
Research Article | DOI: https://doi.org/10.31579/2642-9756/214
1Department of Obstetrics and Gynecology, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria.
2Department of Obstetrics and Gynecology, Nnamdi Azikiwe University, Awka, Anambra State, Nigeria
3Department of Psychiatry, Leicestershire Partnership NHS Trust, Leicester, United Kingdom.
4Department of Obstetrics and Gynecology, Alex-Ekwueme Federal University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria.
*Corresponding Author: Chigozie Okafor
Citation: Citation: Chigozie Okafor, Martin C. Andeh, Chigozie G. Okafor, Chukwunonso I. Enechukwu, Samuel O. Umeononihu, et al, (2024), An Audit of Maternal Mortality in A Tertiary Hospital in Nigeria: A 5-Years Retrospective Review, J. Women Health Care and Issues, 7(5); DOI:10.31579/2642-9756/214
Copyright: Copyright: © 2024, Chigozie Geoffrey Okafor. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 July 2024 | Accepted: 24 July 2024 | Published: 02 August 2024
Keywords: maternal mortality; maternal mortality ratio; direct causes; trend; live birth
Background: Maternal mortality is a key measure of the health of a nation. Globally, maternal mortality has been on the decline, but this is not true for the sub-Saharan African region.
Objectives: To investigate the trends in maternal mortality, identify the background socio-cultural factors, and establish the major causes of maternal deaths.
Materials and Methods: This was a five-year retrospective cross-sectional study of all cases of maternal deaths in Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi, Nigeria, from January 1, 2017 to December 31, 2021. We retrieved data for maternal deaths, number of live births and other relevant obstetrics information from the medical record department of the hospital to provide relevant information. The data were analysed using SPSS statistical software version 25 (IBM, Armonk, NY, USA).
Results: Of 3538 live births, 29 maternal deaths were recorded. The mean age of the women was 29.36 ± 4.79 years. The maternal mortality ratio (MMR) for the period under review was 820 per 100,000 live births. There were annual fluctuations in MMR. The highest ratio of 1297 per 100,000 live births was recorded in 2020. The majority of the deaths, 26 (89.7%), occurred among the unbooked women that were referred from peripheral hospitals and maternity homes as obstetric emergencies. The direct causes of maternal death accounted for 86.2% of the deaths. The major causes of death were obstetric haemorrhage (31%), pre-eclampsia/eclampsia (27.6%), and sepsis (13.8%). The majority of the cases (79.3%) died within twenty-four hours of hospital admission.
Conclusion:
Maternal mortality ratio is still high in Nigeria, the major causes are largely preventable, and this could be achieved through preventive initiatives such as combined safe motherhood strategies. There is a need for intensive advocacy, awareness, and sensitization programmes aimed at early referral and prompt intervention to reduce maternal mortality and morbidities.
The World Health Organization (WHO) defines maternal death as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from unintentional, accidental, or incidental causes [1].
Maternal mortality is a serious public health concern, especially in the sub-Saharan Africa region, of which Nigeria is part. It suffers the highest maternal mortality worldwide, with a high maternal mortality ratio of 553 maternal deaths per 100,000 live births, or 200,000 maternal deaths a year. This translates to 68 percent of all maternal deaths worldwide2. These deaths are unacceptable, as the majority of them are preventable.
About 35% of maternal deaths worldwide in 2017 occurred in Nigeria (23%), and India (12%) alone [3]; with Nigeria having the highest number of maternal deaths worldwide3. According to the World Bank collection of development indicators, the MMR of Nigeria is 917 (per 100,000 live births) [3]. The lifetime risk of a Nigerian woman dying during pregnancy, childbirth, postpartum, or post-abortion is 1 in 22, in contrast to the lifetime risk in developed countries, which is 1 in 4900 [4].
High maternal mortality witnessed in Nigeria can be linked to the three forms of maternal delay proposed by Thaddeus and Maine5, which include delay in making a decision to seek care, delay in locating and arriving at a medical facility, and delay in receiving skilled pregnancy care [5]. This is evidently influenced by the socioeconomic and political context as seen in our health care system And the cultural and biological realities of many Nigerian women seeking healthcare [6].
Maternal mortality is not only a health issue but also a crucial indicator of a nation's development and progress in achieving Sustainable Development Goals (SDGs), particularly SDG 3 (Good Health and Well-being) and SDG 5 (Gender Equality). In highlighting the specific issue in sub-Saharan Africa, particularly Nigeria, is important because of disproportionate burden of maternal mortality in this region compared to the global trend. Therefore, understanding why declines in maternal mortality have not been realized in this context is crucial for targeted interventions.
