
Research Article | DOI: https://doi.org/10.31579/2690-1919/164
* VITROBIO Research Institute, Issoire, France.
*Corresponding Author: Ravi Shrivastava, VITROBIO Research Institute, Issoire, France.
Citation: Remi Shrivastava, Nathalie MANEBY, Ravi Shrivastava (2021). An Instant, Safe, Antihistamine, Anti-Inflammatory and Decongestant Polymeric Nasal Barrier to Prevent and To Treat Allergic Rhinitis in Children. J Clinical Research and Reports, 7(5); DOI:10.31579/2690-1919/164
Copyright: © 2021 Ravi Shrivastava, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 April 2021 | Accepted: 05 May 2021 | Published: 10 May 2021
Keywords: allergy; children; osmotic film; polymers; cytokine binding; clinical; chlorpheniramine; immunoglobulin; proinflammatory cytokines; immunosuppressant; solagum; histamine
Introduction: Allergic rhinitis (AR) in children is a common chronic pathology with a strong impact on patient quality of life. The main physiopathology affects the nasal cavity as a multi-factorial disease involving nasal mucosa damage, nasal inflammation with high concentrations of histamine, pro-inflammatory cytokines such as histamine, TNF-α, IL-4, IL-5, IL-6, IL-10, IL-13, and IgE antibodies on the nasal mucosa. Systemic entry of these proteins through damaged nasal mucosa maintains continued inflammatory and allergen cascades. Therefore, an ideal treatment should be multitarget in order to stop allergen exposure, inflammation, and nasal mucosa barrier degradation, but such treatments are nearly impossible to conceive. We envisaged an osmotic and protective nasal barrier film, not only capable of protecting the nasal mucosa from allergen exposure but also of trapping and neutralizing selected cytokines and cleaning the nasal surface continuously without using any harmful substance for children.
Materials and Methods: We associated highly osmotic glycerol solution with specific plant polymers to conceive an osmotic but stable film. As plant polymers (tannins) can bind with selective proteins, a range of glycerol binding non-cytotoxic polymers were screened using the sandwich ELISA method to select those having binding affinity for allergen induced nasal proinflammatory cytokines. After verifying cytotoxicity and irritant potential, a 15-day observational clinical study was performed with approval from the ethics committee on 30 children aged between 4-13, suffering from allergic rhinitis. The test product (TP) was supplied in 15-ml nasal sprays and applied 2-3 times per day for a period of 15 days. Saline solution served as control (CP). The scores of nasal and ocular symptoms, effect on quality of life, eosinophil count in nasal smears, and need for antihistamine treatment was evaluated at the start, at 30 minutes and on days 2, 3 and 15 of treatment.
Results: A few specific polymers were able to bind with selected cytokines and histamine at adequate filmogen concentrations. The osmotic film was stable, non-irritant and was able to clean the nasal mucosa continuously for 4-6h after each application. Clinical observations of Total Nasal Symptom Score (TNSS) grouping the scores of nasal congestion, runny nose, sneezing, and itching, revealed a strong decrease right after the 1st treatment in both groups but the reduction was much stronger and faster with the TP. The mean TNSS score reduction was 44.74% in CP vs 83.53% in the TP group after 7 days of treatment (p<0.001). Total Ocular Symptom Score (TOSS) was decreased by 21.13% and 51.41% in CP v/s 35.12 and 99.59% in TP group on days 2 and 7, respectively. Nasal smear eosinophil count was equally strongly reduced in the TP v/s CP group. No treatment-related side effects were recorded in any of the groups.
Conclusion: Protecting the nasal mucosa against allergens, neutralizing inflammatory cytokines, and keeping the nasal surface clean with an osmotic polymeric film, constitute a major breakthrough for the treatment of allergic rhinitis in children. This simple but scientific and logical approach should avoid exposing children to chemicals and to their long-term side effects.
