comorbidities. None of them received surgical intervention for definite management.
In addition to shortness of breath as a rare presentation, hiatal hernia can also present with angina pectoris8,arrhythmias, recurrent heart failure7due to the extent of hernia and the compression to heart and pulmonary veins by organs protruded into thorax cavity13and exercise impairment10.
There is an increasing incidence of hiatal hernia with age, from approximately <10>60
In conclusion, large hiatal hernias should be considered in the differential diagnosis as a rare intra-abdominal cause of persistent iron deficiency anemia, dyspnea and chest pain. It should be kept in mind that large hiatal hernias can lead to cardiorespiratory symptoms and complications due to compression. Cases with large hiatal hernias should be assessed by physical examination, endoscopy of UGIT and imaging modalities such as CT scan of thorax.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