This study is aimed at assessing the trends in maternal mortality and progress thus far in achieving Sustainable Development Goal (SDG) target 3.1: reducing global MMR to less than 70 per 100,000 live births by 2030, in Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi, south-east Nigeria, over a 5-year period.
Study Design
This was a 5-year retrospective cross sectional study of all cases of maternal death among women delivered in NAUTH, Nnewi, Nigeria, from January 1, 2017 to December 31, 2021
Study population
The study was conducted among women who died while giving birth in NAUTH, Nnewi, Nigeria, within the study period
Study settings
Over a five-year period, from January 1, 2017, to December 31, 2021, the study was carried out in the obstetrics sections of Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi, South East Nigeria. The facility is a 400-bed tertiary hospital supported by the Federal Government of Nigeria and offers first-rate emergency obstetrics and gynaecology care round the clock. It acts as a referral facility for adjacent states in addition to offering specialised services to the host community and the entire state. The hospital acts as a training institution for undergraduate and postgraduate medical education. As a training institution, it has a large number of consultants, junior and senior resident doctors, and other supporting medical staff.
Inclusion criteria
This included all the pregnant women that died during pregnancy, delivery, or within 42 days of termination of pregnancy, irrespective of gestational age or site of the pregnancy, but not due to accidental or incidental causes within the study period.
Exclusion criteria: pregnant women who died due to accidental or incidental causes.
Sampling Technique and Sample Size Determination
A non-random sampling methodology was employed as the sampling strategy. All available cases of maternal deaths during the study period were studied.
Study procedure
The records department's already-separately stored maternal mortality case files made retrieval easier. The labour ward, intensive care unit, gynaecological ward, lying in ward, and accident and emergency unit registrations were used to identify cases. The following information was gathered: patient residence, booking status, age, marital status, religion, education level, occupation, gravidity, parity, date and time of hospital admission until death, and cause of death as stated in the patient case note. A tally-numbering system was used to manually analyse the collected data. Frequencies, percentages, averages, standard deviations, and charts for categorical variables were used to summarise the data. The hospital's ethical committee gave the research its ethical approval.
All data analysis in this study was conducted using SPSS Statistics version 25 (IBM Corp., Armonk, NY, USA). The data were assessed for normal distribution using Shapiro–Wilk tests. Normally distributed data were analyzed using independent-sample t-tests; the values were presented as mean ± SD. Categorical data were analyzed using the chi-squared test or Fisher exact test and results are expressed as n (%).
During the study period, from January 1, 2017 to December 31, 2021, case files of maternal deaths were reviewed. The majority of the women belonged to the 26–35-year-old age group (68.9%), with a mean age of 29.36 ± 4.79 years. A significant number of the women had a parity of 1–4 (65.5%). Most of the women were married (75.9%). Twenty-one (72.4%) women had completed secondary education. The majority of the patients were from rural areas (69%), while 31% were urban dwellers. Out of the 29 maternal deaths, 26 (89.7%) of the women were unbooked. This is shown in Table 1.
| Variable | Options | Frequency n (%) |
| Age (years) | 16-20 21-25 26-30 31-35 36-40 >41 | 2 (6.9) 4 (13.8) 11 (37.9) 9 (31.0) 2 (6.9) 1 (3.4) |
| Marital status | Not Married Married | 7(24.1) 22(75.9) |
| Parity | 0 1-4 >5 | 8(27.6) 19(65.5) 2(6.9) |
| Level of Education | None Primary Secondary Tertiary | 0 2(6.9) 21(72.4) 6(20.7) |
| Occupation | Trading Civil service Student House wife | 13(44.8) 3(10.3) 7(24.1) 6(20.7) |
| Patient location | Rural Urban | 20 (69.0) 9 (31.0) |
| Booking status | Booked Unbooked | 3 (10.3) 26 (89.7) |
Table 1: Sociodemographic Characteristics of study population (n=29)
Table 2 shows the yearly variation of maternal mortality, live birth, and MMR. There was a total of 29 maternal deaths over the study period that occurred among 3538 live births between 2017 and 2021, giving an average MMR of 820 per 100,000 live births. The majority of the maternal deaths occurred in 2020. The annual live birth versus maternal mortality trend and the trend of the maternal mortality ratio are shown in Figures 2 and 3. MM = Maternal Mortality, MMR = Maternal Mortality Ratio
| Year | Live Birth | MM | MMR per 100,000 |
| 2017 | 878 | 6 | 683 |
| 2018 | 693 | 4 | 577 |
| 2019 | 818 | 6 | 734 |
| 2020 | 617 | 8 | 1297 |
| 2021 | 532 | 5 | 940 |
| TOTAL | 3538 | 29 | 820 |
Table 2: shows the yearly variation of maternal mortality, live birth and MMR.
