
Case Report | DOI: https://doi.org/10.31579/2768-2757/084
Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi, India.
*Corresponding Author: Praneeth Kokkula, Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi, India.
Citation: Zuhour M., Baycar Z., Dadacı M., İnce B., (2023), An Uncommon Case of an Acute Onset Growing Skull Fracture: Case Report and Review of Literature, Journal of Clinical Surgery and Research, 4(4); DOI:10.31579/2768-2757/084
Copyright: 2023, Praneeth Kokkula. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 June 2023 | Accepted: 21 June 2023 | Published: 30 June 2023
Keywords: growing skull fracture; traumatic brain injury; leptomeningeal cyst
Growing skull fractures (GSF) are rare complications of pediatric skull fractures with a reported incidence of 0.05–1.6%. They are most commonly seen in children less than 5 years of age. Most commonly, the onset of symptoms from the time of trauma ranges from weeks to months, with very few cases reported in literature which have an acute onset within a few days. Here we present a case of a 2-year child with a history of traumatic linear skull fracture who had an acute onset of scalp swelling within 4 days of trauma. An MRI scan showed the presence of a GSF and urgent surgical repair in the form of duraplasty and cranioplasty was undertaken. Awareness regarding the possibility of an acute onset of GSF is important for neurosurgeons as early surgical repair has been shown to reduce neurological complications.
Growing skull fractures (GSF) are rare complications of pediatric skull fractures. Their reported incidence varies from 0.05–1.6% [1, 2]. They have been variously termed as leptomeningeal cysts, cranio-cerebral erosion, traumatic ventricular cysts, expanding skull fracture, traumatic malacia etc [3–5]. They represent an area of dural defect in the region of the traumatic skull fracture that creates the possibility of brain herniation through the defect. They are most commonly seen in children less than 3 years of age and very infrequently seen in adults [6, 7]. They occur most commonly through linear fractures in the parietal region [8]. Clinical features range from gradually progressive scalp swelling to intractable refractory seizures [1, 8]. The time of onset of clinical symptoms from the initial impact varies from days to years, however symptoms developing within 3–4 days from impact are rarely seen [8].
Wang et al [9] described two cases of leptomeningeal cysts with symptomatic onset within 10 days of trauma. However, both these cases had evidence of raised ICP from the outset. Prasad et al [8] in a retrospective review of 43 cases reported the mean duration of onset of symptoms from the initial trauma to be 3.34 months (range: 2 days–24 months) and mean interval from symptom onset to surgical repair to be 11.6 months (range: 1 week–15 years). Diyora et al [10] in a series of 11 cases found the mean duration of onset to be 11 months (range: 2 weeks- 4 years).
Clinical Presentation
A 2-year female child who had a history of fall from a height of approximately 14 feet, was received in the casualty intubated with a GCS of E1VtM3. The child was moving all limbs and both the pupils were reactive to light. An NCCT was performed on presentation which showed the presence of a left fronto-parietal linear fracture with left fronto-parietal SDH. Presence of left MCA infarct with a midline shift of 2mm was also noted [Fig. 1. (a)(b)]. However, at presentation there was no clinical evidence of scalp swelling. The child was admitted in the Intensive Care Unit for observation. On day 4 post trauma, the presence of a left parietal scalp swelling was noticed, which was soft, non-pulsatile, non-erythematous and with well-palpable fracture edges. An MRI brain was performed for definitive diagnosis, as an NCCT scan alone has been said to be unreliable in differentiating cephalhematoma from an early onset GSF [11]. The MRI showed the presence of a traumatic left fronto-parietal bone fracture with acute brain herniation through the bony defect [Fig. 1(c)]. The decision was made to operate the patient to repair the defect.