Allergic rhinitis (AR) in children is a common pathology and the prevalence in industrialized countries is increasing very fast. Over 400 million people worldwide [1] adults and children, suffer from what is commonly called hay fever: itchy and runny nose, sneezing, nasal congestion, eye redness and swelling. Allergic rhinitis proportionally affects more children (40%) than adults (10%-30%) and causes irritability, sleep disorders and fatigue with negative impact on work performance and learning skills. Symptoms may start in early stages of life, as early as 18 months of age, and tend to gradually fade away after the age of 40 [2,3].
AR is triggered by airborne particles that are either naturally present in the environment, such as pollens, or issued from atmospheric pollution [4]. The allergic reaction occurs when the body’s immune system considers a common substance foreign and overreacts to defend the body. Nasal mucosa and airway epithelium of pre-sensitized children is extremely rich in allergen-presenting cells (APCs), called dendritic cells (DCs), which express receptors of innate immune system attracting immune cells such as mast cells with IgE receptors, basophils, neutrophils, T-lymphocytes, monocytes, and eosinophils. These cells release multiple allergenic mediators and proinflammatory cytokines, such as histamine, TNF-α, IL-4, IL-5, IL-6, IL-10, and IL-13 [5]. In pre-sensitized individuals, allergens are immediately recognized by antigen-specific immunoglobulin E (IgE) receptors on mast cells, triggering cell degranulation and histamine release. Severe nasal mucosa inflammation inflicts cellular damage, formation of gaps on nasal mucosal surface, increased vascular permeability, and symptoms of allergic rhinitis [6].
Being multifactorial, allergic rhinitis is very difficult to treat in children. Symptomatic relief may be obtained with topical or oral antihistamines and anti-inflammatory drugs, but these drugs are mono-target, cannot be used simultaneously, are mostly chemicals, have multiple side-effects and cannot help repair damaged nasal mucosa, an important factor for quick relief against allergens [7,8].
Taking into consideration long-term adverse effects of currently available chemical drugs and the absence of any multi-target treatment, nasal lavage with saline solution (0.9% NaCl) still constitutes one of the most favored anti-allergic treatments in children [9]. Cleaning the nasal surface with a safe and non-irritant solution helps to reduce the concentration of allergens, histamine, and inflammatory proteins on the nasal surface but lavage must be done frequently (every 3-4h) which is not practical in children. Frequently cleaning the nasal cavity with sea water containing up to 3.2% NaCl is also practiced but such solutions are very irritant when applied on the most sensitive organ in our body, and cannot be used frequently with ease, particularly in children [10,11]. Such hypertonic solutions form a temporary osmotic film on the nasal surface, attracting hypotonic liquid from the nasal tissues, and thereby minimizing the concentration of free-floating allergens and inflammatory particles [8].
We envisaged conceiving a multi-target, absorbent, non-irritant, osmotic, non-cytotoxic, and stable film which can be applied as a bandage on the nasal surface. Such a film could contain large polymeric molecules capable of trapping selected proinflammatory cytokines [12]. Osmosis should attract hypotonic fluid from the nasal tissue to create a strong continuous outward flow of liquid which should detach and drain any free-floating surface contaminants towards the film. The film should be able to absorb and/or trap the incoming impurities. The film could also act as a protective barrier on the nasal mucosa to stop allergen / pollutant contact with the sensitive nasal mucosa.
Combining these multiple anti-allergenic properties in a simple, mechanically acting osmotic film should prevent the progression of the disease, should minimize nasal inflammation and in consequence should help re-establish the natural barrier and defensive functions of the nasal mucosa. The conception and efficacy of such an anti-allergenic device for children is explained.
1. Ingredient for the conception of the osmotic film
The aim was to find a highly osmotic yet non-irritant filmogen base. After screening multiple natural and synthetic, osmotic, non-cytotoxic, and absorbent liquids, glycerol was selected as the most convenient filmogen base. Osmotic and nasal irritant potentials were determined in in vitro cell culture models [13] and by the bovine corneal opacity test (BCOP), as described by Schrage et al [14]. The glycerol film was rendered thick and absorbent by adding small quantities of a few commonly used food-grade thickenings agents.