The causes of maternal mortality in the years during the study period are shown in Table 3. The most common cause of maternal mortality was obstetric haemorrhage, which accounted for 31.0% of direct maternal deaths. Unsafe abortion (3.4%) and thromboembolism (3.4%) were the least common causes of direct maternal death, respectively. Other recorded causes included pre-eclampsia (27.6%), sepsis (13.8%), and uterine rupture (6.9%). Maternal anaemia, anaesthetic complications, and HIV encephalopathy were responsible for indirect maternal deaths during the study period. This is shown in Table 3.
| Causes of death | Frequency (n=29) | Percentage |
| Direct causes | ||
| Obstetric Haemorrhage | 9 | 31.0 |
| Pre-eclampsia/eclampsia | 8 | 27.6 |
| Sepsis | 4 | 13.8 |
| Ruptured Uterus | 2 | 6.9 |
Unsafe Abortion Thromboembolism | 1 1 | 3.4 3.4 |
| Indirect causes | ||
| Anaemia | 2 | 6.9 |
| Anaesthesia | 1 | 3.4 |
| HIV encephalopathy | 1 | 3.4 |
Table 3: shows the causes of maternal mortality in the years under review.
Table 4 shows the interval from hospital presentation to maternal death. Regrettably, the majority of maternal deaths (79.3%) occurred within less than 24 hours of presentation in the hospital, while 20.7% occurred after 24 hours of presentation.
| VARIABLE | DURATION | PERCENTAGE % |
| ≤24 Hours | 23 | 79.3 |
| >24Hours | 6 | 20.7 |
Table 4: Illustrating the duration of Hospital stay before death
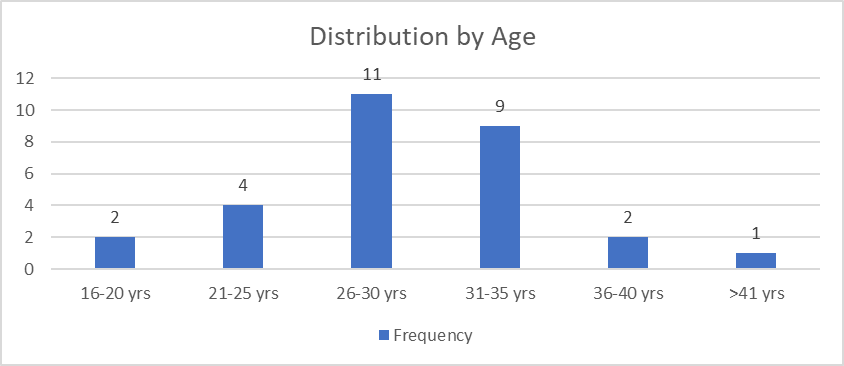
Figure 1: shows the distribution of maternal mortality according to age.