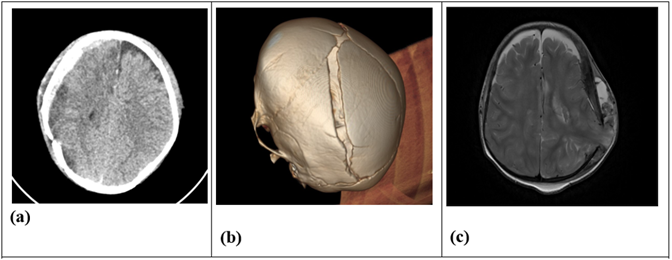
Figure 1: (a) shows the axial NCCT scan and the (b) 3D CT scan at presentation; (c) show the axial T2 MRI scan on day 4 post trauma.
Operative Details
A linear left fronto-parietal incision, going across the visible scalp swelling was made. After retraction of the skin flap, the linear bony defect was appreciated and herniating brain tissue was seen without the dural covering [Fig. 2(a)]. Four burr-holes were made adjacent to the bony defect and craniotomy completed. A small extra dural hematoma was found which was evacuated. The herniated brain was found too actively pulsating and viable. In view of the young age of the patient, the large volume of the herniated brain tissue and the brain viability the decision was taken to not sacrifice the herniated portion of the brain tissue. The
dural edges were defined. Gentle probing was done to release the subdural collection at the durotomy margins. The herniated tissue was gently reduced and watertight dural closure done using a pericranial patch [Fig. 2(b)]. Autologous split Cranioplasty was then used to cover the bony defect [Fig. 2(c)(d)]. The wound was then closed in layers after leaving a sub-galeal drain in situ. The post-operative NCCT showed resolution of the herniation and no other significant changes as compared to the the pre-operative scan [Fig. 2(e)]. The child was tracheostomized and was discharged on post-operative day 8 in the E2VtM3 state.
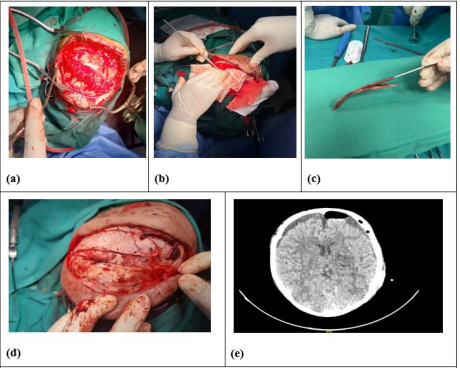
Figure 2: (a) shows the brain tissue herniation through fracture defect after skin incision; (b) shows reduction of herniated brain tissue; (c) (d) using autologous split cranioplasty for bony reconstruction; (e) post-operative NCCT
GSF’s are important complications of pediatric skull fractures that must be diagnosed as early as possible in order to permit early surgical repair in the form of duraplasty. Acute onset GSF’s can be confused with cephalhematoma. They can be distinguished by careful clinical examination as well as with doppler ultrasound which would show an absence of blood flow in case of a cephalhematoma. However, MRI is the gold standard for diagnosis as it can delineate the dural defect and show the site of brain herniation. Early recognition of GSF is of paramount importance as dural repair can prevent future neurological complications like seizures etc.
Ethics declarations
Ethics approval and consent to participate:
All procedures in this study were performed in accordance with the ethical standards of the institution, based on the 1964 Declaration of Helsinki and its later amendments. The parents of the presented patient provided written informed consent to participate in this study.
Consent for publication
The parents of the presented patient consented to the publication of her data.
Conflict of interest
The authors declare that they have no conflicts of interest.
Authors and their contributions:
Het Shah, Sarvesh Goyal, Raj Ghoniya wrote the main manuscript text. Praneeth Kokkula, Raj Ghoniya, Sarvesh Goyal, Het shah were the operating surgeons. Praneeth Kokkula, Raghav Singhla and Deepak Gupta reviewed and edited the manuscript. All authors reviewed the final manuscript prior to submission.
Funding: No funding was required.
Availability of data and materials: NA
Authors and affiliations:
Department of Neurosurgery: All India Institute of Medical Sciences, New Delhi, India.
Het Shah, Raj Ghoniya, Sarvesh Goyal, Raghav Singhla, Deepak Gupta, Praneeth Kokkula
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