2. Rendering the glycerol film resistant to osmosis-induced hypotonic liquid flow
Being osmotic, the glycerol solution attracted hypotonic liquid but was instantly diluted and lost its osmotic potential within a few minutes. Therefore, mechanical resistance of the osmotic film was improved by adding specific glycerol molecule binding inert polymers [12]. As specific polymers are known to bind with selected macromolecules (H, OH binding) and specific proteins, we identified those polymers, which can bind with glycerol molecules to render the glycerol film stable. Dual acting glycerol binding polymeric structures were further tested to evaluate their specific protein binding potential as described by Shrivastava et al [15].
3. Selecting histamine and allergy specific proinflammatory cytokine binding polymers:
Polymers, such as plant tannins, are very big molecules. After glycerol binding, many polymeric H and OH sites remain free. As tannin–protein binding is used to tan skin proteins and convert skin into leather, we used the same technology to evaluate polymeric affinity for proinflammatory cytokines present on allergen-induced inflamed nasal mucosa. The polymeric binding affinity of the key the proinflammatory cytokines, mainly histamine, IgE, TNF-α, IL-4, IL-5, IL-6, IL-10, and IL-13, was evaluated using ELISA tests at a fixed polymeric concentration of 0.10% in 5.0% glycerol aqueous solution. Test products were incubated with each purified human recombinant cytokine (Invitrogen, 400 pg/ml) for 5 minutes in phosphate buffer saline. The remaining free and available recombinant cytokine was measured using a specific ELISA kit (Thermo Fisher Scientific, Elisa kits for cytokines, thermofisher.com) according to the manufacturer's instructions. Recombinant cytokines without polymers were used as negative controls. The Optic Density (OD) was measured at 450 nm using an ELISA plate reader (luminometer-Envision, PerkinElmer).
Data analysis and interpretation: the scavenge activity of polymers is inversely proportional to the quantity of free cytokine detected. The reduction in quantified cytokine following incubation with polymers compared to the amount in negative controls, indicated the extent of cytokine neutralization due to polymeric binding.
Efficacy study
An observational clinical trial was conducted at Mudra Clinical Research, India in 2019 (ISO-14155 certified clinical research organization, Registration N° SQ18N02, dated 05/09/2018, renewed up to 04/04/2021). The protocol and study design were approved by the Institutional Ashirwad Ethics Committee, India (Reg.No. ECR/247/Inst/MH/2013/RR-16, dated 07/08/2018). The study was conducted in accordance with the “Declaration of Helsinki”, concerning medical research in humans (Brazil, October 2013), and following the ICH-GCP guidelines. Informed consent was obtained from all children / parents involved in the study. All subjects gave their informed consent for inclusion before they participated in the study. Being an observational study with a EU registered medical device containing exclusively food-grade ingredients and considering previous results of a closely similar formulae in adult population, CTR registration was not required.
1. Study design
The study was designed as a comparative, randomized, parallel group trial in 30 children, aged 3 to 14, and suffering from rhinitis of various origins, including city pollution generated symptoms of rhino-ocular allergy.
2. Patient selection
Main inclusion criteria were (1) children between 3 to 15, (2) suffering from acute episodes of recent allergic and / or pollution induced rhinitis, (3) with nasal and ocular manifestation of the disease, (4) having at least 6-month history of allergic rhinitis, (5) with positive Prick test or positive IgE test, (6) children / parents ready to follow the protocol and fill-out the daily questionnaire diary, (7) not under any antihistamine or anti-inflammatory treatment, and (8) not suffering from any chronic disease, nasal anatomical abnormality or other disease which may impact study parameters.
(9) Patients ready to abstain from using any drug which may affect study outcome. For ethical reasons, in case of worsening symptoms, only Cetirizine, the most used antihistamine drug was authorized to be prescribed by the physician. The prescriptions were recorded.
Main exclusion criteria included (1) not conforming to any of the inclusion criteria, (2) allergy to any of the test product ingredients, (3) unwillingness of the child/parent to participate or give written informed consent, (4) patients under immunosuppressant or having any abnormality of nasal cavity, respiratory diseases, or evidence of use of any steroid or antihistamine drug during the last 2-weeks.