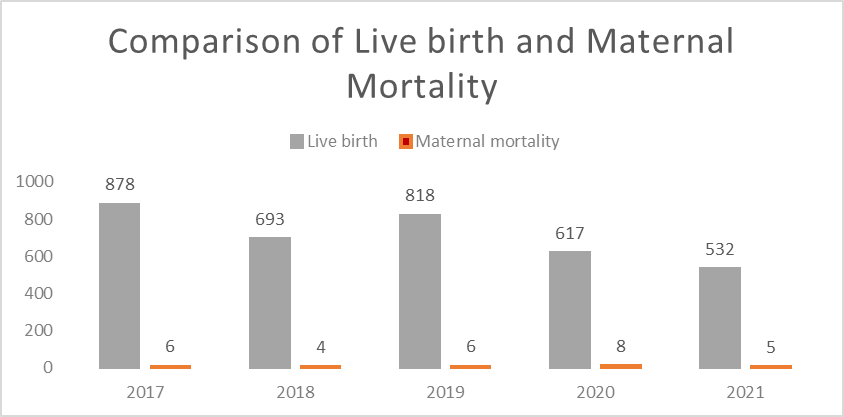
Figure 2: shows the annual live birth vs. maternal mortality trend
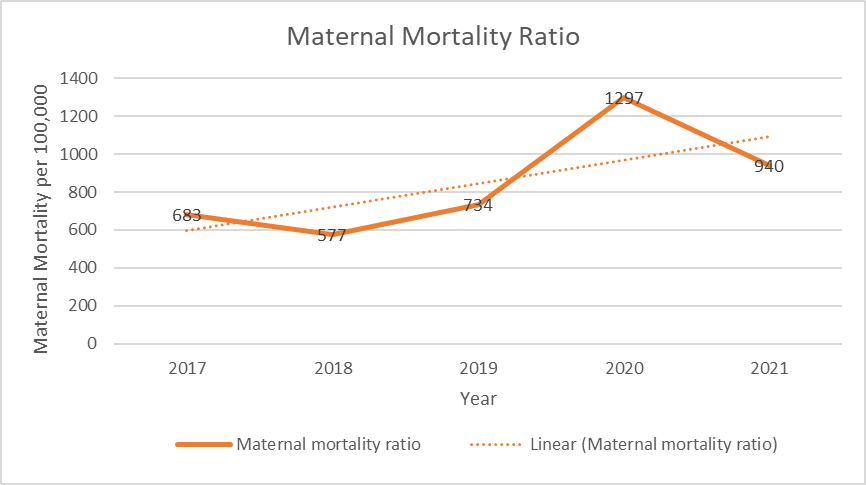
Figure 3: shows trend of maternal mortality ratio
The principal findings from the study showed the maternal mortality ratio (MMR) for the period under review was 820 per 100,000 live births with a mean age of 29.36 ± 4.79 years. The highest ratio of 1297 per 100,000 live
births was recorded in 2020. The majority of the deaths occurred among the unbooked patients. Direct causes accounted for 86.2% of maternal deaths. Obstetric haemorrhage remains the leading cause of maternal death in our study. Regrettably, the majority of the deaths occurred within twenty-four hours of hospital admission.
From the study, the high MMR for the period under review of 820 per 100,000 live births was close to the WHO estimated MMR of 814 per 100,000 live births for Nigeria [6,7]. It is lower than some earlier studies done in Nigeria [8,9] and higher than that reported from south-south Nigeria [10]. The high MMR reported is not unexpected, as NAUTH is a tertiary hospital, with the majority of the women being referred from other peripheral hospitals with severe complications requiring more specialised care. However, more work has to be done to achieve the related Sustainable Development Goal.
In this study, it was noteworthy that there was a rapid increase in MMR in 2020 and 2021 of 1297 per 100,000 live births and 940 per 100,000 live births, respectively, and these observations could be due to the COVID-19 pandemic, industrial strike actions by health workers, and a shortage of manpower with respect to the work load that was prevalent during that period.
The majority of maternal deaths occurred between the ages of 26 and 35, with a mean age of 29.36 ± 4.79 years, and this is similar to studies done in Nigeria and sub-Saharan African countries [8,11-13]. However, lower age ranges of 20–30 years were seen in studies done in northern Nigeria, [14,15] and this could be attributed to early marriage that is peculiar to those regions. The early deaths of these women, aged 26–35, will have a huge negative impact on the immediate family and, inadvertently, on society at large.
The majority of maternal mortality occurred among unbooked women, with 89.7% showing poor health-seeking behaviour, and this finding was similar to earlier studies done in Nigeria [8,9,11,14,15]. Maternal death from this study showed that 65.5% of the women had parity of one to four, while primigravida make up 27.6% and grand multiparous women 6.9%. This finding was similar to other studies in Nigeria [8,11]. Although grand multiparous women may have a higher chance of maternal death from increasing maternal medical conditions and obstetric haemorrhage, this shows the need to protect and be watchful of every pregnant woman regardless of her parity.
The direct causes of maternal mortality contributed 86.2% of maternal deaths, while indirect causes contributed 13.8% in this study. These were also in keeping with the causes of maternal deaths in developing countries [8,9,11,14,15]. In contrast to developed countries, where indirect causes were the major cause of maternal deaths [16,17].