3. Randomization
Treatments were allocated to patients by carrying out randomization using SAS Version 9.1.3. A biostatistician generated the randomization schedule. Block Randomization methodology was employed to follow 2:1 ratio for enrolling approximately 20 patients in the test product (TP) group and 10 in the control product (saline solution; CP) group.
4. Study objectives and parameters
The primary objective was to evaluate the change in mean score of Allergic Rhinitis Severity (ARS) symptoms including Total Nasal Symptom Score (TNSS), Total Ocular Symptom Score (TOSS), Non-Nasal/Eye Symptom Scores from baseline (start of treatment, BL) up to day 15 or up to the day of recovery (whichever earliest).
Secondary objectives included product safety profile, percentage of eosinophils in nasal smears, proportion of patients requiring antihistamines or other allergy medications, adverse events, and product acceptability. All parameters were evaluated 30-min after 1st treatment and on days 2, 7, and 15. Mean scores were compared with BL values and CP group scores, as appropriate. Mean scores were measured on a 1 (good) to 10 (worst) scoring scale at each time point.
5. Finished formulation and product application
The test formulation contained an association of glycerol with and dual acting polymers capable of binding with glycerol + cytokines and excipients. The finished formulation contained polymeric glycerol, allergen specific proinflammatory cytokine binding polymeric premix, jellifying and absorbent hydrophilic swelling agents, and excipients as described by Shrivastava et al. [15].
6. Statistical analyses
Statistical analysis was performed by unpaired two-tailed Student’s test for comparisons between the two groups and the one-way or two-way ANOVA followed by the post hoc Bonferroni’s test for comparisons of multiple groups. p<0.01 was considered statistically significant (GraphPad Prism version 8.4.2, La Jolla, USA).
1. Selection of osmotic solution:
The glycerol-polymer binding formed a highly adherent and osmotic film, capable of generating a strong osmotic flow of hypotonic liquid drawn from the tissues of the nasal mucosa. The hydrophilic thickening and jellifying substances added in film remained inert in glycerol solution but swelled immediately when in contact with incoming hypotonic liquid and rendered the glycerol film absorbent. The film was not irritant and stable for a minimum period of 4-6h. Application such a film on the nasal surface generated a strong osmotic liquid flow that enabled to continuously detach and drain nasal surface contaminants towards the film. These contaminants were then trapped in the absorbent polymeric film.
2. Polymeric binding with proinflammatory cytokines:
ELISA tests were conducted to find a polymeric association capable of binding with the eight key proinflammatory cytokines (histamine, TNF α, IL-4, IL-5, IL-6, IL-10, IL-13, and IgE) present in high concentrations on the nasal mucosa. The aim was to conceive a formulation which can bind and neutralize a maximum number of cytokines. As polymers are highly precise with respect to their protein-binding specificity and as the concentration of polymers incorporated must remain in acceptable quantities, hundreds of polymeric extracts were prepared using different techniques for polymer selection to prepare the finished formulation. Based on the initial screening results, Solagum (a polymeric association of Acacia and Xanthan gums), and three other polymers derived from Vaccinium macrocarpon fruit (Vma), Curcuma longa roots (Cl), and Panax ginseng roots (Pg) were found to bind and neutralize allergy specific cytokines at a concentration of (0.01%) which can be used to formulate the nasal spray. Solagum had a strong affinity for IL-10, IL-5, IL-13, IgE, and histamine but showed no binding with IL-6, IL-4 while Vma strongly neutralized only IL-6 (76%). Cl polymer was active against all the cytokines except for IL-5 while Pg had poor binding with IL-6, IL-10 and TNF-α (Fig.1).
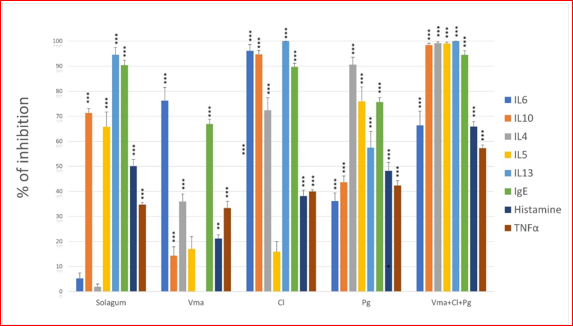
The association of these four polymers incorporated in the anti-allergy nasal spray was capable of binding and neutralizing up to 90% IL-10, IL-4, IL-5, IL-13, and IgE as well as nearly 60% IL-6, histamine and TNF- α.
3. Finished formulation and product application
The test product formulation therefore contained an association of glycerol Solagum, Vma, Cl, and Pg polymeric premix with hydrophilic film-thickening agents and excipients as described by Shrivastava et al. [15].
4. Clinical efficacy and safety study
Following the protocol established for the study (Protocol number: Aller/OBS/2018), the test product (TP) solution was filled in 15-ml sprays (about 130 sprays/vial) for nasal application and used as 2-3 pulverizations in each nostril, 2 to 3 times per day for a maximum period of 15 days. Identically filled 0.9% NaCl saline solution served as control product (CP). For young children, the treatment was applied by an adult or at least under adult supervision.
5. Disposition of patients
Data was collected on 10 patients (6 boys, 4 girls, mean age 7.7 years) in the CP group and 20 in the TP group (11 boys, 9 girls, mean age 8.9 years). All the patients enrolled completed the study.
6. Impact on the use of antihistamine drugs during the study
7/10 (70.0%) patients in the CP saline solution treated group had to take additional drugs to obtain further relief of allergy symptoms during the study, compared to only 1/20 (5.0%) patients in the TP group. Only the most commonly used antihistamine drug CETIRIZINE was recommended in case of strict necessity and average duration of treatment was 3.6 days. Doses employed were 5-mg/day taken orally for children above 6 years and 2.5mg/day for children below 6. Only one patient in CP group used Chlorpheniramine at a dose of 2mg taken orally 3 times per day for 4 days. The results obtained in the TP group show that the test product drastically reduces the need for antihistamines when treating allergic rhinitis symptoms.
As 70% of CP group patients used antihistamines, the impact of this treatment on other parameters must be considered while interpreting the data.
7. Effect on nasal symptoms scores (TNSS):
As the baseline TNSS of allergy rhinitis were quite similar in both groups (2.66 for TP v/s 2.64 for CP), at the start of treatment. Compared to baseline, the mean values of TNSS decreased strongly in TP on day 2 (-36.46±0.55%), day 7 (-75.56±0.33%) and had nearly completely disappeared by day 15 (-96.24±0.15%). Surprisingly, saline solution treated CP group patients equally showed a marked reduction in mean TNSS on day 2 (-21.97±0.38%), day 7 (-43.94±0.34%) and day 15 (-70.45±0.24%) (Fig.2).

Individual symptoms scores show that rhinorrhea and sneezing did not much improve in either group after the first dose of treatment. This is certainly due to the osmotic action of both products, which induce nasal discharge. However, these symptoms strongly improved on day 7 (rhinorrhea -73.24% and sneezing -66.67% in TP group v/s -42.11% and -42.11% in CP group). Congestion and itching symptom scores started receding in both groups just 30 minutes after first treatment. The effect on congestion and itching was particularly strong on day 2 in TP group (-59.38% in TP vs -49.41% in CP). Results of TNSS show that TP and CP have a similar mode of action, but the TP’s effects are faster and stronger. TP superiority is probably related to the fact that the TP contains glycerol which exerts a stronger osmotic pressure compared to an isotonic saline solution. Secondly, due to polymeric binding, the glycerol solution forms a film resistant to the mechanical pressure exerted by outflowing hypotonic liquid, with continuous cleaning effects for a period of 4-6h. As the allergens and proinflammatory cytokines are continuously cleaned from the nasal mucosa, recovery is faster compared to the treatment of CP.