The major causes of maternal mortality in this study were obstetric haemorrhage (31%), pre-eclampsia/eclampsia (27.6%), and sepsis (13.8%). The leading cause of maternal mortality was obstetric haemorrhage, as also seen from most studies in developing countries [12]. These causes are preventable if our women readily assess appropriate antenatal, intrapartum, and postpartum care from skilled healthcare providers. However, some studies from northern Nigeria have reported Pre-eclampsia/eclampsia as the leading cause of maternal death [14,15].
The major indirect causes of maternal death were anaemia (6.9%), anaesthesia (3.4%), and HIV encephalopathy (3.4%). Anaemia is the major cause of indirect maternal death in this study, and this is similar to some previous studies in Nigeria [8,11,14]. However, some studies in Nigeria found HIV to be the leading indirect cause of maternal mortality [15]. Anaemia could be attributed to poor utilisation of antenatal services, poor nutritional status, infections, infestations, and increased demand from repeated pregnancies.
The majority of the maternal deaths in this study occurred in the first 24 hours of hospital stay (79.3%), and this is similar to studies from tertiary hospitals in Nigeria [12,14]. This is due to the late presentation, as most cases are often brought in a very bad state from the community and lower health facilities with poor referral systems. Prompt referral will go a long way in reducing maternal deaths.
Our study has a number of clinical implications: First, the high MMR, particularly among unbooked women referred from peripheral hospitals and maternity homes, underscores the importance of early and comprehensive antenatal care. Healthcare providers should focus on identifying high-risk pregnancies early and providing appropriate interventions to prevent maternal complications. Second, the fact that the majority of maternal deaths occurred among women referred as obstetric emergencies highlights the critical need for improved access to emergency obstetric care. This includes timely access to skilled healthcare providers, emergency obstetric services, and blood transfusions to manage obstetric hemorrhage, pre-eclampsia/eclampsia, and other complications. Third, the finding that the majority of maternal deaths occurred within twenty-four hours of hospital admission underscores the importance of timely referral and prompt intervention. Efforts should be made to strengthen referral systems, improve communication between peripheral health facilities and referral hospitals, and ensure that women receive timely and appropriate care upon arrival at the hospital. Fourth, the annual fluctuations in MMR highlight the need for continuous monitoring of maternal health indicators and ongoing quality improvement initiatives. Healthcare facilities should regularly review maternal death audits, identify areas for improvement, and implement strategies to address gaps in care delivery. Lastly, community education and awareness programs are essential to empower women with knowledge about the importance of antenatal care, the signs and symptoms of obstetric complications, and the need for timely access to healthcare services. These programs can help reduce delays in seeking care and improve maternal outcomes.
The significant limitation of this study is that it is a retrospective study with associated average to poor documentation of some of the relevant information sought. The findings from this study could form the basis for development of a data quality score for each hospital for maternal mortality statistics, which could be used to inform policy.
This study showed that there has been an increase in MMR in 2020 and 2021. The majority of causes of maternal mortality are preventable, and this could be achieved through combined safe motherhood strategies of quality antenatal care, community mobilisation and health education, prompt referral, active management of labour and the immediate postpartum period, and access to family planning. There is a need for intensive advocacy, awareness, and sensitization programmes targeted at private hospitals and maternity homes for early referral, as most cases in this study were brought into a very bad state and died within 24 hours of hospital admission.
There is a need for political will to provide extensive health insurance coverage to offer free quality antenatal, intrapartum, postpartum, and family planning services. There is also a need for proper record keeping and regular interval evaluation of appropriate indicators to measure progress on maternal mortality reduction programmes towards achieving Sustainable Development Goal (SDG) target 3.1.
The authors are grateful to all the study participants whose information was used for the study and to the NAUTH hospital staffs that participated in the study.
This retrospective review has not been submitted to any journal for publication. The conceptualization, design, writing, and critical editing of the article, data collection, and analysis were all greatly aided by the efforts of each author. The submission of this work to a journal for consideration was approved in full by the authors.
The authors received no external funding for the work
The authors declare no conflict of interest.
Ethical clearance for the study was sought and obtained from the Nnamdi Azikiwe University Teaching Hospital (NAUTH) ethics review committee on July 5, 2022, with approval reference number NAUTH/CS/66/VOL.15/VER.3/106/2022/066. The research was conducted according to ethical principles for human scientific research according to the Helsinki Declaration.
This is not applicable as this is a retrospective study.
This is not applicable.
HIV = Human Immunodeficiency virus
MMR = Maternal Mortality Ratio
NAUTH = Nnamdi Azikiwe University Teaching Hospital
SDG = Sustainable Development Goal
WHO = World Health Organisation
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