8. Effect on ocular symptoms scores (TOSS)
In the nasal-ocular reflex, allergens in the nose stimulate inflammatory mediators, which in turn stimulate the trigeminal ganglion leading to ocular vasodilatation, erythema, plasma leakage, and tearing. In both groups, the ocular symptom scores were quite similar at the time of recruitment, except for eye swelling which was lower in the TP group. For unbiased comparison of total mean scores between both groups, an adjustment value of 0.525 was added to all the mean values in CP group.
Compared to baseline, the mean TOSS scores in the CP group started decreasing significantly by day 2 (-21.13±0.52%), day 7 (-51.41±0.32%), with maximum reduction by day 15 (-71.83±0.22%). These results show that nasal lavage with a saline solution every 4-6h also helps improve ocular symptoms of allergic rhinitis. These effects are probably due to frequent elimination of nasal surface allergenic impurities which should minimize allergic and inflammatory cascades.
In the TP group, the reduction of TOSS was even stronger and faster as the mean reduction compared to BL was -35,12±0.58%; -75.21±0.37%; and up to -99.58±0.05% on days 2, 7, and 15, respectively (Fig.3).
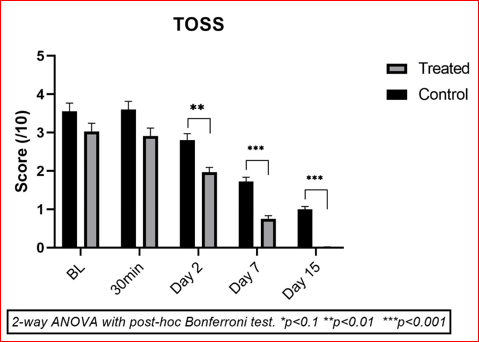
Taking into consideration the reduction of TNSS as well as TOSS, the higher efficacy of the TP on the symptomatic manifestation of AR is evident.
9. Impact on overall Quality of Life (QOL):
QOL parameters included effect on thirst, sleep quality, irritability and feeling of well-being in children suffering from allergic rhinitis. These parameters were scored at the start of treatment (BL) and on day 1 (30 min after 1st dosing), 2, 7, and 15 on a 0 (excellent) to 10 (worst) scoring scale for each child. A reduction of mean values compared to the BL scores reflects improvement in quality of life. In a healthy patient having excellent quality of life, this score should be close to 0. The mean QOL score at the start of treatment was 4.50±1.28 in the CP group and 4.06±1.43 in the TP group. To compare both groups identically, a compensation value of 0.4375 was deducted from all the mean scores obtained during the treatment period in CP group. Based on this calculation, there was no difference between the two groups on day 1 but a reduction of 0.48/10 on day 2 and 1.08/10 on day 7 were recorded in the TP group vs CP (Fig.4).
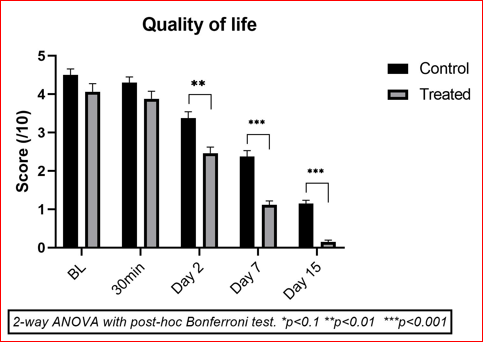
At the end of the study (day 15), mean scores in both groups were very low indicating a better QOL in both groups (mean 1.15/10 in CP vs 0.39/10 in TP).
10. Nasal eosinophil smears:
The mean scores of eosinophil count were nearly identical in both groups at BL (14.1 in the CP group v/s 14.65 in TP group). All the patients enrolled in the study were positive for the presence of eosinophils in nasal smear indicating that the cause of rhinitis was certainly allergic as eosinophils are directly associated with pathogenicity of allergic rhinitis. At the end of the treatment period (day 15), the mean eosinophil count was 10.3 in the CP group compared to 4.55 in the TP group. These results show the efficacy of the test product in eosinophil reduction on the nasal mucosa. The number of children showing positive results (<9 eosinophils) was 7/10 in the CP group compared to only 2/20 in the TP group. This drastic reduction in eosinophil count reveals reduced allergic activity on the nasal mucosa surface, which can be attributed to the filmogen protection offered by the test product.
11. Adverse events:
A few patients in both groups had occasional headache, temporary excitation, and hyperactivity but these patients already had such problems before the start of the study and these events were found in both groups (5 in TP group, 2 in CP group). Therefore, these events are not considered to be related to the use of the test or comparator products. No other adverse event was recorded during the study, indicating that both comparator and test products are safe for use in children.
12. Overall product assessment:
Saline solution and the test product were both well tolerated and favorably assessed by patients and by the investigator. Regular washing of the nasal cavity using saline solution helps remove allergens and reduces symptoms of allergy. The duration and doses of an antihistamine treatment can be reduced by regular nasal application of saline solution. This is an important benefit for limiting the use of these drugs in children. Nevertheless, any use of antihistamines induces side effects and allergic rhinitis is a chronic disease that will reappear after each exposure to allergens. Therefore, the very good results obtained with the test product underline the excellent safety profile (no side effect) and efficacy of the product in treating allergic rhinitis in children. 85% of patients (or parents) assessed the test product as being very good to excellent.
The more we keep our children in a clean environment, the less they are exposed to foreign particles and the less their immune defense system is solicited. The argument that too-clean environments contribute to allergies is called the hygiene hypothesis [16]. Generally, childhood exposure to germs and infection helps to build the immune system because the immune system recognizes these “foreign particles” and has already developed defense mechanisms to protect the body. Not only does a too-clean environment put children at risk of later developing allergies and asthma, but the chemicals used to clean the environment might themselves be responsible for such disorders during adulthood. This is probably the reason why the incidence of allergy and asthma is increasing more in developed and clean countries, Japan for example [17], compared to developing and less clean countries such as India [18]. According to the International Study of Asthma and Allergies in Childhood [19], the global prevalence of wheezing was estimated to be 11.6% for 6–7-year-old children and 13.7% for 13–14year-old children for the period between 2001–2003. Wheezing is particularly prevalent in English-speaking and Western countries. The prevalence of parent-reported doctor-diagnosed allergy and asthma among 6–7-year-old children is 10.8%, with lower rates in Northern and Eastern Europe (4.5%), and the highest rates in North America (20.0%), western Europe and Oceania (29.2%) [20].
Furthermore, recent studies show a direct link between allergen and pollution induced rhinitis and the development of more serious pathologies like asthma[21]. When clinical symptoms appear, the disease pathology has already progressed with nasal mucosa damage, gaps on the nasal mucosa allowing systemic entry of allergens and cytokines, activation of the inflammatory and allergic cascades, severe nasal inflammation, presence of multiple proinflammatory cytokines on the nasal surface, and ocular inflammation due to connection between eye and nose through nasolacrimal duct [10,22,23]. This physiopathology continues up to the time the child is exposed to allergens or pollutants. Being a multi-factorial disease, only a multi-target treatment can provide relief but all currently available treatments, except for nasal lavage with saline solution, are mono target as they are usually directed to block histamine or to suppress inflammation [24,25]. These drugs are chemicals, have multiple short and long-term side effects, must be taken regularly, and can neither offer protection against allergens nor clean the nasal surface of allergens [25,26].Unfortunately, the allergic reaction continues if exposure to allergen/pollution and inflammatory cascades are not stopped, and if gaps on the nasal mucosa are not repaired. An intact and healthy nasal mucosa barrier can defend itself against most foreign substances. As allergy is a long-term disorder and as the immune cells conserve allergen memory over many years [27] the treatment must be totally safe for repeated and long-term use.
We conceived a protective, nasal surface cleaning, and anti-inflammatory film solution which simply cleans the nasal surface through osmosis and helps to minimize the concentration of free-floating toxic molecules from the surface. The film acts as a physical barrier to prevent allergen contact with the nasal mucosa and attracts nasal surface contaminants towards the film through its osmotic properties. Being absorbent, the film traps bigger molecules while the smaller particles can cross the film and be expelled through natural nasal flow. As polymers are big and inert molecules, we incorporated dual-acting polymeric molecules in the osmotic solution which imperatively bind with glycerol molecules to render the glycerol film stable for 4-6h and also with selected proteins, such as inflammatory cytokines and histamine. The selected polymers are derived from food-grade vegetable substances to avoid cellular interactions and potential cytotoxicity.
By attracting liquid from the inner parts of the mucosa, the test product mechanically cleans away contaminants, foreign particles and other undesired inflammatory proteins present on the nasal surface. This creates an ideal environment for cell growth, mucosa repair and restores the natural barrier function of the nasal mucosa. The results of the clinical study clearly show that simple cleaning the nasal surface 4-5 times per day with saline solution remarkably reduces the clinical manifestation of allergic rhinitis. These results should be interpreted carefully as 90% patients in this group required cetirizine treatment for a short duration, which must have influenced the clinical outcome of this treatment. In contrast, only 5% children in the test product group required antihistamine therapy with superior overall clinical efficacy compared to the saline solution controls. This better efficacy of the test formulation compared to the saline solution can be attributed to the four key properties of the test product (1) formation of a long-term preventive barrier on the nasal surface which minimizes allergen contact with the nasal mucosa, (2) 4-6h nasal mucosa osmotic cleaning effects against only a few minutes with the saline solution, (3) absorbent properties of the film due to the presence of jellifying substances, and (4) presence of allergy-specific protein-binding polymers in the film capable of trapping and neutralizing most of the incoming proinflammatory cytokines and histamine. Such treatment can therefore be considered as a multitarget approach, acting as an invisible anti-allergen mask, antihistamine, anti-inflammatory and nasal mucosa repairing device, particularly adapted for repeated use in children. The device can also be used as a preventive measure by applying a few sprays of the product before anticipated exposure to allergens or pollutants or as a device to minimize symptomatic manifestation of the disease in clinically affected individuals. As evident from the topical mode of action of the test product and the clinical observations of this study, this therapy does not restrict use of any systemic drug such as antihistamine drugs.
The use of a polymeric physical or mechanical nasal barrier to protect the nasal surface against allergens is recent and lacks clinical data for comparison. Completing the data obtained in this study by conducting clinical trials on other polymeric compositions for different topical and systemic inflammatory protein related diseases would bring pertinent information regarding the validity of this treatment approach. Several other diseases involving multiple proteins such as cytokines, histamine, and MMPs have no efficient treatments. Polymers being inert, safe and highly specific protein-antagonists, can be used to conceive a new class of polymeric antiviral[28], anti-MMP [29], and anti-CGRP drugs of the future.
Allergic rhinitis is a triggering factor for multiple respiratory diseases, such as asthma, in children. Regular and continuous use of antihistamines and anti-inflammatory drugs induce long-term side-effects and degrade the quality of life of children. A nearly instant, totally safe, histamine and cytokine neutralizing, and allergen protecting film which can replace or at least minimize the use of chemical drugs, represents a great therapeutic advancement. Further large scale clinical trials are recommended to fully validate or refute the hypothesis of using polymers as future drugs.
AR Allergic Rhinitis
TNF Tumor Necrosis Factor
IL Interlukine
IgE Immunoglobulin E
ELISA Enzyme-Linked Immunosorbent Assay
TP Test Product
CP Control Product
TNSS Total Nasal Symptom Score
TOSS Total Occular Symptom Score
APC Allergen Presenting Cell
DCs Dendritic cells
NaCl Sodium Chloride
BCOP Bovine Corneal Opacity Test
OD Optic densit
ICH GCP International Conference on Harmonisation-Good Clinical Practice
EU European Union
CTR Clinical Trial Registration
ARS Allergic Rhinitis Severity
BL Baseline
Vma Vaccinum macrocarpon
Cl Curcuma longa
Pg Panax ginseng
QOL Quality of Life
MMP Matrix Metalloproteinases
CGRP Calcitonin Gene-related Peptide
This clinical study was commissioned and funded by VITROBIO SAS, France.
The data presented in this study are available on request from the corresponding author.
The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
